Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Exponential Smoothing of Postponement Rates in Operation Theatres of Advanced Pediatric Centre - Time Series Forecasting With Regression AnalysisDocument7 pagesExponential Smoothing of Postponement Rates in Operation Theatres of Advanced Pediatric Centre - Time Series Forecasting With Regression AnalysisInternational Jpurnal Of Technical Research And Applications100% (2)
- Aesthetics of The Triumphant Tone of The Black Woman in Alice Walker's The Color PurpleDocument30 pagesAesthetics of The Triumphant Tone of The Black Woman in Alice Walker's The Color PurpleInternational Jpurnal Of Technical Research And Applications100% (2)
- Energy Gap Investigation and Characterization of Kesterite Cu2znsns4 Thin Film For Solar Cell ApplicationsDocument4 pagesEnergy Gap Investigation and Characterization of Kesterite Cu2znsns4 Thin Film For Solar Cell ApplicationsInternational Jpurnal Of Technical Research And Applications100% (1)
- Pod-Pwm Based Capacitor Clamped Multilevel InverterDocument3 pagesPod-Pwm Based Capacitor Clamped Multilevel InverterInternational Jpurnal Of Technical Research And ApplicationsPas encore d'évaluation
- Qualitative Risk Assessment and Mitigation Measures For Real Estate Projects in MaharashtraDocument9 pagesQualitative Risk Assessment and Mitigation Measures For Real Estate Projects in MaharashtraInternational Jpurnal Of Technical Research And ApplicationsPas encore d'évaluation
- Effect of Trans-Septal Suture Technique Versus Nasal Packing After SeptoplastyDocument8 pagesEffect of Trans-Septal Suture Technique Versus Nasal Packing After SeptoplastyInternational Jpurnal Of Technical Research And ApplicationsPas encore d'évaluation
- Evaluation of Drainage Water Quality For Irrigation by Integration Between Irrigation Water Quality Index and GisDocument9 pagesEvaluation of Drainage Water Quality For Irrigation by Integration Between Irrigation Water Quality Index and GisInternational Jpurnal Of Technical Research And ApplicationsPas encore d'évaluation
- Implimentation On Distributed Cooperative Caching in Social Wireless Network (Swnet)Document4 pagesImplimentation On Distributed Cooperative Caching in Social Wireless Network (Swnet)International Jpurnal Of Technical Research And ApplicationsPas encore d'évaluation
- Production of Starch From Mango (Mangifera Indica.l) Seed Kernel and Its CharacterizationDocument4 pagesProduction of Starch From Mango (Mangifera Indica.l) Seed Kernel and Its CharacterizationInternational Jpurnal Of Technical Research And Applications100% (1)
- Performance Analysis of Microstrip Patch Antenna Using Coaxial Probe Feed TechniqueDocument3 pagesPerformance Analysis of Microstrip Patch Antenna Using Coaxial Probe Feed TechniqueInternational Jpurnal Of Technical Research And Applications100% (1)
- 1V DSP in Wireless Communication SystemsDocument4 pages1V DSP in Wireless Communication SystemsInternational Jpurnal Of Technical Research And ApplicationsPas encore d'évaluation
- Effect of Welding Process and Post Weld Heat Treatments On Microstructure and Mechanical Properties of Aisi 431 Martensitic Stainless SteelDocument6 pagesEffect of Welding Process and Post Weld Heat Treatments On Microstructure and Mechanical Properties of Aisi 431 Martensitic Stainless SteelInternational Jpurnal Of Technical Research And ApplicationsPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- 5070 s14 QP 11Document16 pages5070 s14 QP 11OsamaRahimPas encore d'évaluation
- Celltac MEK 6500Document3 pagesCelltac MEK 6500RiduanPas encore d'évaluation
- Hotel Elizabeth in Baguio City: Address: J Felipe Street Cor. Gibraltar Road Mines View Park, Baguio City, PhilippinesDocument16 pagesHotel Elizabeth in Baguio City: Address: J Felipe Street Cor. Gibraltar Road Mines View Park, Baguio City, PhilippinesI amEllaPas encore d'évaluation
- 15 UrinalysisDocument9 pages15 UrinalysisJaney Ceniza تPas encore d'évaluation
- Evidence-Based Strength & HypertrophyDocument6 pagesEvidence-Based Strength & HypertrophyAnže BenkoPas encore d'évaluation
- Written Assignment Unit 4 Health ScienceDocument6 pagesWritten Assignment Unit 4 Health SciencesafsdaPas encore d'évaluation
- Section IIDocument8 pagesSection IIapi-471272376Pas encore d'évaluation
- Supercritical Carbon DioxideDocument3 pagesSupercritical Carbon DioxideRawda SeragPas encore d'évaluation
- Teleperformance Global Services Private Limited: Full and Final Settlement - December 2023Document3 pagesTeleperformance Global Services Private Limited: Full and Final Settlement - December 2023vishal.upadhyay9279Pas encore d'évaluation
- Estrogen Dominance-The Silent Epidemic by DR Michael LamDocument39 pagesEstrogen Dominance-The Silent Epidemic by DR Michael Lamsmtdrkd75% (4)
- 1 A Finalexam FNH330 June 2015 Final Review QuestionsDocument6 pages1 A Finalexam FNH330 June 2015 Final Review QuestionsChinley HinacayPas encore d'évaluation
- Plastic Omnium 2015 RegistrationDocument208 pagesPlastic Omnium 2015 Registrationgsravan_23Pas encore d'évaluation
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- The Preparation of Culture MediaDocument7 pagesThe Preparation of Culture MediaNakyanzi AngellaPas encore d'évaluation
- 48V 100ah LiFePO4 Battery Spec With CommunicationDocument6 pages48V 100ah LiFePO4 Battery Spec With CommunicationsoulmuhPas encore d'évaluation
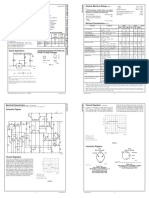
- LM 337Document4 pagesLM 337matias robertPas encore d'évaluation
- Method of Toxicity Test 1Document59 pagesMethod of Toxicity Test 1Widya AnggrainiPas encore d'évaluation
- Silly VersesDocument29 pagesSilly Verseskevin dalePas encore d'évaluation
- 351 UN 1824 Sodium Hydroxide SolutionDocument8 pages351 UN 1824 Sodium Hydroxide SolutionCharls DeimoyPas encore d'évaluation
- Cuts of BeefDocument4 pagesCuts of BeefChristopher EnriquezPas encore d'évaluation
- An Enhanced Model of Thermo Mechanical Loading On A Vaccum Insulated GlazingDocument29 pagesAn Enhanced Model of Thermo Mechanical Loading On A Vaccum Insulated GlazingNguyễn SơnPas encore d'évaluation
- BDC 6566Document6 pagesBDC 6566jack.simpson.changPas encore d'évaluation
- Laboratory Medicine Internship BookletDocument95 pagesLaboratory Medicine Internship BookletMuhammad Attique100% (1)
- Lesson Plan On Tuberculosis (Health Talk)Document8 pagesLesson Plan On Tuberculosis (Health Talk)Priyanka Jangra100% (2)
- KL 4 Unit 6 TestDocument3 pagesKL 4 Unit 6 TestMaciej Koififg0% (1)
- Product Term and ConditionsDocument50 pagesProduct Term and Conditionsain2Pas encore d'évaluation
- TFU-Risk Assessment RA-11 - Use of Grooving & Threading MachinesDocument1 pageTFU-Risk Assessment RA-11 - Use of Grooving & Threading Machinesarshin wildanPas encore d'évaluation
- ESR 2538 ChemofastDocument14 pagesESR 2538 ChemofastEduardo Antonio Duran SepulvedaPas encore d'évaluation
- Intraocular Pressure and Aqueous Humor DynamicsDocument36 pagesIntraocular Pressure and Aqueous Humor DynamicsIntan EkarulitaPas encore d'évaluation
- Epoxy Data - AF35LVE TDS - ED4 - 11.17Document8 pagesEpoxy Data - AF35LVE TDS - ED4 - 11.17HARESH REDDYPas encore d'évaluation