Académique Documents
Professionnel Documents
Culture Documents
A Practical Guide To Head Injury Rehabilitation by Michael (Dec 31, 2013)
Transféré par
HadaAtiyehTitre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
A Practical Guide To Head Injury Rehabilitation by Michael (Dec 31, 2013)
Transféré par
HadaAtiyehDroits d'auteur :
Formats disponibles
A Practical Guide to Head
Injury Rehabilitation
A Focus on Postacute Residential
Treatment
CRITICAL ISSUES IN NEUROPSYCHOLOGY
Series Editors
Antonio E. Puente
UniversilY oJ North Carolina, Wilminglon
Current Volumes in this Series
AGING AND NEUROPSYCHOLOGICAL ASSESSMENT
Asenath La Rue
Cecil R. Reynolds
Texas A & M UniversilY
BEHAVIORAL INTERVENTIONS WITH BRAIN-INJURED CHILDREN
A. MacNeil Horton, Jr.
BRAIN MECHANISMS IN PROBLEM SOL VING AND INTELLIGENCE:
ALesion Survey of the Rat Brain
Robert Thompson, Francis M, Crinella, and Jen Yu
BRAIN ORGANIZA TION OF LANGUAGE AND COGNITIVE PROCESSES
Edited by Alfredo Ardila and Feggy Ostrosky-Solis
HANDBOOK OF HEAD TRAUMA: Acute Care to Recovery
Edited by CharIes J, Long and Leslie K. Ross
HANDBOOK OF NEUROPSYCHOLOGICAL ASSESSMENT:
A Biopsychosocial Perspective
Edited by Antonio E, Puente and Robert J, McCaffrey
NEUROPSYCHOLOGICAL EVALUATION OF THE SPANISH SPEAKER
Alfredo Ardila, Monica Rosselli, and Antonio E, Puente
NEUROPSYCHOLOGY, NEUROPSYCHIATRY, AND BEHAVIORAL
NEUROLOGY
Rhawn Joseph
THE NEUROPSYCHOLOGY OF ATTENTION
Ronald A, Cohen
THE NEUROPSYCHOLOGY OF EPILEPSY
Edited by Thomas L. Bennett
A PRACTICAL GUIDE TO HEAD INJURY REHABILITATION:
A Focus on Postacute Residential Treatment
Michael D, Wesolowski and Amie H. Zencius
A Continuation Order Plan is available for the series, A continuation order will bring delivery of
each new volume immediately upon publication, Volumes are billed only upon actual shipment.
For further information, please contact the publisher.
A Practical Guide to Head
Injury Rehabilitation
A Focus on Postacute Residential
Treatment
Michael D. Wesolowski
Flvrida Department oj Health and
Rehabilitation Services
Miami, Flvrida
and
Arnie H. Zencius
Premier ojChicago Rehabilitation Center
Downers Grove, Illinvis
Springer Science+Business Media, LLC
Llbrary of Congress Cataloglng-ln-Publlcatlon Data
Wesolowski, Michael O.
A practical guide to head injury rehabilitation: a focus on
postacute residential I Michael O. Wesolowski and Arnie H.
Zencius.
p. cm. -- (Critical issues in neuropsychology)
Includes bibliographical references and index.
1. Brain damage--Patients--Rehabilitation. 2. Behavior therapy.
I. Zencius. Arnie H. 11. Title. 111. Series.
[ONLM: 1. Brain 1njuries--rehabilitation. 2. Behavior Therapy.
3. Socioenvironmental Therapy. 4. Caregivers--psychology. WL 354
W514p 1993J
RC387.5.W47 1993
617.5'1044--dc20
DNLM/OLC
for Library of Congress
ISBN 978-1-4757-8993-5 ISBN 978-1-4757-8991-1 (eBook)
DOI 10.1007/978-1-4757-8991-1
1994 Springer Science+Business Media New York
Originally published by Plenum Press, New York in 1994.
Softcover reprint of the hardcover 1 st edition 1994
All rights reserved
93-30642
CIP
No part ofthis book may be reproduced, stored in a retrieval system, or transmitted
in any form or by any means, electronic, mechanicai, photocopying, microfilming,
recording, or otherwise, without written permission from the Publisher
Foreword
Behavioral neuropsychology presents at once achallenge and an opportunity
for the field ofbehavior analysis. A great diversity of problem areas-including
education, classroom management, child rearing, retardation, and industry-
have been treated effectively by the behavior analytic approach, which has
traditionally and quite deliberately chosen to deemphasize physiology and
cognitive variables. Yet brain injury, by its nature, entails neurological insult
that is often closely related to specific cognitive dysfunctions. The challenge
for behavior analysis is to develop effective treatments for a disorder with
such clearly defined tripartite characteristics. The opportunity exists for be-
havior analysis to expand its conceptual basis as well as to provide benefits
to patients otherwise despairing of assistance. Case histories demonstrate over
20 years of successful applications of behavior analysis to brain-injured in-
dividuals, indicating that some applications are possible, but are these reports
notable exceptions or the harbingers of a new general therapeutic approach?
The present book describes an overall focused behaviaral program far
dealing with the diversity of brain injury problems in a general brain injury
rehabilitation setting. The authors describe what types of neurological damage
are associated with specific types of cognitive/emotional dysfunction and in
turn with specific types ofbehavioral dysfunction, thereby demonstrating how
the choice ofbehavioral treatment is guided by the neurological and subjective
assessment. The result is a conceptually unified approach.
The distinctive value of this book lies in the detail as well as the pro-
grammatic guidelines for actual implementation ofthis behavioral approach.
Applications to groups as well as to individuals are described. General guide-
lines for treatment staff are clearly stated, illustrated with case examples, and
even include instructions for training the treatment staff and mantaining staff
competence and motivation. Programs are designed for typical behavior
problems caused by brain injury, such as aggression, noncompliance, social
v
vi FOREWORD
skills deficits, and inappropriate sexual behavior. Similarly, behavioral pro-
grams are described for many of the cognitive/emotional sequelae of brain
injury, such as attention and memory deficits, impulsivity, orientation deficits,
lack of self-awareness, and difficulties in problem solving.
The authorspresent valuable outlines and forms to facilitate standardized
implementation. Exemplary references to published studies, many by the au-
thors, attest to the validation of the procedures described. Especially note-
worthy and valuable are the guidelines for the program staff to implement
treatment continuously during the day outside of formal classes by the use
of incidental teaching methods of instruction. The programs presented include
remediation of the cognitive/behavioral deficits, but also correction of the
disruptive behaviors that otherwise make the educational process unfeasible.
Behavioral neuropsychology is a newly emerging field. The authors have
described an overall program using this approach that enables professionals
in this field to leam the specific details sufficient to establish their own program.
From the results obtained, this behavioral approach is emerging as the clear
treatment of choice, and this book makes an invaluable contribution in de-
scribing the manner of its implementation.
Nathan H. Azrin
Nova University
Fort Lauderdale, Florida
Preface
Advances in medical technology have increased the survival rate and longevity
of individuals who, just a few years ago, would have died from their injuries.
Saving a person's life is of paramount importance after a serious injury. We
now know, however, that once saved, we must help the injured person to live
a life with quality. We also know that following most head injuries, even mild
ones, survivors often exhibit long-term, often lifelong, changes in personality,
cognition, and behavior.
Over the past decade, professionals have attempted various techniques
to overcome barriers created by head trauma. This book presents an approach
to head injury rehabilitation, first recognized by Arthur M. Horton, called
behavioral neuropsychology. That is, the application of behavioral principles
to the study and rehabilitation ofindividuals with brain injury. Although the
approach is not new, we have detailed some behavioral techniques that have
not been tried and experimentally evaluated approaches that have no sup-
porting data. Despite the diversity oftopics we present using behavioral neu-
ropsychology, the reader should know that we believe in using an interdis-
ciplinary team approach that indudes the dient, rehabilitation professionals,
and the family. It is hoped that in the 1990s, advances in postacute head
injury rehabilitation will parallel those in medical care.
This book is concerned with the inpatient, postacute rehabilitation of
individuals who have suffered traumatic brain injury. That is, we are presenting
behavioral techniques that we have found to be effective within the residential
rehabilitation center. This is not to say, however, that these approaches should
not be attempted in the other environments, e.g., horne, work, or school. It
is through such attempts that practitioners and researchers can demonstrate
generalization oftreatment effects we found valuable in the residential setting.
We would like to express our gratitude to William Burke, Mark Guth,
and Richard Zawlocki for the ideas generated in the lively discussions during
VB
viii PREFACE
the Monday night "research meetings" at the Knight House. Many of those
ideas led to the data-based studies presented in this book. We would like to
acknowledge the efforts of many direct care staff, among whom are Fred
Doubleday, Pat McQuade, and Paul Mahoney, who collected data and con-
tributed in many other ways. We are especially thankful to Susie Badgley for
her work on this manuscript. Without her help, this book could never have
been completed. We also appreciate the efforts of Eliot Werner of Plenum
Press and Antonio Puente, Series Editor of Critica! Issues in Neuropsycho!ogy,
for their advice and assistance.
Michael D. Wesolowski
Arnie H. Zencius
Contents
Foreword by Nathan H. Azrin .......................... v
Chapter 1
Introduction
Epidemiology ............................................. 1
The NYU Cognitive Retraining Model ........................ 3
The Hawaii State Hospital Model ............................. 4
The Behavioral Neuropsychological Approach .................. 5
Summary............................................. ... 7
Chapter 2
Applied Behavior Analysis 11
Identification and Measurement ofTarget Behaviors ............. 12
Measuring Behavior . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Duration Recording . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Latency Recording . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Interval and Momentary Time Sampling ..................... 17
Trials to Criterion ....................................... 18
Number of Prompts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Graphing Data ............................................ 19
Performing a Functional Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
IX
x
CONTENTS
Empirical Evaluation ....................................... 23
The Reversal (A-B-A-B) Design ........................... 23
Multiple Baseline Designs ................................. 24
Alternating Treatments Design ............................. 26
Summary................................................ 28
Chapter 3
Developing the Rehabilitation Plan 31
Evaluation in the Natural Environment ........................ 32
The Client in the Natural Environment ........................ 32
Formal Clinical Assessments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Situational Evaluation ...................................... 39
Final Outcome ............................................ 44
Summary ................. ,.............................. 48
Chapter 4
The Daily Routine 51
Designing Routines of Daily Living ........................... 52
Components of Daily Living ..... . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Evaluation ofthe Daily Routine ............................ 53
Developing Teaching Opportunities in the Daily Routine. . . . . . . . 55
Component Descriptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Community Meeting ....................................... 56
Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Teaching Opportunities ................................... 56
Types ofTeaching Interactions ............................. 57
Development of Teaching Competence ........................ 58
Relating Individual and Group Routines ....................... 60
Summary................................................ 61
Chapter 5
Staff Training 63
CONTENTS
Tutorial Processes
Guiding Observation .................................... .
Modeling ............................................. .
Coaching ............................................. .
Observing and Giving Feedback ........................... .
Participating in the Daily Routine ......................... .
Teaching Clients with Brain Injury ........................... .
Guiding the Observation of Clients ......................... .
Modeling for Clients .................................... .
Reinforcing Clients ..................................... .
Recognizing Teaching Opportunities ....................... .
Management of Staff Development .......................... .
Summary ............................................... .
Chapter 6
Procedures for Cognitive Problems
Xl
63
64
65
66
67
69
70
71
71
72
73
74
76
79
Memory Loss ............................................. 79
Cognitive Retraining ..................................... 80
Compensatory Strategies .................................. 86
Orientation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
Orientation Groups ...................................... 96
Individual Orientation Sessions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Attentional Deficits ........................................ 99
Attentional Training Strategies ............................. 100
Self-Awareness ............................................ 105
Assessing Self-Awareness .................................. 106
Treating Denial ......................................... 106
Problem-Solving Deficits .................................... 110
Problem-Solving Groups .................................. 1 10
Problem-Solving Vignettes ................................ 111
Flow Sheets ............................................ 112
Current Events Groups ................................... 112
Scheduled Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 113
Planning Disorders ........................................ 113
Planning Groups ........................................ 114
Planning Checklists ...................................... 115
Repeated Exposure ...................................... 116
Current Events Groups ................................... 117
Summary ................................................ 117
xii CONTENTS
Chapter 7
Procedures for Behavior Problems
121
Noncompliance ........................................... 121
Consequence Management ................................ 122
Antecedent Control Techniques ............................ 129
Aggression ............................................... 132
Causes of Aggression ..................................... 132
Treatment of Aggression .................................. 134
Inappropriate Sexual Behavior ............................... 140
Dating Skills Training .................................... 143
Scheduled Feedback . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 144
Transfer ofStimulus Control .............................. 145
Self-Monitoring ......................................... 146
Behavior Contracting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 147
Interpersonal Skill Deficits .................................. 149
Social Skills Training ................................... .. 151
Point Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 152
Contingent and Scheduled Feedback ........................ 154
Preteaching . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 157
Group Psychotherapy .................................... 158
Impulsivity ............................................... 158
Treatment ofImpulsivity ................................. 158
Summary ................................................ 163
Chapter8
Procedures for Health and Medical Problems 167
Using Assistive Devices ................................. ;... 167
Consequence Management ................................ 168
Antecedent Control Techniques ............................ 168
Operant Seizures .......................................... 169
Hypochondriacal Statements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 173
Bulimia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 174
Obesity .................................................. 176
Diabetes ................................................. 178
Summary ................................................ 178
CONTENTS XIll
Chapter 9
The Role of the Family 181
Family Reactions to Head Injury ............................. 181
The Injured Individual ................................... 182
Family Dynamics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 182
Severity of Injury ........................................ 182
Stages ................................................. 183
Transfer to Postacute Settings ................................ 184
Special Issues, Roles, and Players ............................. 184
Emotion ............................................... 184
Preexisting Issues ........................................ 185
Maladaptive Roles ....................................... 185
Marital Issues ........................................... 185
Y oung Adults . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 186
Siblings ................................................ 186
Children ............................................... 186
.................................... 187
Primary Caregivers ...................................... 187
Discharge .............................................. 188
Assessment ............................................... 188
Goals ................................................. 188
Methods ............................................... 189
Family Services: Intervention/Integration ...................... 190
Assumptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 190
Education ............................ . . . . . . . . . . . . . . . . .. 191
Horne Visits ............................................ 192
Support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 193
Professional Support ..................................... 194
Respite Care ............................................ 194
Advocacy .............................................. 194
Family Therapy ......................................... 194
Support versus Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 195
Intimacy ............................. . . . . . . . . . . . . . . . . .. 195
Summary ................................................ 196
Appendix A: Performance Analysis ...................... 199
Appendix B: Practitioner Forms for Memory .............. 201
xiv
CONTENTS
Appendix C: TBI Education.Curriculum .................. 213
Appendix D: Social Skills Curriculum .................... 223
Appendix E: Horne Trip Observation Scale . . . . . . . . . . . . . . .. 227
References .......................................... 231
Index .............................................. 237
1
Introduction
The human brain, suspended in fluid, protected by a tough layer of tissue
called the dura mater, and enclosed in a bony vault, is nevertheless exposed
to numerous affiictions including trauma, tumors, vascular accidents, infec-
tion, attack from toxic substances, and demyelinating and degenerative dis-
eases. Weshalllimit our discussion to trauma.
EPIDEMIOLOGY
Head injuries in the United States and in all industrialized nations are
frequent. The National Head Injury Foundation (NHIF) estimates that over
1 million persons each year sustain injuries in accidents severe enough to
require hospitalization, and from this group, 30,000-50,000 persons have
such serious intellectual or behavioral dysfunction that they are unable to
return to a normallife. Further, the majority ofhead injuries occur in persons
under the age of 30 (NHIF, 1992).
These rather conservative estimates are, nonetheless, much higher than
the annual incidence of persons with other better known neurological disorders
such as multiple sclerosis, cerebral palsy, muscular dystrophy, and tumors.
Tuerk, Fish, and Ransohoff (1975) estimate that vehicular accidents account
for three million head injuries each year in the United States, including 750,000
concussions, 150,000 skull fractures, and 150,000 significant brain injuries.
The National Institute of Neurological and Communicative Disorders
and Stroke has estimated the annual cost of care for head-injured patients in
the United States at three billion dollars (NINCDS, 1976). This calculation
does not include personal costs or the economic cost to the nation in terms
of lost income. Thus, despite some difficulty in obtaining reliable statistics,
there is ample evidence that brain injury as a result of trauma is a problem
2 CHAPTER 1
of great magnitude and one that may have reached epidemic proportions in
the United States.
Much has been written about the early management ofhead injury and
about the recent medical and technical advances that contribute to the life-
saving capacities ofhospital trauma centers (Bakay & Glasauer, 1980; Cartlidge
& Shaw, 1981; Jennett & Teasedale, 1981). These authors deal with emergency
treatment, early assessment, methods of monitoring, medical and cognitive
sequelae, and prognosis after severe head injury. Despite the thorough coverage
ofthe acute phases ofhead injury management, comparatively little attention
has been devoted to the rehabilitation phase of treatment (Horton & Wedding,
1984). Perhaps this is a result of a pessimistic belief prevalent in some circles
that brain injury is irreversible and that organic patients should be warehoused
and lucky to be alive. Within the last 10 years, however, there has emerged
a considerable body of experience that lends more optimism to the prognosis
for clients with brain injury. This chapter will review a few ofthe models for
rehabilitation of clients with brain injury. Chapter 2 presents an overview of
applied behavior analysis. Chapter 3 focuses on the rehabilitation planning
process. Chapter 4 outlines how to use the daily routine to teach clients with
brain injury. Chapters 5 presents ideal methods of staff training in rehabili-
tation facilities for individuals with brain injury. Chapters 6, 7, and 8 provide
some of the evidence supporting our optimism regarding rehabilitation of
individuals with brain injury. Chapter 9 presents some ideas on the role of
the family in head injury rehabilitation, including assessment techniques and
strategies to reintegrate the head-injured survivor into the family.
Persons with traumatic brain injury usually suffer from multiple problems
that require the services of several different rehabilitation disciplines, including
medicine, speech therapy, neuropsychology, physical therapy, occupational
therapy, social work, and vocational counseling. These clients suffer from
severe changes in motor, communicative, social, behavioral, and cognitive
abilities.
Clinical neuropsychologists and other rehabilitation specialists who en-
gage in retraining the brain-injured client in the cognitive and behavioral
areas are focusing, of course, on the relatively specific band of problems within
a much broader spectrum of difficulties. The ultimate goal of the various
rehabilitation services is to facilitate the process of recovery of an individual
toward the restoration of full physical, social, and vocational capabilities.
In the past, much more attention was given to restoring physical function
and to regaining speech rather than dealing with the behavioral consequences
ofbrain damage or to the relation ofthese sequelae to social reintegration in
the community. Today, however, rehabilitation efforts must encompass the
domains of behavior management, cognitive retraining, family education,
and vocational planning. The individual with brain injury presents serious
INTRODUCTION 3
problems requiring tremendous expenditures of time, skill, energy, and re-
sources on the part of aB members of the rehabilitation team.
THE NYU COGNITIVE RETRAINING MODEL
Although there are several existing programs of cognitive retraining in
rehabilitation centers throughout the United States, there is only a limited
body of clinical practice on which to base program development. In addition,
there are only a few models of cognitive retraining available at the present
time. The first model we shall explore is one used at the New York University
Institute of Rehabilitation Medicine.
Ben-Yishay, Diller, and other faculty at NYU have pioneered a program
of delivering systematic intervention to traumatically brain-injured clients in
the perceptual, cognitive, and interpersonal domains. Intervention consists
of five training modules administered in the following order: (1) an orientation
module (ORM) that deals with attentional deficits; (2) an eye-hand integration
with finger dexterity hierarchy (DEX); (3) a perceptual-cognitive integration
constructional task hierarchy (CON); (4) a visual information processing task
hierarchy (VIP); (5) a verbal logical reasoning task hierarchy (LOG). The
training modules are administered to individuals uniformly, for 20 consecutive
weeks. The number ofmodules and the rate ofprogress, however, are tailored
to the person's ability to reach a plateau on each module.
In addition to the cognitive training modules, NYU clients are involved
in group training (social skills), community activities, personal counseling,
and upon completion of the 20 consecutive weeks, prevocational explorations,
and eventually, vocational placements.
The eligibility criteria are specific and include such items as an IQ of at
least 80, independence in self-care and ambulation, unsatisfactory vocational
and educational rehabilitation prior to entry, a minimum of 12 months since
the trauma, and motivation for rehabilitation (Ben-Yishay, 1981). Since per-
sons with a history ofbehavioral problems, alcohol and drug abuse, and aphasic
and dysarthric problems are excluded from entry, the trainees are an elite
group for rehabilitation.
The cognitive remediation modules themselves represent a hierarchy of
tasks or training packages along three substantive continua, namelyattention
demand: from basic arousal (ORM) to maximal concentration (LOG); generic
function: from simple psychomotor functions (DEX) to ideation and problem-
solving (LOG); and a locus of interaction: from external stimulus-response
processing (ORM) to almost total internal algorithms (LOG). A task qualifies
as a cognitive remediation task ifby training in it, the brain-injured individual
will correct, or at least significantly ameliorate, underlying deficits anywhere
4 CHAPTER I
along the entire range of the cognitive domain, i.e., arousal and attention,
psychomotor, perceptual, cognitive-verbal, and cognitive-emotive functions
(Ben-Yishay, 1981).
Repetition of a task, however, will not, in and of itself, remediate the
generic or core deficit. Diller (1976) suggested some ways a task can be modified
for therapeutic gain. Each includes the speed and number of items presented;
the sensory modality in which the problem is presented; the number of spatial
dimensions as well as concreteness, size, color, familiarity, and complexity.
In addition, other critical dimensions include the speed of response and du-
ration of effort required, the amount of information provided from alternative
sensory modalities, criteria for success, and amount of additional information
provided.
Obviously, although the modules are presented to the trainees in a uni-
form, fixed order, the staff are providing individuals with differing types of
brain damage different methods of instruction, feedback, and behavioral
monitoring during the retraining period. In asense, then, these carefully or-
chestrated training experiences are tailored for the individual client.
The NYU cognitive remediation modules represent a singular achieve-
ment in program development for brain-injured clients. The major shortcom-
ing, however, as noted by Satz and Fletcher (1981), is the consistent theoretical
framework for conceptualizing cognitive retraining. Diller and Gordon (1981)
acknowledge this difficulty in their review of intervention studies.
THE HAWAII STATE HOSPITAL MODEL
The Hawaii State Hospital program of cognitive retraining or "neuro-
training" has evolved over the past 15 years. Neurotraining is defined as "the
systematic application of psycho10gica1 and neurological principles for the
purposes of enabling individuals to overcome deficits that result from central
nervous system dysfunction" (Craine & Gudeman, 1981, p. 5). The procedures
are based on the data from neuropsychological test batteries for structuring
deficit-specific activities for neurotraining. Neurotraining is more concerned
with gaps in human performance than with specific lesions in the brain.
Craine and Gudeman (1981) discuss a number of principles for neuro-
training. The key principles are that they assume the plasticity of function
within the central nervous system and postulate that environmental stimu-
lation can facilitate learning. They further suggest that the activities of neu-
rotraining should follow a developmental sequence of learning. In addition,
the neurotraining approach assumes that the process of learning is more im-
portant than the specific content of any area. Moreover, they posit that con-
sistency and direct feedback are particularly important and that effectiveness
INTRODUCTION 5
of neurotraining can be linked to the degree that individual deficits can be
specified.
Neurotraining is administered on a one-to-one basis, tailored to the in-
dividual's needs, provided in step-by-step increments at regular intervals with
maximal stimulation and aimed toward successful, overlearned endeavors.
Training techniques are created as needed for individual clients. Although
clients with a history of alcohol and drug abuse or serious emotional problems
and clients with degenerative neurological disorders are not excluded, training
may be contraindicated in so me instances.
In planning for neurotraining, it is important to identify the functional
deficits via comprehensive neuropsychological assessment. The areas offunc-
tional deficits are categorized as attention, cognitive (abstraction, feedback,
organization, problem-solving, strategy, discrimination, flexibility, inhibition-
facilitation, memory), processing or coordination (laterality, multimodal,
perceptual-motor, sequencing, spatial-quantitative), and symbolic-Ianguage
(afferent, efferent). These may cut across the visual, auditory, tactile, taste-
smell, motor, and vestibular-proprioceptive modalities. Appropriate training
techniques are then selected to ameliorate the functional deficits. eraine and
Gudeman (1981) present 181 techniques that are graded on the basis oflevel
of difficulty, i.e., elementary, intermediate, and advanced.
Although neurotraining offers a philosophy of training and operates from
a deficit-specific rationale based on neuropsychological assessment, a consistent
theoretical framework for conceptualizing retraining is missing. The program
also suffers from the need for more systematic explication and more rigorous
validation.
THE BEHA V/ORAL NEUROPSYCHOLOG/CAL APPROACH
Neuropsychology is defined as the study ofbrain-behavior relationships.
Behavioral neuropsychology may be defined as the application of behavior
therapy to problems of brain-injured individuals while using neuropsycho-
logical assessment and intervention perspectives (Horton, 1981). This treat-
ment methodology suggests that inclusion of data from neuropsychological
assessment strategies would be helpful in the formation ofhypotheses regarding
antecedent conditions (extern al or intern al) for abnormal behavior. That is,
a neuropsychological perspective will significantly enhance the ability of the
behavior therapist to make accurate discriminations as to the etiology of client
behaviors. Moreover, the formulation of a cogent plan of therapeutic inter-
vention and its skillful implementation could be facilitated by an analysis of
behavioral deficits implicating impairment of higher cortical functioning
(Horton, 1979).
6
CHAPTER I
Stated simply, the radical behavioral model has been characterized by a
rejection ofunobservable variables (thoughts or images) as legitimate entities
in the functional analysis of human behavior. There is considerable wisdom
in carefully and objectively defining one's variables. It should be recognized,
however, that a possible unwarranted assumption ofthe radical behaviorist's
model is that all inferred variables are alike.
A contrary viewpoint would make distinctions between two types of
inferred variables. These would be intervening variables and hypothetical
constructs (Craighead, Kazdin, & Mahoney, 1981). Intervening variables are
theoretical creations. On the other hand, hypothetical constructs are usually
empirical or physical in function. The major advantage of a hypothetical
construct is that at some point, by some means, its existence or nonexistence
can be verified. At present, for example, methods for the direct, objective
verification of a thought or feeling have yet to be adequately developed. In
the future, however, this may not be the case; we may have this technology
(Wesolowski 8!- Deichmann, 1980; Wesolowski & Zawlocki, 1985).
Thus, it can be seen that because a neuropsychological perspective relies
on hypothetical constructs, the inclusion of a neuropsychological perspective
within a behavioral model has particular advantages. The worth of such a
perspective should not be underestimated. Indeed, cross-cultural research has
provided such impressive validation of neuropsychological insights that it
would be unwise to minimize their importance (Benton, 1979; Faglioni,
Spinnler, & Vignolo, 1969; Hacaen & Ajuriaguerra, 1964; Luria, 1966).
The proper meaning of a neuropsychological perspective should be clar-
ified. The rapid development of neuropsychological and neuroradiological
assessment devices makes it difficult to predict which test, group of tests,
battery, or type oftechnology might in the future provide the most appropriate
data upon which to base meaningful behavioral interventions (Horton &
Wedding, 1984). For example, in recent years, CT scanners have come into
widespread use and have significantly affected the demand for Halstead-Reitan
neuropsychological test batteries for diagnostic assessment. It would be rea-
sonable to expect that as technology continues to progress, many traditional
clinical neuropsychological assessment methods may be superseded by more
valid and reliable neurodiagnostic techniques. Thus, because ofthe probability
of significant technological change, it would appear unwise to identify be-
havioral neurpsychology within a single set of neuropsychological diagnostic
procedures. Rather, it would appear more prudent to identify major guidelines
or procedures based on the unique characteristic of the human brain and
interfaced with traditional, contemporary, and emerging behavior therapy
strategies. Chapter 2 will be devoted to a more thorough discussion of applied
behavior analysis.
INTRODUCTION 7
The neuropsychologist's major asset is the ability to measure neuropsy-
chological functioning in a precise, objective, and independently verifiable
fashion. Conversely, the limitation of neuropsychology is that it is not yet
able to make precise statements concerning day-to-day functioning from neu-
ropsychological test scores. On the other hand, the most salient advantage of
applied behavior analysis is that it provides explicit methods for intervention
as weH as demonstrated effectiveness in achieving behavior change in many
settings. The most glaring limitation ofbehavior analysis is that generalization
oflearning does not always occur; improvement may be situation specific. It
would seem that both neuropsychology and behavior analysis have unique
advantages and limitations. It would appear best to use their strengths in a
complementary manner, thus enabling some compensation for the specific
weaknesses inherent in each.
Such an amalgamation of conceptual models would perhaps produce
publicly verifiable assessments, dynamic understanding of brain injury and
its consequences, and effective therapeutic change which also would generalize
to new tasks, skiHs, and situations.
SUMMARY
Epidemiology
1. The NHIF estimates that over 1 million persons each year sustain
injuries in accidents severe enough to require hospitalization, and
of these, 30,000-50,000 persons have such serious intellectual or
behavioral dysfunction that they are unable to return to anormal
life.
2. The National Institute of Neurological and Communicative Disor-
ders and Stroke has estimated the annual cost of care for head-injured
patients in the United States at $3 billion (NINCDS, 1976).
3. Persons with brain injury caused by trauma usuaHy suffer multiple
problems that require the services of several different rehabilitation
disciplines, including medicine, speech therapy, neuropsychology,
physical therapy, occupational therapy, social work, and vocational
counseling.
4. The ultimate goal ofthe rehabilitation is to facilitate the process of
recovery of an individual toward the restoration of full physical,
social, and vocational capabilities.
The NYU Cognitive Retraining Model
5. The NYU model of intervention consists ofthe following five mod-
ules: (a) an orientation model dealing with attentional deficits, (b)
8
CHAPTER I
an eye-hand integration with finger dexterity hierarchy, (c) a
perceptual-cognitive integration constructional task hierarchy, (d)
a visual information processing task hierarchy, and (e) a verballogical
reasoning task hierarchy.
The Hawaii State Hospital Model
6. Neurotraining is defined as "the systematic application of psycho-
logical and neurological principles for the purposes of enabling in-
dividuals to overcome deficits that result from central nervous system
dysfunction. "
7. The key assumptions are the plasticity of function within the central
nervous system, and it is postulated that environmental stimulation
can facilitate learning.
8. Neurotraining assumes that the process oflearning is more important
than the specific content of any area.
9. Neurotraining is administered on a one-to-one basis, tailored to the
individual's needs, provided in step-by-step increments at regular
intervals with maximal stimulation, and aimed toward successful,
overlearned endeavors.
10. The areas of functional deficits are categorized as attention, cognition
(abstraction, feedback, organization, problem-solving, strategy, dis-
crimination, flexibility, inhibition-facilitation, memory), processing
or coordination (laterality, multimodal, perceptual-motor, sequenc-
ing, spatial-quantitative), and symbolic-language (afferent, efferent).
The Behavioral Neuropsychological Approach
11. Neuropsychology is defined as the study ofbrain-behavior relation-
ships. Behavioral neuropsychology may be defined as the application
of behavior therapy to problems of brain-injured individuals while
using neuropsychological assessment.
12. Intervening variables refer to theoretical creations whereas hypo-
thetical constructs are usually empirical or physical in function.
13. The neuropsychologist's major asset is the ability to measure neu-
ropsychological functioning in a precise, objective, and independently
verifiable fashion.
14. The limitation of neuropsychology is that it is not yet able to make
precise statements concerning day-to-day functioning from neuro-
psychological test scores.
INTRODUCTION 9
15. The most obvious advantage of applied behavior analysis is that it
provides explicit methods for intervention as weIl as demonstrating
effectiveness in achieving behavior change in many settings.
16. The most glaring limitation of the behavioral approach is that gen-
eralization of learning does not always occur; improvemeJ'+ may be
situation specific.
17. It is recommended that the strengths of applied behavior analysis
and neuropsychology be used in a complementary fashion.
2
Applied Behavior Analysis
In their book Applied Behavior Analysis, Cooper, Heron, and Heward (1987,
p. 14) define applied behavior analysis as "the science in which procedures
derived from the principles ofbehavior are systematically applied to improve
socially significant behavior to a meaningful degree and to demonstrate ex-
perimentally that the procedures employed were responsible for the improve-
ment in behavior." The key words here are science, socially signijicant be-
havior, and improvement. Thus, the focus of applied behavior analysis is the
improvement of socially significant behavior through scientific manipulation.
Behavior analysts use a simple paradigm, A-B-C. That is, each time a
behavior (B) occurs, a condition or antecedent (A) is present immediately
prior to that behavior, and there is a consequence (C) that follows the behavior.
It is through the analysis of this basic paradigm that the procedures used by
behavior therapists have emerged. Behavior analysis has been widely applied
in mental health, developmental disabilities, corrections, education, business,
and medicine. Only recently, however, has it been used in brain injury re-
habilitation. The purpose of this chapter is to suggest that rehabilitation
professionals can increase success in treating individuals with traumatic brain
injury (TBI) with proven applied behavior analysis strategies.
Applied behavior analysis is the treatment of choice for brain-injured
clients for four reasons:
1. The most common sequelae ofTBI include behavior disorders, mem-
ory loss, cognitive deficits, and increased inability to learn.
2. The TBI client must relearn almost all behavior to some extent. The
amount of behavior to be relearned is, of course, dependent on the
severity ofthe injury.
3. Applied behavior analysis is based on principles of learning.
4. Applied behavior analysis has been extremely successful when used
with clients.
11
12 CHAPTER 2
Applied behavior analysis can be implemented to affect two types of
behavior presented by clients:
I. Behavioral excesses: the irritating or obnoxious behavior that prevents
people from being welcome in most areas ofthe community or work-
place. Examples include physical and verbal aggression, alcohol and
drug abuse, impulsivity, and socially inappropriate behavior.
2. Behavioral deficits: those behaviors that occur at too low a frequency
or not at all. Examples include social skill deficits, memory loss, lack
of vocational skills, and communication deficits. These behavioral
deficits require learning new or alternative behavior.
To decrease behavioral excesses or increase behavioral deficits, behavior
analysis offers a process model that includes six steps. The steps in the
process are:
I. Identification of behavior to be studied or changed
2. Measurement of the current frequency of the identified behavior
3. A functional analysis of the behavior
4. An intervention plan
5. Programming generalization
6. Empirical evaluation
IDENTIFICATION AND MEASUREMENT
OF TARGET BEHAVIORS
Step 1 in the behavior analysis process is identifying the target behavior.
The rehabilitation professional must identify the behavior that needs to be
studied or changed. This identified behavior is called the "target behavior."
The inexperienced behavior therapist will usually target a problem behavior
and then develop or seek out procedures to reduce that behavior. This is
UI,:'lI'lUnate because behavior analysis is founded on learning theory, and the
basic premise is one of teaching new behavior. The experienced behavior
analyst is adept at identifying abilities on which to build new skills. For ex-
ample, a client may be disruptive in class-e.g., leaving without permission,
asking irrelevant or embarrassing questions, speaking out oftum, or making
jokes. These are obviously problem behaviors, and the novice behavior analyst
would try a punishment procedure to reduce their frequency. The more ex-
perienced behavior analyst, however, would recognize that reinforcing co-
operative and academic behavior and increasing it will eliminate disruptive
behavior. One cannot be both a good student and a class clown. The two
APPLIED BEHA VIOR ANALYSIS 13
behaviors are incompatible. Table 2.1 presents examples of behaviors that
are incompatible with aggressive behavior. Targeting the incompatible be-
havior will focus our intervention on reinforcing the appropriate behavior
versus punishing aggression.
Whatever behavior you identify as a target, the behavior must be precisely
or operationally defined. Hawkins and Dobes (1977) describe three charac-
teristics of a good definition. (1) The definition should be objective, referring
only to observable characteristics ofthe behavior (and environment, ifneeded)
or translating any inferential terms (such as "expressing hostile feelings," "in-
tended to help," or "showing interest in") into more objective ones. (2) The
definition should be clear yet should be reasonable and unambiguous so that
experienced observers could read it and readily paraphrase it accurately. (3)
The definition should be complete, delineating the boundaries of what is to
be included as an instance ofthe response and what is to be excluded, thereby
directing the observers in all situations that are likely to occur and leaving
little to their judgment.
Morris (1985, p. 169) suggests testing the definition of a target behavior
by asking: (1) Can you count the number of times that the behavior occurs
in, for example, a 15-minute period, a I-hour period, or 1 day? Or, can you
count the number of minutes that it takes for the client to perform the be-
havior? That is, can you tell someone that the behavior occurred "X" number
of times or "X" number of minutes today? (Your answer should be "yes.")
(2) Will astranger know exactly what to look for when you tell him or her
TABLE 2.1. Examples 0/ Behaviors That Are
Incompatible with Aggressive Behaviors
Aggressive behaviors
Hitting
Shoving
Kicking
Throwing objects
Pulling hair
Biting
Threatening facial expression
Swearing
Arguing
Criticizing
Threatening others
Shouting
Screaming
Incompatible social behaviors
Cooperating with others
Helping others
Participating witb agame
Smiling at others
Complimenting others
Engaging in noncontroversial talk
Offering to help others
Talking quietly
Whispering
14 CHAPTER 2
the target behavior you are planning to modify? That is, can you actually see
the child performing the behavior when it occurs? (Y our answer should be
"yes.") (3) Can you break down the target behavior into smaller behavioral
components, each of which is more specific and observable than the original
target behavior? (Y our answer should be "no.") Examples of precise behavioral
definitions are:
1. Teasing-provocative statements directed toward another person. In-
clude ridiculing, name-calling, taunting, picking on, and other nagging
or provoking verbal responses. Exclude friendly, playful teasing, and
other statements accompanied by smiles and laughter. 00 not include
threats to harm another person or another's property. Examples of
teasing include:
a. "Ha, ha, you got in trouble."
b. "Man, you're really a crybaby."
c. "You ugly S.O.B."
2. Arguing-a three-statement sequence ofnegative verbal provocation.
Include any verbal provocation that occurs in sequence such as teases,
ownership statements, refusals, denials, and other verbal responses
with negative affect and meaning. Exclude threats, playful arguing,
and true debates. Examples of arguing include:
a. "Get lost." "No, 1 won't." "Just leave me alone."
b. "You jerk." "Don't call me names." "I'11 do what 1 want."
c. "Give it back." "I1's mine, go lay off." "Y ou stole it out of my
room."
3. Threats-a verbal statement or physical gesture to hurt another person
or destroy something belonging to another. Verbal statements must
include a behavioral reference to aggressive responding, such as "I'm
gonna break off your arm." Gestures may include fist swinging, a
raised belt, stick, etc. Exclude playful, good-natured threats ("I'11 get
the boogeyman after you!") and threats that are unrealistic ("I'11 crush
your mother with my foot!"). Include any threat that the student may
be able to carry out. Examples of threats include:
a. 'Tm going to let the air out ofyour tires."
b. ''1'11 smack your face if you do that."
c. 'Tm gonna break every bone in your body."
d. 'Tm gonna kill you."
4. Hitting-aggressive behaviors toward another person that may pro-
duce pain or injury. Physical contact must be made by part of the
clien1's body or an object with which he has contact. Identify as hitting
only when you actually observe the aggressive act. Includes shoving,
APPLIED BEHA VIOR ANALYSIS 15
hitting, slapping, punching, kicking, pinching, throwing objects, etc.
Exdude playful or friendly contact perforrned in a positive context
(with smiles and laughter). Examples of hitting indude:
a. A swift kick in the butt
b. Several punches in the arm
c. A rapid succession of blows to the head with a fist or a two-by-
four
5. Fighting-Indicate fight only ifyou observe the dient engaged in an
exchange of physical and aggressive behaviors. This requires two or
more dients induding the target dient and at least a three-response
sequence ofbehaviors from the hit category. Exdude playful fighting
or wrestling that is done in a positive context or is accompanied by
smiles and laughter. Identify the behavior as fighting if one of the
dients involved in the exchange is only making weak attempts to fight
and is less aggressive. Examples of fighting indude:
a. Client A throws a pencil. Client B throws it back. Client A kicks
dient B.
b. Client A slaps dient B on the back. Client B turns and kicks dient
A. Client A punches dient B's face.
c. Client A hits dient B in the face. Client B punches dient A's head.
Client A kicks dient B powerfully in the groin.
6. Property damage-unauthorized destruction of personal or facility
property. Indudes breaking, ripping, tearing, cutting, shredding,
smashing, burning, shattering, etc. Exdude appropriate disposal of
items such as stomping of empty milk cartons and throwing it in the
trash. Indude marking or marring. Examples of property damage
indude:
a. Writing obscenities on the walls
b. Tearing someone's shirt
c. Smashing windows
d. Setting fires
7. Offers to share-A dient verbally or physically indicates that a peer
have, touch, take, manipulate, trade, or cooperatively use material
from the available free play activity or when a dient invites a peer to
join in a particular activity.
8. Productive activity-an activity that is perforrned in response to
something a teacher has requested or assigned. Examples are working
on a reading assignment, reading a library book, or listening to a tape-
recorded story. Answering a question should not be induded.
Although we have given several examples of definitions oftarget behav-
iors, one should not use standardized definitions. Target behaviors should be
16 CHAPTER 2
situation and complaint specific. The notion that a behavior analyst could
draw from a standardized list of target behaviors is antithetical to the concept
of individualized programming.
MEASUR/NG BEHA V/OR
After identifying and defining behavior, one must measure the current
frequency ofthe target behavior. By measuring the current level ofbehavior,
a baseline is established. A baseline is the extent to which the behavior is
occurring in the absence of the planned intervention. The most fundamental
method of measuring behavior is to count each instance ofthat behavior; this
is called a frequency count. A 24-hour frequency count is usually inconvenient
in applied settings; the therapist, therefore, selects portions of the day during
which the behavior is most likely to occur to record the frequency. There are
several things to consider when choosing frequency as a method of
measurement.
1. All observation times must be the same length.
2. The target behavior must be discrete; that is, it must have adefinite
beginning and end.
3. The target behavior should not occur at high rates.
4. The target behavior should not be in a dass of responses that can
occur for extended time periods.
Duration Recording
When a practitioner is concerned with how long a dient engages in high-
rate, extended, or continuous behaviors, duration recording should be used.
Duration measures can be collected using either of two procedures: total du-
ration or duration per occurrence. Total duration measures the total amount
of time an individual is engaged in a performance during aperiod of obser-
vation. In contrast, duration per occurrence reports the amount of time for
each instance of the behavior during the period of observation.
Analysts must be able to determine when frequency recording, total du-
ration, or duration per occurrence are appropriate for data coUection. For
instance, a teacher concerned about a student's out-of-seat behavior could
use frequency recording because out-of-seat behavior is discrete and would
not occur at such high rates as to make a taUy of occurrences difficult. The
teacher also could use total duration recording because one instance of out-
of-seat behavior has the potential to occur for an extended period of time.
APPLIED BEHA VIOR ANALYSIS 17
Total duration and frequency recording, however, measure entirely different
dimensions of behavior, and these differences provide the criterion for selec-
tion. Frequency recording establishes a numerical dimension ofthe behavior,
whereas duration recording provides the temporal dimension. With out-of-
seat behavior, frequency recording would tell how many times the student
left her seat. Total duration recording would indicate how long the student
was out of her seat during the observation period. Because of the relevance
ofthe temporal dimension, total duration recording would be a more appro-
priate measurement technique in this case. With frequency recording, the
teacher might report that the student was out of her seat only once in 30
minutes of observation. That one time, however, occupied 29 ofthe 30 min-
utes, and a different picture of the behavior is obtained. In this situation,
duration per occurrence would be an even better measurement technique
because it establishes both the numerical and temporal dimensions of the
behavior. By using duration per occurrence, the teacher would know the
number of times the student was out-of-seat and the duration of each occur-
rence. As a general rule, duration per occurrence is preferable to total duration
because it provides more information about the target behavior. Ifbehavioral
endurance is a major consideration, however, then total duration recording
may be sufficient (Tawney & Gast, 1984).
Latency Recording
Latency is the measurement oftime between a stimulus (e.g., instruction
or prompt) and the initiation of a behavior. Latency recording should be used
when the major concern is the length oftime between an opportunity to start
a behavior and the beginning performance of that behavior. For example, a
student may be slow in following teacher directions. The response latency
would be the length of time between the end of the teacher's direction and
the student's compliance. Concern can also focus on latencies that are too
short. For instance, a student may give incorrect answers because he or she
does not wait for the teacher to complete the question.
Interval and Momentary Time Sampling
Interval recording and momentary time sampling provide an estimate
ofthe number of occurrences and the duration ofbehaviors. With these data
collection systems, analysts record the number of timed intervals within an
observation session in which the target behavior has been identified as present
or absent. Interval recording and momentary time sampling are most useful
with continuous and high-rate behaviors.
18 CHAPTER 2
Interval recording is used to record the presence or absence of behavior
within specific time intervals. The total observation session is divided into
brief time intervals of equal size. For example, ifthe total observation session
is 10 minutes and the observer is using 10-second interval measurement, the
session would be divided into 60 equal 10-second recording units. The interval
size should provide the observer with sufficient time to observe and record
behavior reliably. Interval size usually ranges from 6 to 15 seconds, depending
on the behavior to be observed. To record the presence or absence ofbehavior,
the observer can draw aseries of ruled boxes on paper with each box repre-
senting one interval. The boxes can be positioned either vertically or hori-
zontally. The observer marks each time interval with a symbol that indicates
that the behavior occurred. Data collected via interval recording are reported
as a percentage of intervals in which the target behavior occurred.
Interval recording can be conducted in two ways. The first and most
common procedure is partial interval recording, which requires the observer
to record whether the behavior was present or absent at any time during the
interval. Partial-interval recording is not concerned with how many times the
behavior occurred during the interval or how long the behavior was present.
Whole-interval recording requires that the behavior be present throughout
the entire interval if it is to be considered an occurrence. For example, if
attending behaviors were recorded using whole-interval recording, a student
would need to attend during the full interval to have that interval scored as
an occurrence.
The procedure for momentary time sampling is similar to that for interval
recording but with a notable difference. Momentary time sampling is con-
cerned with recording the presence or absence of behaviors immediately fol-
lowing specified time intervals, unlike interval recording, which is concerned
with recording behaviors during specified time intervals. If an observer wishes
to record the occurrence or nonoccurrence of a behavior, the paper is ruIed
into squares that represent equal or variable intervals. Behavior is scored only
once per interval and is reported as a percentage of intervals scored.
Trials to Criterion
Trials to criterion is the number oftimes response opportunities are presented
before an individual achieves a preestablished level of accuracy or proficiency.
For example, the measurement could be reported as ten trials to achieve 100%
accuracy (percentage) or ten trials to achieve 60 words a minute (rate).
Measuring trials to criterion is appropriate in an evaluative comparison
of two or more kinds of materials or methods of intervention. For example,
a teacher might report the number of times a particular word was presented
APPLIED BEHA VIOR ANALYSIS 19
orally before a student read it independently and might compare that number
with the number of times the word was presented in written form before the
student read it independently. 1ftrials to criterion are tallied for several different
words taught to a student in different ways, the teacher can then compare
performance measures to determine whether the student mastered words better
with one method or another.
Number of Prompts
Frequently, especially when self-initiation is a problem, we might wish
to assess behavior in terms of the conditions under which it might be observed
to occur. In other words, we might want to know how many or what kind of
prompts cause a behavior to occur. You could count the number ofprompts
needed for a task to be completed, or you could score a prompt level shown
in Table 2.2.
GRAPHING DATA
After you have precisely defined the target behavior and started to measure
it, it is time to begin a graph of the behavior. Graphically displaying the mea-
surements of behavior allows one to form a picture of the behavior. It keeps
the practitioner dose to the data. Graphing baseline measurement and subse-
quent intervention measures allows one to visually identify trends in the data.
We often miss some of these subtle trends in our data when they are not
TALE 2.2. Levels 0/ Prompting
Test item
The test item was performed appropriately without further prompting or
guidance of any kind after a specific instruction was presented.
The test item was performed appropriately only after the instruction and a
specific verbal prompt were provided by the tester.
The test item was performed appropriately only after the instruction and a
modeling prompt were provided. Specific verbal information and a
modeling prompt are provided concurrently.
The test item was performed appropriately only when physical assistance
was provided.
The test item was not performed correctly or was not attempted.
Score
4
3
2
1
o
20
CHAPTER 2
graphed. In addition, graphing baseline data helps us to evaluate the success of
the intervention we will eventually implement to change the behavior.
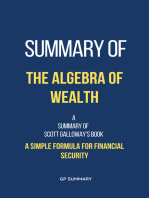
Figure 2.1 presents a sampie graph used to plot frequency. The number
of times the behavior was observed is plotted on the vertical axis; the horizontal
axis is the time frame of our observations.
Client:: ______ _ Behavior: ____________ _
Observer:.. _________ _
,0
29
28
27
26
2')
24
22
21
20
19
18
17
16
15
14
n
12
11
10
9
8
7
6
5
4
.,
2
1
0
1 2 3 4 5 6 7 8 9 10 12 14 16 1 20 22 24 26
Hours, Days, Weeks or Sessions
Target Behavior(s) and Definitions of Behavior(s): ________ _
Inwrvention: _____________________ ___
FlGURE 2.1. Frequency chart.
APPLIED BEHA VIOR ANALYSIS 21
If we had measured the frequency of inappropriate social comments in
each daily therapy session, the vertical axis would indicate the number of
inappropriate comments, and our time dimension (therapy sessions or days)
would be on the horizontal axis.
Ifwe were interested in the duration of a behavior, the vertical axis would
indicate the number of minutes or hours spent on an activity, and the hori-
zontal axis would indicate days, weeks, or sessions in which data were collected.
PERFORMING A FUNCTIONAL ANALYSIS
After you have identified and defined the behavior to be changed and
have empirical evidence ofits frequency, you can conduct a functional analysis
of the behavior. In other words, you use the A-B-C paradigm to carefully
identify the antecedents and consequences surrounding the target behavior.
This analysis allows one to understand the environmental influences that may
be causing or maintaining a particular behavior. Most of the research in be-
havior analysis has focused on how consequences affect behavior. The unique
problems of people with brain injury such as memory loss, impulsivity, and
disinhibition, however, necessitate greater analysis ofthe antecedent conditions
or what may have prompted the behavior to occur. In addition, rehabilitation
professionals, in consultation with a neuropsychologist, must determine what
impact the brain injury will have on the client's capacity to learn new behavior,
given memory loss and possible impaired ability to process visual, auditory,
or tactile information.
Although we have referred to conducting this functional analysis of be-
havior as step 3 in the behavior analysis process, in reality it is an analysis
that is used continually throughout the behavior analysis process. For example,
it would be difficult to identify and define a behavior without having some
idea of what is maintaining it. Perhaps, most of the information regarding
maintenance or nonexhibition of a behavior is provided by the results of an
intervention. Ifthe intervention is not successful, one must look at alternative
antecedents or consequences to influence that behavior. When programming
generalization, one must look at the antecedents and consequences main-
taining or preventing a behavior if transfer cannot be established.
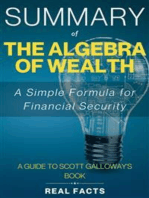
The form presented in Figure 2.2 is helpful when conducting the func-
tional analysis. Simply check the behavior of interest in the behavior col-
umn and make notes from your observations of anything that occurs im-
mediately prior to the behavior being exhibited and check the consequences
that followed the behavior. For example, assurne that you want to eliminate
verbal threats and replace them with more appropriate methods of dis-
22 CHAPTER 2
ABC CHECI:LIST
Describe anteeedent eonditions and then eirele applieable behavior(s)
and eonsequenees.
ANTECEDENTS BEHAVIOR(S) CONSEQUENCE(S)
What preeeded the behavior ?
Hurt seit Soeial disapproval
Hurtother Given warning
Property damage Item taken away
Sereaming Counseling
Xieking Redireeted
Biting Simple eorrection
Hitting Time out
Throwing Point loss
Date
stripping Ignored
Time Began
Toilet aeeident Followed program
Duration
Elopement Lost privilege
StaU
Stealing Sent to room
Verbal abuse Physieal restraint
Threatening
What preeeded the behavior ?
Hurt self
Soeial disapproval
Hurt other
Given warning
Property damage
Item taken away
SCreaming
counseling
Xieking
Redirected
Btting
Simple correetion
Hitting
Time out
Throwing
Point loss
Date
Stripping
Ignored
Time began
Toilet aeeident
Followed program
Duration
Elopement
Lost privilege
StaU
Stealing
Sentto room
Verbal abuse
Physical restraint
Threatening
FlGURE 2.2. A form for conducting a functional analysis.
agreeing or expressing dissatisfaction. First, we must identify the circum-
stances in the environment that may be maintaining verbal threats. After
you develop adefinition ofwhat constitutes a verbal threat and have mea-
sured the frequency of its occurrence, use the functional analysis form to
gather data for your analysis. 00 the threatening statements occur only
following requests or demands (antecedent conditions)? After making
APPLIED BEHA VIOR ANALYSIS 23
threats, are the demands reduced (consequences)? The information you
gather to conduct your functional analysis will prove critical in choosing
the most appropriate intervention. In the example above, the dient may
have learned that ifshe threatens the staffwith harm, the staffreduce their
demands. It also may be that her threatening statements follow requests
to attend therapy. The therapy sessions may weIl be providing direct evi-
dence to the dient of her limitations, and the threat is an expression of
frustration, anger, or denial. In either case, this functional analysis will
help you to better understand under what conditions the behavior may be
occurring, and it also provides us with an understanding of what we are
doing to maintain or reinforce the behavior.
EMPIRICAL EVALUATION
The final step in the behavioral process is the empirical evaluation. This
is extremely important as it provides the data necessary to determine whether,
in fact, the procedure had the desired effects on the target behavior. Evaluation
in brain injury rehabilitation has been sadly neglected. The complexity ofprob-
lems is the reason for the present state ofbrain injury rehabilitation evaluation.
It can be confidently asserted that brain-behavior relationships are incredibly
difficult to comprehend. The simple diagnosis of local brain injury involves a
variety of parameters induding, but not limited to, laterality, etiology, extent,
chronicity, age of the dient, and premorbid levels of functioning. When the
matrix of additional dimensions involved in treatment are added to these pa-
rameters, the mix of variables is difficult to describe, much less to untangle.
We shall present three common experimental designs used in behavior
analysis. Experimental designs are used to demonstrate the cause-effect re-
lationship between a particular behavior, sometimes referred to as adependent
variable, and a treatment program, sometimes referred to as the independent
variable. Although we are presenting three commonly used experimental de-
signs, it is important to remember Sidman's (1960) statement that "the fact
is that there are no rules of experimental design" (p. 214).
The Reversal (A-B-A-B) Design
The reversal design was once the most common experimental design
used in behavior analysis. We begin by taking a baseline ofthe target behavior
(A) and then implementing a treatment (B), reinstating the baseline by re-
moving the treatment (A), and finally, reinstating the treatment (B).
24 CHAPTER 2
A. A stable baseline is established.
B. The intervention is applied.
C. The intervention is removed and baseline conditions are reinstated.
D. The intervention is reinstated.
Control ofthe intervention is demonstrated ifthe target behavior changes
in the desired direction only when the intervention is in effect. When using
areversal design, several questions may arise. The first is: how long should
the baseline period last? Ideally, a baseline should continue until the pattern
of performance is stable or until it shows a trend in the direction opposite to
that predicted when the treatment is introduced. There are also ethical con-
siderations regarding the length of baseline. For example, if the behavior is
aggression or self-injury, then an extended baseline is ethically unacceptable.
It also may be unethical to reverse or reinstate baseline conditions after treat-
ment has been effective.
Multiple Baseline Designs
There are three kinds of multiple baseline designs:
1. Multiple baselines across behaviors
2. Multiple baselines across subjects
3. Multiple baselines across settings
In a multiple baselines across behaviors, baselines are simultaneously
taken across three or four behaviors. The treatment is then introduced on
one behavior but not the others. After demonstrating the effectiveness on the
first behavior, the treatment is introduced on the second behavior but not the
third. Finally, treatment is introduced on the third behavior (see Figure 2.3).
When using a multiple baselines across settings, simultaneous baselines
are taken in different situations but on the same behavior. Intervention is
employed sequentially across each setting (see Figure 2.4).
When using a multiple baselines across subjects, the treatment is imple-
mented sequentially on each subject until all subjects receive treatment (see
Figure 2.5).
Multiple Baselines across Behaviors
A. Baseline data are collected on a single subject for three or more be-
haviors.
B. After baseline reaches a stable rate, the intervention is introduced for
APPLIED BERA VIOR ANALYSIS
Behavior
1
Behavior
2
Behavior
3
A
Baseline
B
Intervention
Applied
Intervention
Applied
Time
FIGURE 2.3. Multiple baseline designs across behaviors.
25
Interventi on
Applied
only one behavior until the baseline conditions are continued for the
others.
C. The first target behavior should be affected while others remain at
stable levels.
D. When the rates are again stable for all behaviors, the intervention is
introduced for the second behavior.
E. This procedure is replicated until all behaviors receive the interven-
tion.
Control of the intervention is demonstrated when behavior change is
associated in each case with the introduction ofthe treatment or independent
variable.
Multiple Baselines across Subjects
A. This design follows the same procedures as the multiple base-
lines across behaviors except that the same behavior of three dif-
ferent individuals is used rather than several behaviors of one
individual.
B. Subjects must be exposed to the same environmental conditions to
rule out the possibility that something other than the intervention is
responsible for change.
26
SUbjeet
-.
A B
Baseline Intervention
Applied
Intervention
AppUeci
Time
FlGURE 2.4. Multiple baseline designs across subjects.
CHAPTER 2
Interventl OD
Appliecl
Experimental control is demonstrated when the target behavior changes
for each subject.
Multiple Baselines across Settings
A. With this design, the treatment is applied to the target behavior first
in one situation, then in the other, in a manner similar to applying
intervention to three different behaviors or three different subjects.
B. Control of the intervention is demonstrated if the behavior changes
in a particular situation only when the intervention is introduced.
The obvious advantage ofthese multiple baseline designs over areversal
design is that they eliminate the need for returning to a baseline condition.
On the other hand, it is not always possible to find two or more behaviors,
two or more settings, or two or more people who can be baselined simulta-
neously such that there is complete independence among multiple measures.
Moreover, it often takes additional time and observers to gather the necessary
data for multiple baselines.
Alternating Treatments Design
The alternating treatment or multielement design is used to compare the
effects of different treatments within an individual. Two or more treatment
APPLIED BEHA VIOR ANALYSIS
Situation
"'1
Situation
"'2
Situation
"'3
A
Baseline
B
Intervention
Applied
Intervention
Applied
Time
FIGURE 2.5. Multiple baseline designs across settings.
27
Interventi on
App1ied
conditions are programmed in randomly alternating sessions with the same
individual (see Figure 2.6).
One problem associated with alternating treatment designs is that the
treatment conditions may interact; that is, one ofthe treatments may produce
an effect either because of the contrast to the other treatment in alternating
Treatment "A" and "B"
12
Treatment A
10
8
6
4
o 10
Days
20
FIGURE 2.6. Alternating treatment designs.
28 CHAPTER 2
sessions or because of generalization across conditions. In other words, if just
one treatment had been applied, the effects gained may not have been much
greater.
A. The design is useful when you want to compare the relative effec-
tiveness of two or more treatments.
B. The design involves the alternation oftreatment within a single sub-
ject.
C. No specific time duration between alternation of the treatments is
required.
D. The effects of both treatments on the target behavior are plotted on
a graph.
E. If the two treatments separate over time, you can say with some
certainty that one treatment is superior to the other.
SUMMARY
Applied Behavior Analysis
1. Applied behavior analysis has been defined as the science in which
procedures derived from the principles ofbehavior are systematically
applied to improve socially significant behavior to a meaningful de-
gree. It must demonstrate experimentally that the procedures em-
ployed were responsible for the improvement in behavior.
2. Behavior analysis procedures have been widely applied to other pop-
ulations including mental health, mental retardation, education,
business, and medicine.
Identification and Measurement ojTarget Behaviors
3. Step 1 in the behavior analysis process is identifying the target be-
haviors. The rehabilitation professional must precisely pinpoint the
behavior and then develop procedures to increase or reduce the be-
havior.
4. The novice behavior therapist will usually target an inappropriate
behavior and then develop procedures to reduce the behavior, while
the experienced behavior analyst will target an adaptive behavior
and develop a plan to increase it.
5. Three characteristics of a good definition include: (a) the definition
should be objective, referring only to observable characteristics of
the behavior, (b) the definition should be clear, and (c) the definition
APPLIED BEHA VIOR ANALYSIS 29
should be complete, outlining what is an occurrence and what is
not.
6. One should not use standardized definitions of target behaviors;
rather, they should be individualized to each dient.
Measuring Behavior
7. Baseline refers to the extent to which a behavior is occurring in the
absence of the planned intervention.
8. Frequency simply refers to counting each occurrence of a behavior.
Frequency provides the number oftimes a behavior occurs in a spec-
ified time period.
9. Duration recording is used to measure how long a behavior occurs.
Duration recording should be used for high-rate, extended, or con-
tinuous behaviors.
10. Latency recording is the measurement oftime between the onset of
a stimulus (e.g., instruction prompt) and the initiation ofa behavior.
Latency recording is recommended when the major concern is the
length of time between an opportunity to emit a behavior and the
beginning of that behavior.
11. Interval recording is used to record the presence or absence of be-
havior within a specific time interval. Partial-interval recording re-
quires the observer to record simply whether the behavior was present
during the interval. With whole-interval recording the behavior must
occur throughout the entire interval in order to be scored an occur-
rence of behavior.
12. Trials to criterion refers to the number of times response opportu-
nities are presented before an individual achieves a preestablished
level of accuracy or proficiency.
13. Number of prompts refers to the number of prompts that were re-
quired to facilitate the occurrence of a behavior.
Graphing Data
14. Graphically displaying the measurements ofbehavior allows one to
form a picture of the behavior. It keeps the practitioner dose to the
data.
15. Graphing baseline measurement and subsequent intervention mea-
sures allows one to visually identify trends in the data. We often
miss some subtle trends in our data if they are not graphed.
30 CHAPTER 2
16. Graphing baseline data helps us to evaluate the success or lack of
success of the intervention.
Performing a Functional Analysis
17. In performing a functional analysis, we determine the functional
relationships causing and maintaining the target behavior. The func-
tional analysis entails studying relationships between the target be-
havior and its antecedents and consequences.
Empirical Evaluation
18. Experimental evaluation is extremely important as it provides the
data necessary to determine whether the procedure had the desired
effects on the target behavior.
19. Components of an (A-B-A-B) reversal design include: (a) a stable
baseline is established, (b) the intervention is appIied, (c) the inter-
vention is removed and baseline conditions are reinstated, and (d)
the intervention is reinstated.
20. There are three types ofmultiple baseline designs: (a) multiple base-
Iines across behaviors, (b) multiple baselines across subjects, and (c)
multiple baselines across settings.
21. An alternating treatments design consists of comparing two or more
treatments within an individual. Treatments are randomly presented
to the individual rapidly and repeatedly.
Developing the
Rehabilitation Plan
3
Rehabilitation planning for individuals following a traumatic brain injury is
a goal-oriented, dient-centered process with its foundations in functional,
integrated, and comprehensive assessment (Guare, Samson, Guth, Warren,
& Burke, 1988). The emphasis on dient-centered assessment relates to the
extreme variation in skill performance even among individuals with similar
brain injuries. In more specific terms, rehabilitation planning following brain
injury is defined as a process of identifying a desired outcome; specifying
current performance abilities and inabilities (those skills needed to function
in the desired community, educational, and vocational domains); and defining
the necessary interventions, services, and environments that will assist an
individual in achieving the desired objectives.
To accomplish this, comprehensive evaluation is a critical first step. The
evaluation must be carried out by a dinical team that is capable of operating
in an inter- or transdisciplinary fashion.
There are two primary reasons for this. First, the thoughts, emotions,
and physical and social behavior ofhead-injured persons derive from a single
source and are interrelated. To conduct separate and independent evaluations
that separate what are, in fact, integrated functions will lead to fragmented
treatment planning and intervention. Second, the objectives ofthe dient and
family must have a priority in the evaluation and rehabilitation planning
process. When separate, independent evaluations from various rehabilitation
specialists in each discipline occur, they typically make their own discipline-
specific recommendations. These recommendations may or may not be ger-
mane to the stated objectives of the dient and family and may or may not
be consistent with the objectives of other dinicians. Rather than yielding this
multiplicity of possible unrelated objectives, a team evaluation facilitates in-
31
32 CHAPTER 3
tegration of data, and those data are designed to address the achievability of
dient and family objectives. Thus, we propose that, whenever possible, re-
habilitation planning for the head-injured dient begin with a team that indudes
as many relevant rehabilitation disciplines as can be brought together along
with the family, the dient, and the referring agency. This chapter contains a
detailed description of the evaluation and treatment process, which constitutes
the heart of the rehabilitation plan.
EVALUATION IN THE NATURAL ENVIRONMENT
Rehabilitation planning begins with the evaluation ofthe dient. We see
this evaluation as consisting ofthree major components. The first component
is the observation ofthe dient in his or her horne and community and school
or job setting ifthat is where he or she is expected to return. This component
indudes interviews with the dient, the family, and the referring or current
treatment personnel. The purpose of these interviews is to evoke specific ob-
jectives that those individuals hope to accomplish as a result ofthe evaluation
and treatment process. This component is critical to the success or failure of
the rehabilitation process.
The second component of the evaluation is the formal, discipline-by-
discipline evaluation, which yields data about the dient's cognitive, emotional,
physical, behavioral, and social status. This component is the aspect with
wh ich most rehabilitation personnel are familiar, and it is frequently this
information that is seen as the key in rehabilitation planning. While the in-
formation gathered through these evaluations is important, it should not be
the only or even the primary element in rehabilitation planning. Rather, this
formal evaluation must be viewed in the context of the dient's history and
current objectives, along with the critical situation al assessments.
The third major component of the evaluation is the situational assess-
ment. For this component, each dinician determines aseries of situations
that are related to the projected environment in which the dient will ultimately
live. The dient then performs the activities and responds to the demands of
those situations, and his or her responses are evaluated by the dinician. Once
these evaluation components have been completed, the information is syn-
thesized by the team, which indudes the dient, family, and referring source.
Through this process, treatment outcome objectives are decided on by the
team and treatment probes, i.e., tentative treatment techniques, are decided
on along with who will be responsible for implementation.
THE CLIENT IN THE NATURAL ENVIRONMENT
Ifthere is an expectation that the dient will ultimately return to the same
community or situation from which he or she is being referred for treatment,
DEVELOPING THE REHABILITATION PLAN 33
then the evaluation should begin in that situation. The variables in the job,
school, community, and family of the client are likely to be different from
those in the treatment or rehabilitation setting. The way in which the client
experiences and is experienced within his or her "natural" environment is
unique and contains both positive and negative influences. Family members,
co-workers, and neighbors in vocational and recreational situations represent
elements that are specific to each client and cannot be easily duplicated in
the rehabilitation setting. We know that head-injured clients cannot easily
generalize their learning from one situation to another. While it may not be
possible to conduct their treatment in the natural environment, it is critical
to know what the demands of this environment are so that they can be ap-
proximated and addressed in the treatment setting. Otherwise, generalization
from the treatment setting is unlikely to take place.
Clients are typically referred because of an inability to effectively respond
to the demands of their environment. The cultural, community, and peer
group expectations to wh ich the client is subject may be different from those
of the rehabilitation setting or personnel. In residential rehabilitation pro-
grams, even different geographie origins may make so me of the client's be-
haviors unfamiliar. Certainly in the case of adolescents, wh at is viewed as
acting-out behavior and credited to the head injury may instead be normal
ifviewed in the context ofthe person's peer group. We must remain aware
of the context of the person's life to ensure that their treatment will help
them co pe with the demands of their environment and not just the envi-
ronment in which they are currently being treated. Knowing what these
demands are and what, if any, response the client makes to them is the first
step in determining barriers to successful community living. This phase of
evaluation begins with an information-gathering process and interviews with
the client, family, and past or current personnel involved in treatment and
rehabilitation.
A detailed premorbid history (i.e., prior to injury) is the first information
to be gathered. This history gives us our first sense of who the client iso By
examining the developmental and educational history, medical history, vo-
cational training and experience, and recreationalfleisure preferences, we can
begin to understand the skills, deficits, and personality of the client. Depending
on the severity ofinjury, the similarity between pre- and postinjury behavior
can range from nonexistent to barely distinguishable differences. Regardless
ofthis, however, past experience will be the best place to begin rehabilitation
planning because, even in the case of severe injuries, the information and
behaviors that are best retained are those that have been experienced repeat-
edly. It is, therefore, this information and behavior that will be easiest to
build on.
34 CHAPTER 3
Specific preinjury history information needed indudes the following:
1. Medical history. This should indude data concerning developmental
history, illnesses, major accidents, physical limitations, and general health.
Specifically, it is important to know if there were any premorbid neurologie
or psychologie problems. Patterns of drug and alcohol use should be
questioned.
2. Educational history. The number of years of education completed
and the level of performance should be determined. It is important to know
ifthere are any learning or behavior problems and what the person's attitude
was toward schoo!. There is evidence in the head injury literature indicating
that a significant number ofhead-injured persons had learning problems prior
to their injury. Since the problems encountered in learning disabilities are
similar to those encountered in head injury-e.g., attention, memory, plan-
ning, and organization-this information will impact in rehabilitation
planning.
3. Vocational history. Return to work is a major priority in rehabilitation.
Knowledge about the dient's preinjury vocational training, work experience,
job preferences, and performance evaluations will be the first step in vocational
planning. As noted above, it would be easiest to build on those skills that the
individual developed prior to injury, and hence, this information would be
the starting point for job training.
4. Psychosocial history. This should indude information about family
background and family relationships, the dient's personality and style ofbe-
havior, peer and community interactions, availability ofsupport systems, and
leisure preferences.
While some ofthis information may be available in written form (e.g.,
school transcripts, medical history) or from family members, whenever pos-
sible brief interviews with individuals such as job supervisors and teachers
can be invaluable.
After this information has been gathered, a detailed postinjury history is
important. This history begins with the occurrence of the injury itself and
medical treatment in the acute care hospital, followed by the results of any
rehabilitation and the person's course of recovery. By gathering some of the
same information as in the preinjury history and knowing the degree of medical
recovery, it is possible to get a sense ofthe change in life-style and the impact
the injury has had. If the dient has contact with some of the same people
both pre- and postinjury, then interviewing these people can provide a dear
sense of changes or deficits that have resulted.
After reviewing this information, the next step in the process is inter-
viewing the dient, family, and referral source when appropriate. The purpose
of the interviews is to create specific objectives for the referral source which
indude behaviors that are operationally definable. It is these objectives that
DEVELOPING THE REHABILITATION PLAN 35
the dient, family, and referral source see as critical in defining whether treat-
ment has succeeded or failed. To gather data effectively, at least two elements
are necessary. First, at the time ofthe interview, as much background infor-
mation as possible must have been collected and reviewed. Second, the in-
terviewer must be able to get from the family, dient, and referral source those
specific behavioral examples and specific situations that demonstrate the crit-
ical behaviors that need to be taught or diminished to enhance independent
functioning.
Ifthe defined objectives cannot be addressed after this initial intake eval-
uation procedure, the remainder ofthe evaluation will flounder. At the onset
ofthis process, it should be explained to the family, dient, and referral source
that the initial step in this process is to obtain objectives from them. They
may feel that they lack the expertise to formulate such objectives and that
this is the purpose of the team's evaluation process. The interviewer should
demonstrate, however, by the information that the dient and family provide
that they are, in fact, aware ofwhat is needed and desired. Once these objectives
have been stated, it is the job of the evaluation team to assess the achievability
ofthe objectives, the types ofskills that will be needed to achieve the objectives,
and the time and resources necessary to complete the job. In other words, it
is the responsibility ofthe evaluation team to flush out, fine-tune, and evaluate
the objectives that are provided by the dient, family, and referral source.
While some help from the interviewer or the team to define the objectives
may be necessary, it seems likely that each dient's wishes to leam certain
skills or eliminate certain behaviors should be considered.
Once the specific objectives have been ascertained, they should be pre-
sented to the entire evaluation team for discussion. This presentation is critical
because the objectives form the background against which the next phase of
the evaluation is to be conducted.
FORMAL CLINICAL ASSESSMENTS
The second major element in the evaluation process is the assessment
ofthe dient by various dinical disciplines using the instruments and techniques
unique to each. Clinical members of the team will typically indude the oc-
cupational therapist, physical therapist, social worker, speech/language pa-
thologist, vocational specialist, behavioral psychologist, nurse, neuropsy-
chologist, and neurologist. Depending on the age, problems, and goals of the
dient, an educator and a psychiatrist may become part of the dinical eval-
uation. The necessity for evaluation by each of these disciplines will be de-
termined by the presenting problems and objectives ofthe dient. Each dinician
will minimally review the available data relevant to his or her specialty and
36 CHAPTER 3
make a determination on the need for more in-depth evaluation. Although
background information may not indicate problems in a particular dinical
area unless arecent evaluation has been conducted, each dinician should at
least conduct a screening evaluation to ensure that nothing of significance
has been overlooked. For the disciplines in which it is determined that eval-
uations are necessary, these evaluations will consist of tests unique to each
discipline that yield information and the detailed data that constitute a mi-
croscopic view ofthe dient's current physical, cognitive, and social functioning.
The following are examples of areas within each dinical discipline that would
be evaluated.
The sodal worker initiates the evaluation process by compiling a detailed
psychosocial history. This is done separately with the dient and family where
possible to highlight discrepancies in perceptions. The evaluation indudes
family history, values, and dynamics along with the support systems that
surround the family. The purpose is to locate the dient and the family within
a context and to understand and use that context in the rehabilitation process.
Knowledge of the family-dient context is important because it is areturn to
that context for which the dient must be prepared. Members of the rehabil-
itation team, working day after day in their own treatment context (e.g., hos-
pital, residential center), may begin to use their own context as the frame of
reference for judging dient behavior. Viewing the dient in this context can
lead to the development of objectives that may be more relevant to the needs
ofthe rehabilitation team or the facility than to those ofthe dient or family.
Hence, we must always remind ourselves ofthe client's situation and evaluate
behavior in the context of that situation. Finally, in evaluating the dient's
context, the social worker can begin the identification of resources (e.g., church
groups and community agencies) and support systems that will be mobilized
to receive the dient as part ofthe discharge planning process.
The focus ofthe occupational therapist's evaluation is the assessment of
skills that underlie and make up the simple and complex activities of daily
living. This assessment is concerned with visual spatial and visual motor func-
tions, upper extremity functioning, and manual dexterity and sensory motor
integration. In addition, as part of the level of performance evaluation, the
therapist will look at money and time management, orientation, and the
client's knowledge about the everyday environment to determine the likelihood
of success for functioning in that environment.
The physical therapist is responsible for evaluation ofthe dient's physical
status as it relates to the ability to move and carry out activities. To accomplish
this, the physical therapist completes an evaluation of the following skills:
mobility, gross motor coordination, strength and endurance, range of motion,
motor planning, tone, sensation, posture, balance, and equilibrium.
DEVELOPING THE REHABILITATION PLAN 37
The speechjlanguage pathologist is charged with evaluating the oral motor
and communication skills of the individual. The former includes following
the motor functions required to produce sounds. Communicative ability is
evaluated across four broad categories: phonology (speech sounds), semantics
(the meaning of words), syntax (the structure of language), and pragmatics
(the uses of communication). The speech/language pathologist looks at both
receptive and expressive capacities in these areas and how they are integrated
to make up auditory comprehension, reading comprehension, verbal expres-
sion, written expression, and social communication.
The formal evaluation by the vocational specialist examines the interests,
aptitudes, and attitudes ofthe individual as they relate to the world ofwork.
Information regarding the interests and expectations ofthe client is particularly
critical since many individuals will have had a preinjury work history that
substantially impacts on their ideas about return to work. Depending on the
nature and range of the deficits, the vocational evaluation may be combined
with or incorporate one or more of the other clinical specialties that impact
on job performance. For example, ifprior to injury the individual was involved
in a manufacturingjob that required visual discrimination or complete upper
extremity functions, and these skills are impaired, then vocational and oc-
cupational therapists will need to conduct a joint assessment.
The neuropsychologist carries out a comprehensive assessment of the
cognitive and emotional status of the client. Tbis includes the evaluation of
reasoning skills, memory, attention, language, visual spatial and constructional
skills, information processing and response speed, auditory perception, tactile
perception, academic achievement where appropriate, and a personality as-
sessment. Through tbis examination, the neuropsychologist is able to evaluate
level of performance of the individual in comparison with other people of
that age. More important, the neuropsychologist is able to examine the process
by which the individual acquires and retains information and approaches and
solves problem tasks.
The nurse, through a review of current medical information and physical
evaluation of the patient, assesses general health status, problems, and med-
ication regimens that have been prescribed for health maintenance. The nurse
also assesses the individual's knowledge ofhis or her condition, general health
care practices, and specific routines that are necessary for medical mainte-
nance. If arecent neurological evaluation has not been conducted, then the
neurologist will conduct a full neurological evaluation including any diagnostic
tests that are needed. The purpose of the evaluation is to ensure that there
are no medical contraindications to participation in rehabilitation and to
assist in rehabilitation through active medical management (e.g., medication
changes).
38 CHAPTER 3
Additional team members might include a teacher, depending on the
age and projected needs of the client, and a psychiatrist, depending on the
presence of mood or thought disorders. As noted above, this phase of the
evaluation process involves formal, systematic assessment using test instru-
ments developed for each clinical specialty. Data obtained from these eval-
uations in highly structured settings are likely to be atypical of the client's
day-to-day situational demands. On the face of it, such data may also be of
unknown or seemingly questionable relevance to the client's presenting prob-
lems. When combined with other major evaluation elements, however, in-
formation obtained in these situations can be critical in planning the reha-
bilitation process, the objective of which is the acquisition and retention of
new information and behavior. Without knowing the status of the skills as-
sessed by the various clinical disciplines, the rehabilitation process can become
an exercise in trial-and-error treatment, a waste ofvaluable time for both the
client and clinician. For example, to employ verbal instruction strategies with
a person who has receptive language or auditory processing problems may
result in failure to leani. Such deficits can be missed in situational observation
because the individual with such a deficit may fail to respond in a situational
observation, but the failure may be credited to lack of motivation, poor teach-
ing, or a host of other variables that are,in fact, not the source ofthe problem.
By assessing discrete and specific functions, the formal, discipline-specific
evaluations provide information about strong and weak skill areas and the
learning styles and modalities that are most likely to lead to successful infor-
mation processing.
In addition to this information on specific skill areas in styles and mo-
dalities of learning, informal evaluations by each clinician should provide
information in two other areas. The first is to comment on the implications
ofthe information obtained in each clinical area as they relate to the objectives
initially stated by the client, family, and referring agency. For example, if one
ofthe objectives ofthe client is to return to college to complete a degree, and
it is determined in the formal evaluation that severe auditory and visual mem-
ory deficits are present, then the hypothesized impact of those findings for
the achievement of the objective should be stated in the clinician's report.
Second, each clinician should state additional findings of the evaluation that
he or she feels are critical to the independent functioning and quality of life
for the dient, although not covered in the initial client and family objectives.
This statement of additional findings should not be confused with a lengthy
list of objectives that are often found at the end of clinical reports. These
objectives often are written in response to below-average findings in specific
skill areas in each evaluation (e.g., the individual scored well below average
on the block design; therefore, visual-motor training is needed). Too often,
DEVELOPING THE REHABILITATION PLAN 39
such lists are offered without much thought to the relevance for the dient's
or family's objectives or for their impact on meaningfulliving.
SITUATIONAL EVALUATION
While the formal evaluations can provide detailed and valuable infor-
mation about the dient's status, they are not sufficient for rehabilitation plan-
ning. In fact, the structure, cuing, and nurturing provided by dinicians as
they carry out formal evaluations may compensate for and to some extent
mask the very deficits that are most often seen in head-injured individuals.
Most notably, the so-called executive functions-which involve planning and
organization, sustained attention, impulse control, and initiation-tend to be
less evident in structured, one-to-one situations where there is a reduction in
extraneous stimuli. Thus, the information gained during formal evaluations
must be considered in the context of previous behavior, behavioral reports,
observations of the dient, and the evaluation which is conducted by various
dinical disciplines in day-to-day situations. In these more unstructured sit-
uations, the problems and coping skills of the dients as they occur naturally
will be seen. This will allow dinicians to combine their formal data with
naturalistic observations and thus bring validity to the evaluation process.
There is no fixed number ofsituations, nor is the content ofthe situations
determined prior to knowing the dient. Rather, the types of situations in
wh ich the dient is evaluated will depend on his or her entry-Ievel behaviors
and the objectives that constitute the reason for the referral. Each dinical
discipline will determine what situations or settings are most appropriate to
observe the particular behaviors of concern and what situations will best ad-
dress questions relating to the objectives stated by the dient and the family.
For ex am pie, if a dient has been living at horne or in an institution where
daily needs have been attended to by other persons, the goal is for the dient
to live in an unsupervised or minimally supervised apartrr.ent or horne, then
an assessment of daily living skills must occur in that type of environment.
Thus, the occupational therapist will conduct evaluations of self-care, cooking,
laundry skills, and so on to determine the level of functioning of the dient
for those skills and environments. lethe objective were different, for example,
adesire to decrease social isolation, then other types of situations would need
to be evaluated. For example, the speech pathologist might observe the dient
initiating conversations with peers. In this case, the speech pathologist may
observe and evaluate such skills as eye contact, gestural reactions to the listener,
ability to keep in mind what the speaker is saying, and ability for planning
what to say.
40 CHAPTER 3
Regardless of where they occur, these situational evaluations must be
carried out in a systematic and planned way. The purpose is not to overwhelm
the client or cause problems in the community settings. For treatment pur-
poses, however, it is critical to know how the client will be able to function
in a range of common domestic, community, vocational/educational, and
recreational situations that he or she might ultimately desire. Only by con-
ducting observational evaluations in "in vivo" situations can hypotheses be
generated about what may benefit some of the problem behaviors or how the
skill deficits manifest themselves. Given the nature of the head in jury, it is
possible to make general statements about the problems the individuals will
face in some daily living and vocational situations. For example, attending,
planning, organizing, and remembering can be anticipated as problems given
the "typical" head injury. When one looks, however, at a variety ofindividuals
postinjury, it is evident that each tolerates one situation or another differently.
The same general skill deficit (e.g., attending or memory) may or may not
cause problems in one individual or another depending on other variables
(e.g., motivation, amount ofstimulation, sensitivity to social skills). Moreover,
the behaviors manifested when the individual is under stress, that is, where
he or she is unsure of ability to perform, are idiosyncratic. The response may
vary from withdrawal to aggression depending on the person's history in re-
sponse to frustration and stress. Thus, while the skill deficit may be known
in general, the interaction between the individual and the situation and re-
sulting behavior is not.
Just as skill deficits will be played out differently in different situations,
the range of coping responses that the individual has can also be expected to
vary from situation to situation. It is critical for the clinician to observe and
understand these coping strategies; if they are adaptive, they will form the
basis of treatment in a particular situation. W orking with strategies that cap-
italize on existing behavioral and leaming patterns is far easier than trying to
introduce new and unfamiliar strategies. Putting this observational information
in the context of the client's premorbid life can help the team to understand
the behavior and to devise strategies for intervention that "fit" the individual.
Often overlooked in observing the client's leaming and behavior is con-
sideration of the individual's own knowledge about the ways that he or she
leams best. Some individuals are able to respond directly to the question,
"What would help you to learn in this situation?" This question is often
overlooked in the evaluation process. In doing so, the clinician misses an
opportunity not only to gain intervention information, but also to enhance
the individual's sense of participation and control in the rehabilitation planning
process. Some individuals may have only a vague awareness ofwhat methods
or information could be helpful to them. They do show, however, a preference
when asked to select among a number of different instructional techniques.
DEVELOPING THE REHABILITATION PLAN
41
Even in the absence of awareness about specific methods or content, individ-
uals may prefer one option over another. In part, this has to do with learning
style, but in addition, it involves self-concept, past experience, and perhaps,
most important, a sense of choice and control over one's life. While it may
seem evident to ask or inquire about the dient's knowledge ofhim- or herself
or to present the person with alternative approaches to problem-solving from
which they might choose, rehabilitation recommendations and plans are often
written without this information. Trying to get a sense from the dient ofhow
he or she might best be taught and thus giving hirn or her some choice about
methods and strategies can certainly speed up the search for productive meth-
ods and also ensure dient participation and cooperation during the rehabil-
itation process.
As noted above, the types of situations to be used for evaluation will vary
somewhat from client to client depending on stated objectives along with
information gathered during the formal evaluation. Figures 3.1, 3.2, and 3.3
present structured observation formats that might be used for the assessment
of a client in the areas of cooking, laundry, and shopping.
Each clinician may have specific situations that he or she needs to observe.
For some situations, however, multiple skills (money management, language,
mobility) are needed. Hence, clinicians may work together and observe be-
haviors specific to their discipline in the same situation.
Regardless of the particular situation, there are three levels of observation
that potentially could be used. At the first level, the clinician(s) observes the
individual in the situation from a distance and provide no assistance or cuing
as the individual moves through the task sequence. If the individual is un-
successful, then the situation is presented a second time with the clinician
providing cues at what appear to be crucial times in the first evaluation. If
the individual remains unsuccessful, then systematic and intensive cuing or
environmental modification is provided at whatever level is necessary for the
individual to successfully complete the task. Since a task analysis of the sit-
uation will have been carried out prior to its use, the type, number, and timing
of assistive cues or prompts can be reported for each step of the task. When
possible, videotaping can be valuable and can eliminate the need for obser-
vations by multiple team staff.
Ouring phase 2, and particularly phase 3 of the evaluation process, two
objectives are accomplished. The first is the delineation of the individual's
behavior and levels of performance including skills and deficits. The second
is the beginning of hypothesis generation about effective treatment strategies
based on treatment probes that have been tried by the clinicians in the course
of their evaluations and observations up to this point. Questions such as
"What type and intensity of cue is needed to keep the individual on task?,"
"Is performance more consistent with tight structure?," or "Is there a response
42 CHAPTER 3
Client's Name: Date:
-------------------------- ----------------
Observer's Name:
------------------------------------
Pass Fall Comments
Located food for meal:
Located utensils, cookware
formeal:
Located utensils in
appropriate/safe manner:
Turned appropriate
stove knob on:
Set knob for appropriate
temperature:
Used pot holders:
Wiped up spills:
Followed steps of recipe:
Transports hot items safely:
Adjusted cooking heat
asneeded:
Food adequately cooked for
safety purposes (e.g. pork):
Handled food & cookware
in sanitary manner:
Other:
Poor Fair Good
General Assessment:
Awareness of Safety Factors:
Judgment:
Attention Span:
Frustration Tolerance:
Other Comments:
FIGURE 3.1. Structured observation format for cooking.
DEVELOPING THE REHABILITATION PLAN 43
Client's Name: Date:
--------------------
Observer's Name:
---------------------------------------------------
Pass Fall Comments
1. Ga thered solled clothes
and linens:
2. Put soiled clothes & linens into
Jaundry bag/basket:
3. Calculated amount & type of change
needed to wash & dry:
4. Sorted clothes according to color
and/or material type:
5. Put different categories of clothes
in separate mlichines:
6. Set washing machine for
BEJ'ropriate cycle:
7. Put appropriate amount of
detergent in machine:
8. Put correct amount of change
inmachine:
9. Started the machine:
10. Monitored washing
machines:
11. Removed clothes from machine at
the end of the cyde:
12. Pu t clothes in dryer:
13. Put correct amount of
change in dryer:
14. Started the dryer:
15. Monitored the dryer:
16. Removed dry dothes from
the dryer:
17. Restarted dryet (i!
needed) (Return to step 15)
18. Folded clothes following step 16
and/or 17:
19. Folded clothes into laundry
bag or basket:
20. Back in the room. student sorted
the clothes into separate groups:
underwear, shirts, pants/shorts,
linens:
21. Put folded clothes away
properly:
FlGURE 3.2. Structured observation format for laundry.
44 CHAPTER 3
Objective: When left at a parking lot in a shopping plaza, the
client will buy a predetermined item(s) at a drug store and will
return to the vehicle.
Client's Name: ..________ Date: ________ _
ObseITersName: ________________ __
Pass Fall Comments
Brought identification:
Brought money:
Dressed appropriately for
the weather:
Dress won't produce adverse
public reaction:
Arrived at designated place:
Crossed parking lot safely w / 0
causing dangerous situations:
Found itern(s) in store:
Purchased designated
itern(s) only:
Received correet amount
of change:
Returned to vehicle at
designated time:
FIGURE 3.3. Struetured observation format for shopping.
to presumed social reinforcement and encouragement?" will help guide de-
cisions about treatment probes that will be implemented in the next phase of
the evaluation process.
FINAL OUTCOME
At the completion of all evaluations, the c1inicians on the team meet to
compare and review the evaluation data. At this meeting, the team leader
first restates the referral objectives given by the c1ient, family, and referral
agency. This is followed by a time-limited presentation by each c1inician re-
viewing the formal and observational data and commenting on the achiev-
DEVELOPING THE REHABILIT A nON PLAN 45
ability of the objectives in light of the evaluation. Discrepancies in findings
across clinical disciplines and across situational observations are not unusual,
and they are presented here to determine if there are explanations for the
inconsistencies. Following this, each clinician will present what he or she sees
as the significant skill strengths, deficits, and behavior problems which, al-
though not necessarily part ofthe referral objectives, are important for optimal
independent functioning of the individual. Thus, this meeting is an oppor-
tunity for cross-disciplinary sharing and clarification of evaluation data.
This is followed by the process of rehabilitation planning, which involves
the entire team including the client, family, referring agency, and clinical
disciplines involved in the evaluation. In general terms, this planning session
involves the following: group summary of the quality of life at present, a
discussion of the evaluation findings and materials, identification of the op-
portunities and barriers for enhancing quality of life, sharing specific images
of a desirable future, identifying a tentative action plan for overcoming any
barriers, and identification oftentative but specific strategies toward realization
of desired outcomes. More specifically, the process begins with a statement
ofthe referring objectives and a description ofthe current functioning levels
of the client across the domains relevant to those objectives. Clinical team
members in presenting preliminary evaluation data, give their opinion as to
whether the referring objectives are achievable and appropriate. If there is a
discrepancy between referring objectives and current evaluation data (e.g., if
an objective seems unachievable because of a critical skill deficit), then a
discussion and negotiation process takes place so that the discrepancy is clar-
ified and, where needed, new objectives are defined. At this point, clinicians
mayaiso suggest additional objectives that, aIthough not part of the original
referring objectives, are feit to be important for independent functioning and
improved quality of life. The purpose of the meeting is to achieve at least a
tentative consensus on the priority and type of objectives that will be the
focus ofthe treatment. It is rare that this consensus cannot be reached. 1fthis
does occur, however, then further evaluation around the specific problem
areas may be needed. If resolution still does not occur, continued treatment
by the particular clinical team or facility is inadvisable, and a referral to another
facility or agency should be made. Without consensus, there cannot be unified
participation in the treatment plan, and one or another of the participants
on the team will inevitably be dissatisfied with the outcome. If consensus is
reached, the next step in the process is to review the leaming style of the
individual and the treatment probes that have proven effective during the
evaluation process. From this information, tentative therapeutic strategies
will be determined along with situations that are most closely in line with the
treatment and objectives. The role of each clinician will then be determined,
and techniques for measuring treatment effects will be designated to evaluate
46 CHAPTER 3
the specific treatment strategies. Finally, the approximate times needed to
carry out the plan will be suggested.
The next and final phase of the rehabilitation planning process can be
conceptualized as a diagnostic-prescriptive period. Having analyzed the in-
dividual's pre- and postinjury history, along with formal and situational eval-
uation information, the clinicians now implement treatment strategies in those
situations in which the client is most likely to learn the skills needed to enhance
independent functioning. These strategies may include self-instructional, self-
monitoring, external memory aids and cuing devices, reinforcement systems,
organization and time management for activities, or modifications in the
physical and social environment. As stated above, they are based on brief
interventions that clinicians have made during their evaluations and that
seem promising. They will now be applied for a longer period (e.g., a few
days to a few weeks) to determine if they are effective in terms of helping
achieve the objectives and to determine if the effort needed is justified by the
outcome obtained. Most importantly, they are examined for their general-
izability and practical usability in the environments in which the client will
ultimately live.
Depending on the objectives and treatment strategies, the clinical team
will meet again after abrieftime (usually not more than 2 weeks) to evaluate
the efficacy of the treatment probes and to reexamine the objectives to see if
additional modifications are needed. If, for example, use of a memory device
or cuing strategy would seem to substantially improve the person's skill ac-
quisition, then objectives previously rejected might be reconsidered. 1fthis is
the end ofthe individual's contact with this particular team or facility, then
the team will meet and summarize their findings and make detailed recom-
mendations for subsequent treatment. If the individual is to remain in this
particular rehabilitation setting, then a form of this process continues on
throughout the training and teaching period. Regardless of the teaching or
treatment environment, the objectives are stated in measurable terms, and
the measurement criteria and techniques are given. The treatment techniques
are specific, and approximate times are given at which objectives would be
expected to have been accomplished. Ifthese are long periods oftime (e.g., a
year), then interim short-term objectives or subskills should be given and
evaluated at 1- to 3-month intervals.
The outcome of the evaluation phases and the information-gathering
process is a specific rehabilitation plan in the form of a document (a sampIe
format for the recording ofthese data is provided in Appendix A). This working
document contains all of the critical data along with the specific objectives
that will be pan ofthe ongoing rehabilitation plan. In terms of the format of
this document, it can be organized around the totality of environments or
situations in which the person operates. Thus, skills and behaviors in domestic,
DEVELOPING THE REHABILITATION PLAN
47
vocational/educational, recreational, and community domains must be
broadly considered to ensure maximum functioning.
Within each domain, the team delineates those environments that are
most relevant to the dient based on the objectives. Thus, in the domestic
domain there might be a specific horne or apartment, and in the vocational
domain, a specific location and type of job. Once these broad domains have
been identified, then smaller or subenvironments within each domain must
be delineated. For example, a kitchen or bathroom should be considered a
subenvironment of the horne environment. Again, the subenvironments se-
lected for analysis are based on the dient's objectives and stated needs. Once
the relevant subenvironments have been selected, then those activities that
occur within the subenvironment that are of key importance to the person
must be specified. For example, meal planning, cooking, or deanup might
be priority behaviors in the kitchen. By proceeding in this fashion of increasing
specificity, evaluation and treatment are made more effective and efficient
since the precise areas of need are the focus of attention, while other related
areas that may not be problematic or irrelevant to the dient are omitted.
Once these activities have been defined, it is necessary to state the specific
skills required to participate in each activity. That is, the cognitive, motor,
and language skills necessary for successful completion of the activity are
given. The dient's performance in this activity is then compared with the
skills necessary for successful completion. The result is an analysis of the
discrepancies between the dient's current skills and the skills needed for
successful performance. The analysis reveals the barriers to be overcome
if the person is to succeed in that activity. Depending on the abilities of
the dient determined in earlier phases of the evaluation, it might be de-
termined that the skills simply could be taught. If this were not possible,
however, an adaptation might need to be introduced into the environment
(e.g., adaptive device) or for the dient (e.g., memory aid) that would assist
hirn or her in the performance of the activity. This process continues
throughout each domain of relevance to the dient. An example of a working
document for a particular environment and subenvironment is shown in
Figure 3.4. It is part of a plan developed for a severely head-injured
lO-year-old boy.
The use of this format ensures that all major domains and environ-
ments of a person's li fe will receive consideration. Within each domain,
the breakdown to subenvironments, activities, and skills allows for a
higher level of specificity or task analysis so that, at any given time, the
skills ofthe dient and the next required step in the teaching or adaptation
process are readily apparent. Thus, there is a built-in measurement feature
to chart progress toward an objective level of functioning within the
environment.
48
CHAPTER 3
Dornain: Dornestic
Environment: Horne Subenvironment: Kitchen
Subenvironment Oient
Barrier Objectives
TukAnal)"is lnventory
Activily. Preparation
To impro .... e skills related to meal
preparation.
Skills:
I) Will partidpate in a food
preparation prograzn.
ldentiiy food products
-
Needs verbal prompt>.
Will begi.n to develop disol.!nination
vs. non-food. between food. versus non-fooG..
Brings food products 10
Will gather food required to
Gathe: ingred.ients together. +/- counter, requlres verbal
prepare his Oleal.
prompts.
ldentiiy wolOng u_ils
-
Needs verbal prompts.
Will begin to iden'iIr cooki.'g
utensils.
utensils, plates, glasscs, etc.
Requil"es physical assistanre
Will begin to'stir, spread, serve,
Stir, POUJ', spread, scrape. -
to initiate and follow
with verbal prompt::s.
through.
Open. dose o:mtainen, Jars, box ..
-
Attenpts; need, pJry.ia.l
Will require pl'OI:"Ipts to turn hot
plastic cartons, mill: containers.
prompts to follow through
vs. cold faucet.
with physical skill.
Need, physia.l assist to
Using a designed like
Discri.minate hot vs. cold. - adjust temperature and flow
place 5etting, will set place properl y.
of wate!.
Respond to simple, single lnoonsistent,. needs verbal
2) To improve communication skills
action commands.
-
physical.prompl
dlL..mg Oleal preparatior..
Will gain and
Set table. -
Brings utensil to table.
accuzacy at following simple,
single-5tep com.mands.
lndicate choices using
-
lncom.istent.
Will gain use of appropriate
comrounication. spontaneous rommunication.
lndiC3.te need for help. -
lnconsistenl
Will gain use of speech to
indicate help.
FIGURE 3.4. Environmental performance analysis,
SUMMARY
Evaluation in the Natural Environment
1. The evaluation process can be divided into three distinct components:
(a) observation ofthe dient in his or her horne and community, (b)
discipline-specific assessments, and (c) situational assessments,
The Client in the Natural Environment
2. If there is an expectation that the dient will ultimately return to the
same community or situation from which he or she is being referred
for treatment, then the evaluation should begin in that situation.
DEVELOPING THE REHABILIT A nON PLAN 49
3. Frequently the cultural, community, and peer group expectations
to which the dient is subject may be quite different from those of
the rehabilitation setting or personnel.
4. Specific preinjury history needed to complete a comprehensive eval-
uation indudes medical history, educational history, vocational his-
tory, and psychosocial history.
5. Subsequent to completing apremorbid history, a detailed history
since the injury is taken. Information throughout the acute stages
of rehabilitation and information on the course of recovery are gath-
ered.
6. Once sufficient information is gathered on premorbid history and
acute stages of rehabilitation, interviews are conducted with the dient,
family, and referral sources. The purpose of these interviews is to
obtain specific information that will be used to develop objectives.
Formal Clinical Assessments
7. The social worker initiates the evaluation process by compiling a
detailed psychosocial history. The evaluation indudes family history,
values, and dynamics along with the support systems that surround
the family. The social worker also begins the identification of available
resources and support systems that will be part ofthe discharge plan-
ning process.
8. The occupational therapist's evaluation focuses on skills of activities
of daily living and independent living skills, whereas the physical
therapist is responsible for evaluation of the dient's physical status
as it relates to the ability to move and carry out activities.
9. The speech therapist evaluates communication across four categories:
phonology, semantics, syntax, and pragmatics.
10. The vocational specialist examines the interests, aptitudes, and psy-
chological attitudes of the individual as they relate to the world of
work.
11. The neuropsychologist carries out a comprehensive assessment of
the cognitive and emotional status of the dient. This entails evalu-
ation ofreasoning skills, memory, attention, language, visual spatial
and constructional skills, information processing and response speed,
auditory perception, tactile perception, academic achievement, and
personality assessment.
12. The team nurse is responsible far reviewing current medical infor-
mation and physically evaluating the dient. Additionally, the nurse
assesses the general health status of the dient, and reviews medical
routines that have been prescribed for health maintenance.
50
CHAPTER 3
Situational Evaluation
13. Clinical assessments alone are not sufficient for rehabilitation plan-
ning. In fact, the structure, cuing, and nurturing provided by clini-
cians as they carry out formal evaluations may compensate for and
to some extent mask the very deficits that are most often seen in
head-injured individuals.
14. The types of situations in which the client is evaluated will depend
on his or her entry-Ievel behaviors and objectives that constitute the
reason for the referral.
15. Only by conducting observational evaluations in "live" situations
and environments can hypotheses be made about the treatment to
be selected and the nature of the skill deficit.
Final Outcome
16 .. Following completion of evaluations, the team clinicians meet for a
comparison and review ofthe evaluation data. Discrepancies in find-
ings across clinical disciplines and across situational observations are
not unusual.
17. When discrepancies between referring objectives and current eval-
uation data exist, then a discussion and negotiation process takes
place so that the discrepancy is clarified and, where needed, new
objectives are defined.
18. Depending on the objectives and the types of treatment strategies,
the clinical team will meet again after a specified period of time to
evaluate the efficacy of the treatment and to reexamine the objectives
to see if additional modifications are needed.
4
The Daily Routine
The teaching and learning ofbehavior are taking place around us all the time,
and we usually do not notice them. Thus, it appears that people learn to
behave without outside influences. Although most of us do not realize that
we are teaching and learning, the process is going on almost continuously in
the social interactions within various environments. Not all the behaviors are
those that you would call "socially desirable." Bad habits are learned and
taught just as readily as good ones. This can be particularly true in certain
families and rehabilitation environments.
It is easy for those of us who are responsible for teaching clients with
head injury to be overwhelmed by the array of problem behaviors that some
individuals have developed over the years and to focus on teaching these
individuals to stop such behavior. What are some ofthe conditions that pro-
mote this captivation by problem behavior?
First, there is the tendency to be attracted to the unusual or bizarre and
to ignore the usual. When entering a room, for example, it is more likely to
look at someone disrobing than to notice someone looking at a magazine.
Unusual events in the social environment attract our attention and are "more
interesting," as are unusual events in the physical environment (sudden noises
or changes in illumination). This is an occupational hazard in human services.
To be effective teachers, the staff must recognize that the skillful use of attention
is a potent teaching tool and learn to use it wisely.
Second, there is often a formal mandate by the administration to attend
to misbehavior. Supervisors may require that staff observe, record, write about,
and discuss problem behavior. This institutional practice directs attention to
inappropriate behavior at the expense of desirable behavior. Such supervisory
practices must be redesigned before attention can be focused on appropriate
behavior and consideration given to teaching it.
51
52
CHAPTER 4
Third, predominant child-rearing practices of a culture (e.g., middle-
dass, United States) may direct attention to problem behavior. Most of us
learn to teach children by punishing misbehaviors rather than presenting
models of desirable behavior and reinforcing approximations to their ideal
performance. This focus on punishment is reflected in the "spare the rod and
spoil the child" approach to child-rearing. Also, public pressure may encourage
parents to attend to the problem behaviors of their children, a fact that can
often be confirmed by casual observation in a supermarket. Arehabilitation
facility may be subject to the same kinds of public pressure when neighbors
call to complain of loud noises, aggressiveness, or disrobing in the yard.
DESIGNING ROUTINES OF DAILY LIVING
From research, we know that it is difficult for an individual to stop be-
having inappropriately in a situation until he or she learns an alternative way
ofbehaving in that situation. Attempting to eliminate maladaptive behavior
before beginning to teach alternative behavior is neither a necessary nor suc-
cessful approach.
There is a tendency in many rehabilitation facilities to define appropriate,
alternative behavior through the definition of the problem behavior: the ap-
propriate alternative is the opposite of the problem behavior. For example,
the opposite of falling to the floor in atemper tantrum may be defined as
sitting quietly in achair with hands folded. Another common tendency is to
accept and reinforce any behavior other than the problem.
In arehabilitation facility, however, the appropriate alternatives to mal-
adaptive behavior are those behaviors that are compatible with a culturally
accepted routine of daily living. A daily routine composed of randomly de-
termined opposites to inappropriate behavior will indeed be a bizarre one.
The design of an acceptable daily routine is, therefore, crucial to the devel-
opment of a rehabilitation environment that emphasizes teaching. The daily
routine specifies the behavior that dients are learning and practicing 24 hours
a day; they constitute the culture practiced by arehabilitation facility. For
these reasons, the design of the daily routine is said to be the "anchoring
point" of program development. The daily routine is the positive teaching
program of arehabilitation facility, and its design shifts the focus to the de-
velopment of acceptable behavior.
Components 0/ Daily Living
Every residential facility has a daily routine. The daily routine is a se-
quence of daily events within the facility that is common to the group. In-
THE DAIL Y ROUTINE 53
dividual routines vary from one another within the context of the common
routine.
The daily sequences ofbehavior that are common to the group are made
up of observable events or components. Components are behaviors in the
daily routine that occur repetitively, e.g., awakening, showering, dressing,
eating, doing house jobs, recreating, and so forth. The following is a repre-
sentative list of components from a sequence from a community-based group
horne:
AM components
Wake up
Toilet
Shower
Dress
Clean room
Fix breakfast
Eat breakfast
Clean up after breakfast
Brush teeth
Meet bus
PM components
Arrive horne
Community meeting
Housejob
Group activities
Meal preparation
Dinner
Groupactivities
Bedtime preparation
Bedtime
Listing the components and sequences of the routine does not signify
that the routine is fixed and regimented. For example, during the week when
dients go to school or work and there are time constraints, some components
may be shifted in sequence, shortened, or dropped. On the weekend, the daily
routine may be more relaxed, more complete teaching may be occurring, and
the components may be more spread out over time. Variations of components
may be seasonal. During the summer when school is out, a daily routine may
contain different components than during the winter. Variations mayaiso be
related to special events, e.g., holidays, vacations, parades.
Evaluation 01 the Daily Routine
Although every facility has some sort of daily routine, the routine may
not be one that prornotes the leaming of normal, culturally acceptable be-
haviors. In many cases, the routine of a dient evolves over time in response
to a variety of circumstances and has never actually been designed to teach
appropriate behaviors.
It will help the designing of a routine if the people collaborating on it
will first develop the major behaviors that they agree are important to teach.
Once these behaviors are identified and defined, they can be arranged into a
54
CHAPTER 4
culturally acceptable sequence. The sequence of behaviors constitutes the
proposed chain and provides a framework or pattern against which the daily
routine can be evaluated or modified. The evaluation involves (1) observations
ofbehavior in the current routine and (2) identification ofteaching deficiencies
in the current routine.
Observations in the Current Routine
Through observation, one identifies behaviors that dients are learning.
The components provide the context of observation. Suppose, for example,
we begin by observing the "wake up" component in the morning. We see
direct care staff enter the bedroom, turn on the lights, and say, "Good morning.
Time to get up. Stand up and go to the bathroom, please." The clients stir,
open their eyes and make eye contact with the staff, but remain in bed. After
a few minutes, the staffmember returns and says, "Good, you're awake. Get
up and go to the bathroom now, please." The dients comply. From this
observation, we see that clients in this facility have learned to wake up when
the lights go on and the staff greet them. They have also leamed to remain
in bed until a staff member returns to instruct them again to go into the
bathroom. Is there anything wrong with this routine? Not necessarily. Some
people, for instance, may consider it an inappropriate routine for young chil-
dren. A staff member may consider this routine a wonderful improvement
over earlier times when dients were highly resistant and even combative when
attempts were made to get them out of bed.
Suppose these are adult clients preparing to move into independent living
situations. In this case, observers may agree that they can and should learn
to set and wake to alarm docks. To teach these new behaviors, both the bed
preparation and the wake up components of the routine will have to be re-
formulated.
In designing a daily routine, similar observations should be made across
all behaviors of the current routine. In each instance, observers must ask,
"What behaviors now occur in this component of the routine? Are these
behaviors good for the dient to leam? If not, what behaviors should this
component of the routine be teaching?" When these observations are com-
pleted and summarized, the staff will have some new ideas about changes to
make in the current routine and list the specific behaviors to add to the com-
ponents of the proposed routine.
Most behaviors cannot be designated acceptable or inappropriate without
the knowledge oftheir contexts and circumstances. Behavior that is desirable
in one component may be inappropriate in another. Removing one's shirt,
for instance, is okay at bedtime, but not usually at mealtime. The social
significance of the behavior depends on its sequential position in the daily
THE DAIL Y ROUTINE 55
routine. A behavior may be a problem beeause it is out ofthe normal sequenee
of events. A deseription of the form of the behavior (topography) or its fre-
queney may not be suffieient to define it as maladaptive. The appropriateness
of a behavior also depends on the eomponent of the daily routine in whieh
it oeeurs.
Identification o/Teaching Dejiciencies
Observations of and discussions about a routine may reveal a number
of problems. The following are typical:
1. Missing components. Example: Food is purchased, prepared, and
served for the clients. With little opportunity to partieipate in these
normal, daily events, clients do not learn these skills and remain de-
pendent on others.
2. Abnormal sequences. Example: A client is taught the sign for water
in training sessions at 3:00 PM. The client learns to sign water when
it is presented at training, but not when thirsty.
3. Component behaviors not taught. Example: A daily routine contains
several "free-time" and "leisure-time" components. The rationale for
these components is that "clients should have time to do what they
choose." Yet no one teaches the clients to look at magazines, engage
in cast aetivities, or even to watch television. Clients do not learn to
do or to ehoose.
4. Absence 0/ common routine components. Example: Routines of the
clients are so highly individualized that no opportunities are presented
for group activities. Clients do not learn group living skills such as
sharing, co operating, and taking turns.
Characteristics like these should be noted during the review of the present
routine and correeted in the proposed routine.
Developing Teaching Opportunities in the Daily Routine
In the analysis of the daily routine, eaeh eomponent is comprised of a
setting and a set of behaviors eommonly recognized as normal, benefieial,
and eulturally appropriate to the time and plaee. From the standpoint of
teaehing staff, therefore, eaeh eomponent presents extensive opportunities for
teaehing. Opportunities for teaehing and learning are, of course, two sides of
the same eoin so that the daily routine also eontains unlimited potentials for
learning. A residential facility is obligated to formulate components of living
that continually give clients the option to learn.
56 CHAPTER 4
Component Descriptions
In designing a daily routine, it is useful to consider each component
separately and to specify the teaching functions it contributes to the overall
design of living. Descriptions of each component verify for staff, clients, and
family the purpose and general procedures of the component, and the op-
portunities for teaching that it offers.
The following is an example of a component description for the com-
munity meeting in a group home with eight people who have brain injuries
and live-in, married, house parents who are relieved on weekends. This de-
scription includes (1) the name ofthe component, (2) a statement ofpurpose,
(3) a briefdescription ofprocedures, (4) a list ofteaching opportunities, i.e.,
learning options.
COMMUNITY MEETING
Pur pose
The community meeting is a teaching activity that establishes the social
interactions of clients and staff with each other. Because clients are often
excited or upset when they return from school or work, the community meet-
ing also can serve to reintegrate people into the routine. The meeting is an
opportunity for staffto access the status of each client, to communicate with
each other, and to plan.
Description
As they get off the bus, clients are greeted by one of the house parents.
The other house parent is stationed inside the door. This house parent also
greets each client and gives any necessary instructions for toileting and chang-
ing clothes. Clients are instructed to assemble at the dining table for "a meet-
ing." At the meeting, the clients and house parents sit together, have snacks,
review the day's happenings, discuss house-job assignments, and plan for
later events such as dinner and recreational activities.
Teaching Opportunities
In this component of the daily routine there are opportunities to teach:
Attending: e.g., eye contact, listening.
Fine and gross motor skills: e.g., pressing a pitcher of juice, pouring,
setting out snacks, taking "just one."
THE DAIL Y ROUTINE 57
Following instructions: e.g., "Look," "Listen," "Come here," "Sit
down," "Please pass .... "
Social interactions: e.g., passing, sharing, taking turns, helping.
Language: e.g., reading, names and descriptions of people, objects,
events, questions, conversation, and recall.
The list ofteaching opportunities contains many behaviors often selected
as objectives for people with brain injuries. One important advantage of com-
ponent descriptions is that they indicate to direct care staff when and where
the behaviors can be taught during the course ofthe day.
Types ofTeaching Interactions
Teaching opportunities are characterized by the forms that teaching in-
teractions take. Three types ofteaching interactions may be distinguished and
combined to develop a daily routine with maximum teaching potential: (1)
planned, (2) incidental, (3) coincidental.
Type 1: Planned Teaching Interactions
In this type ofteaching interaction, the occasion, teaching strategy, and
performance criteria are planned ahead of time. This type is probably the
most familiar. Planned teaching objectives and strategies are based on an
assessment of the client's learning needs, an analysis of the responses and
skills involved in the objective, and the knowledge ofthe current competence
of the learner.
The components ofthe daily routine provide the framework from which
we select occasions for planned teaching. Any event in the course of daily life
may be selected: self-care, household maintenance, recreation and leisure,
social and community events. Even though the teaching strategy is planned,
care must be taken that the teaching interaction occurs within the normal
sequence of daily life.
Type 2: Incidental Teaching Interactions
By definition, incidental teaching interactions are not planned and may
occur incidentally to almost any activity during the course of daily living. To
illustrate, let's return to the description ofthe community meeting component
earlier in this section. The staff members may plan certain teaching strategies
for that component: to teach one client to ask for juice; another, to grasp a
plate and pass it; yet another, to wait his or her turn, and so on. Simultaneously,
the situation incidentally permits the teaching oflanguage, social interactions,
58 CHAPTER 4
a variety of motor skills, and many other behaviors. It would not be possible
to predict and plan for all of the possible teaching opportunities that might
arise incidentally during a community meeting.
One definable characteristic of incidental teaching interactions is that
they are often initiated by behavior ofthe clients. Incidental teaching involves
the skill of observing and responding to the behavior of the student while
grasping the moment to extend or elaborate competencies. A client is watching
TV. A passing staff member stops and says, "What is that? That's a white
horse, isn't it?" Another client is having difficulty using the spray bottle of
glass cleaner. A staffmember approaches and says, "Here, let me show you."
(Demonstrates) "Now, you try it. Good! You got it." A staff member is helping
a client dress: "Y ou're putting on your red shirt. Is that the one with the
alligator on it? Right, there's the alligator."
Incidental teaching is critical to the success ofteaching at arehabilitation
facility. Incidental interactions make the socia1life of the facility pleasant,
lively, and effective and introduce variations into what, at first glance, look
like repetitive sequences in the daily routine.
Type 3: Coincidental Teaching Interactions
Certain events are always intruding on the daily routine that are unique
and that staff members leam to handle on the spot-a fuse blows, someone
cuts his finger, the sink clogs, a tire goes flat. Ifstaffknow exact1y what to do,
then these are unique opportunities for incidental teaching. But suppose one
does not know what to do or what is going to happen. In these situations,
staffhave the opportunity to teach what to do when one does not know what
to do: to stay calm, review the options, figure it out, get help (problem solve).
These are mutual leaming interactions in which both teacher and student
leam something new. Coincidental teaching interactions are lessons in leaming
how to leam or problem solving.
DEVELOPMENT OF TEACHING COMPETENCE
A good way to begin formulating teaching opportunities is to plan Type
1 teaching interactions for a single component ofthe daily routine. So me staff
members may want to select for change the most difficult behavior in the
routine. Consideration should be given, however, to the experience of staff
members and competence of clients. The planned activity should be easy
enough for staff and clients to perform reasonably successfully. Through the
process of designing, trying out, evaluating, and redesigning an activity, staff
leam to teach the essential behaviors and gain competence from guided, prac-
THE DAIL Y ROUTINE 59
tical experience. Clients, too, learn essential behaviors ofthe component and
gain competence from staff members' support.
As staff and clients acquire more experience, the original activity may
become elaborated. Over time, variations in activities within a single com-
ponent can be designed, implemented, evaluated, and redesigned. As the pro-
cess continues, the skins ofthe rehabilitation staff expand through experience
with varied activities. The skins of the clients also expand as they gain ex-
perience with more sophisticated and varied activities.
The skins of the staff can be expanded to other components of the routine
as they gain experience in various planned teaching opportunities within the
training component and with the process of designing, evaluating, and rede-
signing activities. Certain skills of the clients also may be used in similar
components of the daily routine.
By planning a simple activity in each component of the daily routine, a
stable foundation is established for building more varied and complex activities
that over time, can increase the teaching potential of the daily routine. Also,
planned, basic activities can be designed for each component of the daily
routine that can be managed by a minimum of staff members during staff
shortages.
As stafflearn and practice planned teaching, they also begin to recognize
and take advantage of incidental opportunities to teach behaviors. With
teaching skills sharpened through experience with planned teaching activities,
they can better observe and respond to behaviors of clients. Staff also will
learn to recognize recurring patterns of coincidental events and reduce the
disruption to the daily routine that these events bring. For example, if the
bus is frequently late in picking up clients for school or work, then this recurring
event can be taken into account in the design ofthe daily routine and activities
can be provided to teach clients what to do while waiting for the bus.
For the experienced staff member, almost all teaching is Type 2 so that
he or she moves through the daily routine seizing the opportunities for inci-
dental teaching that are continuously available. Intrusive, disruptive, coin-
cidental events that force a teacher to develop a new way to teach occur less
often, not because the day has become more routine, but because the staff
member is mastering incidental teaching, and clients are mastering incidental
learning.
Furthermore, variations are always occurring within the routine. Vari-
ations in food, dress, housework, leisure time activities, and community out-
ings produce stimulating experiences that are not merely stereotyped repetition
of preceding days. Nor is it a matter of visually repeating every component
every day. We have intentionally avoided suggesting that time units be assigned
to each component because we do not want the reader to assume that the
community meeting must stop at 3:29 PM and house jobs begin at 3:30 PM.
60 CHAPTER 4
If the meeting is going weIl and people are engaged in new social behaviors,
keep it going and forget about house jobs. If everyone is having a terrific time
working together on house jobs, forget about dinner preparation. Send out
for pizza!
RELATING INDIVIDUAL AND GROUP ROUTINES
Individual routines may vary from one another within the context ofthe
daily routine. Sometimes individual routines become so highly variable that
a daily routine for the group is impossible. The lack of congruence between
individual routines may become a problem. For example, consider the com-
ponent prepare and eat breakfast. Different groups of clients may prepare and
eat breakfast at different times throughout the morning. Though breakfast is
a common event, it is not common to the group as a whole, as it is when
everyone prepares and eats breakfast together.
There is no need for a common breakfast component
1. When clients are capable of preparing and eating breakfast on their
own
2. When clients are capable of cooperatively preparing breakfast ifthat
is desired or necessary
3. When the group of clients is small enough for everyone to prepare
and eat breakfast individuaIly, without bumping into each other in
the kitchen
In most rehabilitation facilities, independent behaviors are usually not
characteristic of the dient. More often, they need to learn behaviors such as
preparing and eating breakfast, and group-living behaviors such as coopera-
tively working together on something. Also, groups of five to ten dients may
make it necessary to teach these living skills simultaneously.
The fact that groups of dients are living together and have common
needs forces the integration of individual routines. There must be an oppor-
tunity for the daily routine for dients to live and work together. Individual
routines must be consistent, at least during some part of the day, with the
routine of the group.
Highly individualized routines force "one-on-one" (one staffjone dient)
teaching strategies. "One-on-one" teaching strategies are inadequate for
teaching group living skills. "One-on-one" teaching, although attractive at
first glance, actually fractures the normal sequences of events in the daily
routine because there are fewer staff to be deployed throughout the daily
routine than there are dients. "One-on-one" teaching forces a certain number
of clients to wait while others are in their "one-on-one" teaching sessions.
THE DAIL Y ROUTINE
61
For the dient, the sequence of daily events becomes the series of "one-on-
one" training events followed by waiting. This is anything but a normal routine
ofliving.
SUMMARY
Designing Routines of Daily Living
1. It is difficult for an individual to stop behaving inappropriately in a
situation until he or she leams an alternative way of behaving in
that situation. To attempt to eliminate maladaptive behavior before
beginning to teach appropriate, alternative behavior is not a successful
approach.
2. In a residential environment, appropriate alternatives to maladaptive
behaviors are those that are compatible with a culturally appropriate
routine ofliving.
3. Every rehabilitation environment has a daily routine. The daily rou-
tine is a sequence of daily events within the environment that is
common to the group.
4. By directly observing dients participating in daily activities, it can
be determined what behaviors have been learned or not learned.
5. Most behaviors cannot be designated appropriate or inappropriate
without knowledge oftheir context and circumstances in which they
exist. That is, behavior that is appropriate in one environment or
situation may be inappropriate in another.
6. Four common daily routine deficiencies are: the routine is missing
components, the routine has an abnormal sequence, the routine does
not allow for teaching component behaviors, and absence of common
routine components.
Community Meeting
7. The community meeting is a teaching activity that establishes the
social interactions between dients and staff. The meeting provides
the opportunity for staff to leam the status of each dient, to com-
municate with each other, and to engage in planning activities.
8. Three types of teaching interactions can be distinguished: planned
teaching, incidental teaching, and coincidental teaching.
9. Planned teaching sessions are scheduled in advance and involve
teaching to specific situations and tasks. Planned teaching sessions
62
CHAPTER 4
are scheduled on a regular basis and are not contingent on clients'
behavior.
10. Incidental teaching interactions are not planned and may occur in-
cidentally to almost any activity during the course ofthe day. Inci-
dental teaching interactions are usually initiated by the behavior of
the clients.
11. Coincidental training occurs when staff are placed in a situation to
teach when neither client nor staff know what to do. Coincidental
teaching interactions are lessons in learning how to leam.
Development ofTeaching Competence
12. It is recommended that new teachers begin practicing teaching skills
by engaging in planned teaching interactions. Initial teaching situ-
ations should be easy enough that both staff and client obtain success.
13. For the experienced residential teacher, almost all teaching consists
of incidental interactions. Disruptive coincidental events will decrease
because the teacher is mastering techniques of incidental teaching
and clients are mastering the techniques of incidentalleaming.
14. Variations are always occurring within the components ofa routine.
Variations of food, dress, housework, leisure-time activities, and
community outings produce stimulating daily experiences that are
not necessarily repetitive.
Relating Individual and Group Routines
15. Frequently individual routines become so highly variable that a daily
routine for a group is impossible. The lack of congruence between
individual routines may become a teaching problem.
16. There must be an opportunity in the daily routine for clients to live
and work together. Individual routines must be consistent, at least
during some part ofthe day, with the routine ofthe group.
5
Staff Training
Most rehabilitation facilities cannot maintain a full staff while new personnel
are in training. They tend, therefore, to suffer from two related and chronic
conditions: (1) a high frequency of turnover and (2) crisis training. Crisis
training occurs when experienced staffleave and new personnel must assume
responsibility for clients as soon as possible. Crisis training tends to be poorly
designed and fragmented. Inadequate training results in additional stress,
which, in turn, increases the frequency ofstaffturnover. Thus, many facilities
are caught in a cycle of perpetual crisis.
When considering staff training, it is important to distinguish between
the transmission of information and the learning of skills because a person
may have access to information and lack skills to perform adequately. Crisis
training most often emphasizes transmission of information. New personnel
may be placed in an environment with no real skill training and only such
information as can be gleaned from the facility's policy handbook and a few
orientation sessions.
This chapter on staff training will emphasize development of skills through
practicum training. This emphasis is not to imply that information training
is less important, but rather, to suggest that skill training is currently in greater
need of development. Books, audiovisual materials, and in-service courses
are now available that introduce trainees to the history and nature of head
injury and to a wide array of techniques for treatment. No such sources,
however, can teach personnel how to work with specific individuals in specific
circumstances. This requires practicum training processes.
TUTOR/AL PROCESSES
Primarily, practicum training enables new staff to participate in reha-
bilitation routines usefully and effectively. This integration is accomplished
63
64 CHAPTER 5
through aseries of experiences under guidance from knowledgeable
staff. After a day or two of directed observation, new staff work alongside
experienced staffwho provide the necessary models, coaching, feedback, and
reinforcement. In these tutorial processes, new staff members acquire essential
skiHs from their peers, those around them who already possess necessary skiHs;
in other words, this is apprenticeship.
Both trainee and trainer must bring certain abilities to the tutorial situ-
ation. The trainee must be observant and willing to try new behaviors. He or
she must exhibit curiosity about work: ask questions, listen, follow instructions,
and acknowledge feedback. The trainer must use the same basic skills applied
in the tutorial interactions with clients: guided observation, modeling, coach-
ing, observing, and providing feedback. The following sections review these
basic teaching skills and describe their application in tutorial staff interactions.
Guiding Observation
Most new staff are unaccustomed to learning in the natural environment
and may need preparation. Trainers orient trainees before entering the en-
vironment by describing what there is to be observed: "What you will be
seeing is ... ," 'TH be talking to you about. ... " Trainers encourage trainees
to carry a notebook and write down for later discussion questions that occur
during observation. Trainers prepare trainees for interactions with dients:
"When the dients greet you, just say, 'Hi, nice to meet you,' as you would
to anybody and shake hands. If the dients ask you why you're here, just say
you're here to see how they make spaghetti."
Observing
Observing in natural environments does not require one to be an "in-
visible" nonparticipant as in most traditional research studies. Participation
in ongoing activities is often necessary and desirable; e.g., when clients greet
visitors, ask questions or invite one to dinner. In natural settings, there are
no hard-and-fast rules concerning when one should or should not participate
in activities. Some guidelines, however, for observers in training will help
them preserve the naturalness of ongoing events. (1) Respond as you would
naturally to similar circumstances (introduce yourself, answer questions), but
do not say things that prolong conversation. (2) Move to a background position
as soon as possible and remain there. (3) Pick a position that does not disturb
the activity but still allows you to see. (4) Avoid positioning yourselfin door-
ways or in front of windows. (5) Keep a low profile; sit, if possible. Don't
attract dient or staff attention. (6) A void prolonged eye contact with dients.
(7) Talk in a low voice; point and use gestures discretely.
STAFF TRAINING 65
Directing Attention
During guided observation, trainers direet trainees' attention to specifie,
eritical events either verbally or by discrete gesture. "Look at Seott and Steven"
(trainer points). "See how Steven is holding the bowl while Seott stirs." "Listen
to George" (points to George, a staff member). "You heard George say, 'Steve,
you're holding the bowl for Seott.' George is reinforcing eooperation by de-
seribing behavior."
Establishing a Language
Through guided observation, trainers establish a language of instruetion.
By labeling, trainers teaeh trainees names for the events observed: "That's a
prompt." "That's a model." "George is prompting that behavior." Trainers
label eomponents of the residential routine and their essential features: "This
is a eommunity meeting. George and Mary are team teaehing. Notiee what
Mary does as the lead; see how she. . . . Notice what George does as the
support; see how he .... Now, that's team teaehing!"
Debriefing
Immediately after the observation, trainers arrange for trainees to deseribe
the observations and ask questions. These diseussions eneourage trainees to
use and praetiee the instruetional language.
Modeling
Modeling is demonstrating new behavior for trainees. Whatever the be-
havior, learning is faeilitated by showing how it is performed. Trainers should
avoid asking trainees to perform behaviors that they have never seen.
Trainers either model behaviors themselves or arrange for eompetent
models. Trainers themselves need not be eompetent in everything to ensure
that trainees have essential learning experienees. If trainers know the eom-
peteneies of the entire residential staff, appropriate models ean be sought
when they are needed.
Modeling teehniques differ depending on whether trainees are expected
to imitate immediately. If the behavior is eomplex, only small segments are
needed before trainees perform. If trainees are not expeeted to imitate, but
only to observe a teaehing aetivity (e.g., leading a eommunity meeting), longer
and more eomplex behaviors may be modeled. In many eireumstanees, train-
ers model and guide observation simultaneously. Demonstrating operation
of a dishwasher, for example, a trainer might say, "After loading the dishes,
66 CHAPTER 5
take the soap from here" (takes the soap from the cabinet), "and put it in
here" (points to soap pan). "Use this much" (pours small amount). "Press
the button labeled energy saver" (presses button), "and push in on the dial"
(pushes dial) "like that. And that's all there is to it."
When trainees have seen behaviors demonstrated and their observations
have been directed to essential aspects of performance, they are ready to begin
practicing under coaching conditions.
Coaching
Through coaching, trainers involve trainees in routines of residential
living. Coaching requires that (1) trainees participate in the routines and in-
teract with dients and other staff, and (2) trainers stay dose by to direct
appropriate behavior and redirect incorrect behavior.
Directing Appropriate Behavior
Coaching provides immediate direction. The trainer prompts the trainee
through a performance, e.g., "Say (this) ... " or "Don't do (that); do (this).
. . ." Coaching is a teaching interaction, not a social interaction. Coaches
may not have time for social niceties such as "please, " "thank you," and
"would you mind.. . ." They are directing trainees into appropriate behavior,
not engaging in social rituals. Trainees need preparation for coaching. "I want
you to try .... I'm going to be right behind you telling you what to do and
say. 1'11 need to be brief so I may appear impolite."
Redirecting Incorrect Behavior
Coaches do not let trainees engage in incorrect behavior. They anticipate
these behaviors if they can and stop them. Coaches tell trainees that they are
going to redirect, step into the situation, model, and guide trainees' obser-
vations of the appropriate performance. Coaches protect trainees. They do
not let trainees do anything that will frighten or embarrass them. They structure
experiences for success by starting with easier performances (e.g., the support
role in the community meeting), and moving to more difficult performances
(e.g., the lead role in a community meeting).
The following are some guidelines to basic mechanics of coaching: (1)
Stand behind the trainee and stay dose. (2) Whisper briefinstructions; don't
say too much. (3) Save long explanations and discussion for later debriefing.
(4) Use gestures and touch cues. (5) Give periodic encouragement to trainees
(e.g., "You're doing fine; hang in there").
ST AFF TRAINING 67
Observing and Giving Feedback
There is no sharp distinction between coaching and the next tutorial
interaction to be discussed, observing and giving feedback. The trainer grad-
ually fades from direct coaching of the trainee's performance to observing
and giving hirn feedback later about the trainee's behavior. As trainees acquire
skills, trainers will find direct coaching increasingly unnecessary. Rather,
trainees need someone to observe their performance (perhaps take notes) and
provide feedback regarding appropriate behaviors and alternatives to inap-
propriate behaviors. Feedback helps trainees become aware ofthe correctness
or incorrectness oftheir behavior. Feedback is a description of past behavior
with respect to a criterion. By observing and describing behavior, trainers
inform trainees about the adequacy of their performance relative to the cri-
terion. Part of the feedback is a description of appropriate behavior followed
by a description ofthe desired effect on the client's behavior. For example, a
trainer may say: "George, I heard you say to Jill, 'Good, you're peeling po-
tatoes,' while you prompted her behavior. That was very effective. I noticed
that she smiled and that a few minutes later she continued peeling potatoes
when you faded your prompt. Did you see that too? That's why we reinforce
clients' prompted behavior just as if they were performing on their own." By
looking for and describing strengths (appropriate behaviors), trainers help
trainees see relationships between their behaviors and the appropriate circum-
stances. Since positive feedback "feeis good" to most individuals, many people
believe this to be the main reason for giving it. But the fact that positive
feedback "feeis good" is only a pleasant side effect. Positive feedback serves
much more important functions than emotional stimulation. Describing
strengths helps trainees recognize their own effective behavior under a variety
of circumstances and the effect that their behavior has on that oftheir clients.
Corrective feedback provides the other half of the process needed to
establish trainees' recognition of effective artd ineffective behavior. Positive
feedback alone may not establish this discrimination efficiently. Corrective
feedback is a description of the inappropriate behavior and a description of
the outcome, followed by suggested opinion or alternative. For example, a
trainer may say, "Bob, I heard you laugh when Tom put his shoes on the
wrong feet. Don't do that. Did you notice that Tom started sulking and
wouldn't put his shoes on correctly when you asked hirn? We want Tom to
continue trying to put on his shoes even if he doesn't always do it correctly.
We want learning to be enjoyable for hirn. Next time, praise hirn for trying
and then show hirn which shoes go on the left and right feet."
Corrective feedback does not take the form of criticism or abusive cri-
tiques, which are common. Trainers do not give corrective feedback to punish
trainees or to make them "feel bad." Abusive practices allow trainers to vent
68
CHAPTER 5
their emotional responses to frustration but do not help the trainee. The
trainee is helped most when told what is inappropriate about his or her per-
formance and then told or shown what the appropriate behavior iso
When trainers cannot suggest a successful option for an ineffective be-
havior, they tell trainees so, and together they ask others, review research
literature, or develop alternatives through empirical investigation. The fol-
lowing are some guidelines for giving feedback: (1) Prepare the trainee. Tell
the trainee what you are going to do and why. The trainer might say, "As
part of your training, I will be observing you this afternoon to give you some
feedback on your performance. I'm not here to criticize, so relax and go about
your normal routine. 1'11 be looking for appropriate behaviors to describe
because I want you to continue them. 1'11 also be looking for incorrect or
inappropriate behaviors to describe, not to make you feel bad, but because I
want you to become aware ofthem. 1'11 be helping you to correct the incorrect
or inappropriate behaviors by giving you some options or alternatives. 00
you have any questions? Is there anything I can clarify?" (2) Be specific.
Describe exactly what was seen; avoid general descriptions. Contrast the fol-
lowing examples: (A) "Your instructions and follow-through were good." (B)
"Your instruction to Jerry, 'Take the milk to Mike,' was short and clear. You
waited until Jerry followed your instructions and then praised him with
'Thanks, Jerry.' Did you see Jerry smile? That's reinforcement and appropriate
behavior on your part. Reinforcement will help Jerry learn to follow instruc-
tions." (3) Be objective and understanding in giving feedback. Among other
things, this means avoiding emotionally charged words or phrases such as the
following: "You should have .... " "Some mistakes I saw you make were .
. . . " "I like the way you did ... , but you should have .... " Words like
"mistakes" or the phrase "you should have" frequently disturb listeners. The
word "but" tends to negate the positiveness of the first part of the feedback
statement. Describe what you saw, using "and" instead of"but." "When you
. . . (this good outcome occurred) and when you. . . (this outcome occurred).
In this situation you might try .... " (4) Give feedback immediately. Feedback
is more effective if given immediately after the occurrence of behavior, not
hours, days, or weeks later. If feedback must be delayed, refresh the trainee's
memory of the incident: "Remember yesterday at the community meeting,
before the hose broke on the washing machine and squirted water all over
the place (laughter). Iwanted to get back toyou and talk to you about some
things I observed in the meeting. Let's see, you were in the support role, sitting
between Jerry and Mike. Fred was talking about his home job and you .... "
(5) Select a setting for feedback that is conducive to clear communication.
For example, give feedback before clients come home or after bedtime. Don't
give extensive feedback when staff are working with clients.
ST AFF TRAINING 69
Video technology is an especially effective feedback device. Trainers and
trainees can view a single tape many times and study different aspects of staff/
dient behavior. The technology allows for immediate feedback during which
viewers can pause, back up, and repeat all segments. The production ofuseful
training tapes requires a knowledgeable camera operator who can focus on
important aspects of teaching interactions. Small format cameras are simple
to operate, and staff can readily add video skills to their training repertoires.
Most people are initially sensitive to the presence of video equipment so it is
important not to use the camera critically. Don't record mistakes that show
viewers in a bad light. Record events that viewers will be pleased to see so
that videotapes can function to reinforce appropriate behaviors. Later, vid-
eotapes may be used to give trainees an opportunity to evaluate their
performance.
Observation and feedback continue as routine features of staff interactions
and especially ofsupervisory activities; stafflearning does not stop at the end
of formal training. Supervisors continue to observe and inform staff about
their performance. This feedback cannot be predominantly negative, otherwise
staff will not welcome supervisory observation. Supervisors maintain appro-
priate staff behavior and morale by participating in rehabilitation routines
and providing mostly positive feedback regarding staff accomplishments.
Participating in the Daily Routine
Practicum training introduces new staff to routines of daily living and
enables them to participate, as soon as possible, in teaching,' naturally and
effectively. To accomplish these ends, other staffmembers in the facility assist
new staffthrough tutorial interactions whose essential features have just been
described. Through their tutorial experiences, new staffleam to (1) participate
in the routines of daily living, (2) teach brain-injured individuals, and (3)
recognize opportunities for teaching that arise naturally in the course of
rehabilitation.
Basic Information about the Routine
New trainees are easily overwhelmed by too much information given
too quickly. To avoid this, tutors must direct attention to information that
is immediately important and useful and order information according to
priorities. Do not, for example, merely hand trainees the official book of
policies and procedures with instructions to read it. With too much infor-
mation, trainees will be unable to discriminate high-priority from less essential
information. Some trainees may not read weIl enough to leam a great deal
from reading. In these ca ses, tutors must present information verbally or
70 CHAPTER 5
simplify reading assignments and design procedures to verify comprehension.
The following information is essential to a trainee's orientation: (1) design of
the daily routine and purpose of each component; (2) physicallayout of the
facility, including storage oftools, location ofthe fuse box, water main, etc.;
(3) standards of maintenance, e.g., what constitutes, in this facility, a clean
kitchen or a clean bathroom; and (4) nature of organization, e.g., how many
group homes it operates, organizational structure, location of offices, orga-
nizational history.
Basic Living Skills
Rehabilitation often fails because staff members do not have the routine
skills they are attempting to teach. Tutors must not assume that new staff
bring with them a full complement of routine living skills. Even trainees
experienced in everyday household maintenance may need guidance in the
procedures of a particular facility: "Toilets are cleaned in this home, this
way." "You light the pilot on this stove tbis way." "You turn on the washing
machine this way." Basic skills offacility living include (1) operational skills,
e.g., operating the dishwasher, oven, garbage disposal, vacuum cleaner; (2)
household skills, e.g., following a recipe, cooking, making beds, setting the
table; (3) maintenance skills, e.g., changing a fuse, cleaning a toHet, mopping
floors, mowing grass.
New staff need not appear to clients to know everything and should be
encouraged to learn from the clients: "I don't know; let's go ask," "Help me,"
"Tell me," "Show me." Most clients will know the routines better than new
personnel and can participate in tutorial training along with experienced staff.
In turn, new staff can model good learning: attend, thank clients for helping,
make mistakes without being embarrassed or defensive.
TEACHING CLIENTS WITH BRAIN INJURY
Staff training can be designed so that the trainees learn to teach clients
in much the same way they themselves are taught. Everything said to trainers
about staff training may also be said to staff about teaching clients. Guiding
observation, modeling, coacbing, and giving feedback are all techniques that
apply to teacbing clients. Because of their disabilities, however, these teaching
(tutorial) interactions must be modified to accommodate individuals with
different handicaps.
The following do's and don'ts are derived from the experiences of suc-
cessful rehabilitation staff. They are illustrations, not formulas; of course, they
ST AFF TRAINING 71
must be modified for different dients. They are not induded here simply to
be handed to new trainees but to guide trainers in choosing new personnel.
Guiding the Observation oJ Clients
Do have demonstration materials ready before beginning. "George, let's
see if we can interest Mary and Sue in pastel chalk drawing. 1'11 get the materials
out and begin drawing. Can you bring Mary and Sue to the table for a guided
observation?"
Do orient the dient to the teaching situation. "Fred, come into the kitchen
with me, please. Good. You came with me. Stand here (point). You're standing
here where you can see me mop the floor. See how I mop .... " Do make
sure the dient is attending. "Jill,. . . good, you're looking at me. Now, look
at the mop." Jill's eyes glance around the kitchen. The teacher waits and
looks at the mop (models). If Jill does not imitate, the teacher gently prompts
Jill's head in the direction ofthe mop and waits for Jill to glance at it. "Good,
Jill, you're looking at the mop."
Do talk about behavior. 'Tm opening the can." "He's stirring the soup."
"Harry's vacuuming the carpet."
Do label objects, events, and relationships. "This is an eggbeater." "This
is a community meeting." "You're holding the bowl, that's helping." "It's
lightning and thundering."
Do keep the language simple; don't complicate descriptions. "Look, Mary
is wearing her raincoat," rather than, "Look, Mary won't get cold and sick
because she is wearing her raincoat." "Watch George cutting vegetables. See
how he keeps his fingers out ofthe way," rather than, "Watch George. He's
so careful, he won't have to worry about cutting his fingers and having to
stop and put on bandages. "
Do keep descriptions short; don't try to describe too much. "Watch, Bob
throws the ball and Jerry catches it," rather than, "Watch how Jerry is standing
under the hoop. Now watch Bob. He's going up for a jump shot and sinks
the ball, and Jerry is right there to catch it."
M odeling Jor Clients
Do model successive steps of a complex performance. "First, you put
the hamburger in the taco shell, like this. Now you try it. You're putting the
hamburger in your taco shell. Then you put some cheese on the hamburger,
like this. Y ou do it. That's it, put the cheese a11 over. Then you put on some
lettuce, like this. That's right, its alright if you spill, one can't help it. Now
you put a little hot sauce on it like this. Good. Not too much. That's right.
Now, let's eat."
72 CHAPTER 5
00 maintain attention to the model. (Gestures, prompts, facial expres-
sions, pauses, and noveIty all help maintain attention.) "Watch me mop the
kitchen floor. Look how I move the mop back and forth, back and forth,
back and forth. Look how I get in the corners. Come over here, where you
can see. That's right, now you can see. See how I get in the corners."
00 use others as models; point out what other staff members and dients
are doing. George wants to involve Jack in preparing tacos. George says,
"Look at Jane and Bill; they are grating cheese." George points to Jane, a
staffmember, and Bill, a dient. "Fred and Bob are frying hamburger." Points
to Fred, a staff member, and Bob, a dient. "Brian is all alone, cutting lettuce."
Points to Brian, a dient. "Help Brian so we can eat sooner."
00 use slow, exaggerated movements. Don't model too fast.
"Y ou take the cucumber and place it on the cutting board, like this .
and you slice it like this." Jean cuts quarter-inch slices as she counts in a slow-
paced manner. "One, two, three. Now, you try it." As the dient takes the
handle of the knife, Jean gently guides the knife and says, "One, two-count
with me-three, four." The dient begins counting, "five, six, seven .... "
Jean and the dient continue slicing and counting in a slow-paced manner.
Reinjorcing Clients
00 describe the dient's behavior. "You're putting your coat on." "You're
vacuuming the rug." Oescribing the learner's behavior is attending, a basic
reinforcer for most people. For many individuals the reinforcing value is not
so much what one says, but that one attends. Basically, one is saying: "I see
you." "I see you doing .... "
Describing behavior also provides labels. "You're holding the bowl; that's
helping." "You gave Amber a piece of candy; that's sharing." "You let Aaron
take a turn; that's cooperating."
00 specifically describe the "value" of a dient's' behavior. Praise is more
than abstractjudgment: "very good," "very nice"; such praise quickly becomes
sterile. Praise can be natural and low-key. In the initial stages of learning,
describe what the dient is doing and its value: "You're doing a nice job
opening cans; that helps us get dinner ready." "Y ou 're holding the bowl; that
helps Mary make the salad." Mix such praise with a smile, a nod, a touch on
the arm. Later, when a dient is more skilled, you may be more abstract, "You
did that very weIl, Larry." "Oid you make that? That's beautiful!"
Do direct group attention to appropriate behavior. Get everyone together
to reinforce each other, e.g., a group cheer. Instruct dients to reinforce each
other and to notice each other: "Oid you all see what Jerry is doing?" 00
direct another person's attention to appropriate behavior of the dient. Call
over other staff members to see what the dient is doing; get some interplay
ST AFF TRAINING 73
going between staff: "George, co me and look at what Jerry is doing." George
says, "Jerry, you're cutting vegetables for the salad; good, you're watching for
your fingers; that's being careful."
00 attend to the client's performance by instructing the next appropriate
response. For example, you can reinforce opening a can by saying, "now
dump it in the bowl." Dumping ingredients in the bowl can be reinforced by
saying, "now stir it around." Stirring ingredients can be reinforced by saying,
"take out the spoon and put it down."
00 fade contrived outcomes or rewards to naturaloutcomes. Contrived
outcomes or rewards (e.g., tokens, check marks, bits offood, high concentra-
tions of praise) may be necessary to establish behavior, but the goal is to
maintain behavior by naturally occurring outcomes. It is often necessary to
point out these outcomes to clients. At dinner, for example, one might say,
"Isn't this fmit salad good? Jerry and Mike made it."
Contrived reinforcement can be faded into normally occurring daily
events as in the following example: Jose loves coffee, but dislikes to shower
and wash his hair. Ron takes coffee into the bathroom and allows Jose sips
for more and more appropriate behavior. "Coffee, coffee," Jose says and Ron
says, "Okay, as soon as you soap and rinse your armpits." Jose complies and
Ron gives hirn a sip of coffee. "Coffee, coffee," says Jose and Ron says, "Okay,
put some more shampoo on your hair and rinse it." Jose complies and Ron
gives hirn another sip of coffee. Eventually, after Jose showers and washes his
hair, he and Ron chat and have coffee together each morning at the kitchen
table with the other clients. In these chats, Ron calls Jose's attention to the
natural consequences of showering by asking hirn how he feels or commenting
on his appearance.
Recognizing Teaching Opportunities
It is important for new staff members to realize that rehabilitation is not
usually accomplished in formal training sessions. In formal training, therapists
establish new behavior through intense, often programmed applications of
teaching mechanisms: repeated demonstrations, verbal instructions, massed
practice, and corrective feedback. These techniques are designed to teach
learners to perform as quickly and efficiently as possible. Teaching the daily
routine, on the other hand, is more often informal, occurring incidentally
throughout the course of daily living.
Although this teaching is informal, it is based on the same principles as
formal teaching: getting attention, modeling, guiding observation, prompting,
instmcting, reinforcing, and supplying feedback. The difference is that these
teaching mechanisms are applied selectively according to naturally occurring
circumstances rather than a predetermined lesson plan. Over time, staff mem-
74 CHAPTER 5
bers develop the ability to recognize circumstances that call selectively for a
model, a prompt, a word of praise, a specific instruction, or a bit of quiet
attention. From this perspective, opportunities to teach are always available.
New staff members may bring to rehabilitation facilities several assump-
tions about teaching and leaming established, for the most part, by school
experiences. Trainers can help trainees understand unique aspects ofteaching
by emphasizing the following directions: (1) Teaching is not always formal
training. Incidental training, though subtle, is effective over time. (2) Teaching
is not always telling people what to do. (3) Teaching does not always involve
new behavior; it may consist of piecing together parts of old behavior or
simply arranging opportunities for practice. (4) Teaching is embedded in nor-
mal social interactions that do not necessarily look like instruction. (5) Leam-
ing and teaching can be fun for both teacher and student.
MANAGEMENT OF STAFF DEVELOPMENT
Staff members are managers of a rehabilitation environment. Managing
a rehabilitation environment that is comfortable, natural, and positive, as
well as effective for leaming, requires knowledge and skill. The quality ofthe
teaching program for clients is directly related to the staff's overall level of
knowledge and skills. As the staff develop their knowledge and skills, the
clients will progress in their own acquisition of knowledge and skills for ev-
eryday living.
One responsibility of supervisors is the continuation of staff development.
Staff development activities include (I) monitoring the status of knowledge
and skills of staff members, (2) assessing the strengths and training needs of
staff members, (3) designing a process for maintaining and generalizing
strengths, and (4) providing or arranging training for needs identified through
periodic observations.
Supervisors might approach the process of staff development as though
they were responsible for developing highly skilled, well-coordinated teaching
teams. From this perspective, supervision and training blend into a single
activity.
Assessment ojTraining Needs. To monitor staffknowledge and skills
within a facility, supervisors must make frequent, direct observations. Staff
training inventories can be designed to focus the supervisor's observations.
These inventories provide information that the supervisor can use to identify
strengths and training need of each staff member. By identifying strengths
and needs, supervisors can (I) provide feedback to staff regarding observed
strengths, (2) develop a resource list, which identifies individual staffstrengths
STAFF TRAINING
75
in the facilit y, (3) develop a list oftraining needs for each staffmember, and
(4) develop a tutorial, in which staffwith specifi c strengths are malched in a
tutorial process with stafl' who have specific needs. Staff training invenlorics
help supervisors design efTeclive Iraining experiences that are relevant 10 spe-
cific training ncedsofcach Slaffmember within Ihe rehabililation environment.
0/ Stoff E"alllotiom. Like any 1001. staff training inventories
can be abused. A common mistake is 10 use stafftraining invenlories tocritieize
slaff performance. For example. a supervisor observes a slaff membcr' s per-
formance with dients. using a stafftraining inventory as a guide. She observC$
that he does not reinforce dienlS adequately. She teils a slaff membcr this is
a skill he needs 10 improve before the nexi evaluation. She gees on to say
that ifhe improves by the next evaluation. she will rale his performance high
on this skili : if he shows no improvement, she wi ll rale his performance low.
Further observations by the supervisor indieate no improvement Repeated
warnings don't seem to help. Shc gives Ihe slaff member a low rating on Ihe
skill at his nexi employcc evaluation. He turns in his resignation.
StafHail to perform successfull y cilher bccause they havc not learned the
skills necessary for successful performance or because they are not motivated
to perform successfull y. Supervisors may not adequately dislinguish between
these two reasons for stafrpcrformance failures. I f staffmembers do not know
how 10 reinforce dienls appropriately, simpl y telling Ihem about thei r inad-
equacies won't help. Knowing when and how to reinforce is a ski lI : training
is needed. Telling people about thcir problems and evaluating their perfor-
mances are not. l thcmselves. effcctive training tcchniques.
Stafftraining inventorics actualt y eval uate the adequacy oflhe stafft rai n-
ing program. If the staff training program is effcctive. then staff will show
progress on the stafftrdining inventory over time. Ifslaff do nOI show progress.
the training program may need redesigning.
Training to Train. The goal of training 10 train is to invorve all slaff
memhcrs in the tUl orial process as trainers. In this process. slaff1earn to guide
observat ions. model. coach. and give feedback to their colleagues. When staff
have been taught to teach dients successfully. they should be able 10 gencralize
these teaching skills successfull y 10 work with thei r co-workers.
Generalization of leaching skills 10 tutorial interacti ons requi res ( I) the
authorilY 10 teach other slaff and (2) practice in tutorial interactions. In re
habilitation faci lities. the responsibiHty to train new staff belongs to al1 staf[
ResponsibililY for managing the staff training process. however. is held by
supervisors.
76 CHAPTER 5
Supervisors are responsible for calling meetings to plan training agendas
for new staff members. They generally lead these planning meetings to develop
a tutorial process (what is going to be taught, by whom, when, and where).
Supervisors discuss the process of staff training with staff tutors. They en-
courage tutors to practice guiding observation, modeling, coaching, and giving
feedback to each other and supervisors. Through this process, supervisors
check out training skills of tutors, give feedback, and make suggestions. Also,
supervisors arrange for tutors to practice with others: staff from other dients,
visitors, and family.
SUMMARY
Sta.fJ Training Procedures
1. Tutorial processes involve the trainee working alongside experienced
staff members subsequent to directly observing more experienced
staff members performing job functions. Here, new staff members
acquire essential skills from their peers.
2. Guided observations refer to orienting new staffto the environment,
situations, and roles before the trainee enters the environment.
3. Directing attention refers to having the trainer outline critical events
in the environment. This can indude dient behavior, staff responses,
interactions, and procedures in effect.
4. Modeling consists of demonstrating new behaviors to trainees.
Trainers must be competent in the behaviors they model.
5. Trainers do not allow trainees to engage in incorrect behaviors. The
trainer informs the trainee that he/she will redirect, step into situa-
tions, model, and guide trainees' observations of the appropriate
performance.
6. Three specific guidelines for providing feedback are as folIows: (a)
prepare the trainee for accepting feedback, (b) be specific regarding
what behavior was observed, and (c) be objective and understanding
in providing feedback.
The Daily Routine
7. Practicum training introduces new staff to routines of daily living in
a specific residence and enables them to participate, as soon as pos-
sible, in residential teaching, naturally and effectively.
8. Through tutorial experiences, new stafflearn to (a) participate in the
routines of daily living, (b) teach brain-injured individuals, and (c)
ST AFF TRAINING 77
recognize opportunities for teaching that arise naturally in the course
of residentialliving.
9. Tutors must not assume that new trainees bring with them a full
complement of skills. Even trainees experienced in everyday house-
hold maintenance may need guidance in the procedures of a partic-
ular residence.
Teaching Clients with Erain Injury
10. When teaching clients with brain injury, several strategies should be
involved: provide demonstrations and models ofthe appropriate be-
havior, keep instructions and language short, reinforce clients fre-
quently, direct the group to appropriate behavior, and fade contrived
rewards to natural outcomes.
11. It is important for new staff to realize that teaching is not usually
accomplished in formal training sessions. Rather, residential teaching
is more informal, occurring incidentally and appropriately through-
out the course ofthe day. This characteristic distinguishes residential
from schoolleaming environments.
Management 0/ Staff Development
12. The quality of the teaching program for clients is directly related to
staff's overall level of knowledge and skills. As staff develop their
knowledge and skills, clients will progress in their own acquisition
of knowledge and skills for everyday living.
13. Staff development activities include: (a) monitoring the status of
knowledge and skills of staff members, (b) assessing strengths and
training needs of staff members, (c) designing a process for main-
taining and generalizing strengths, and (d) providing or arranging
training for needs identified through periodic observations.
14. Assessment oftraining needs can be established both by conducting
direct observations of staff and by completing staff training inven-
tories.
15. Staff evaluations are frequently misused by using them to criticize
staff performance.
16. Training to train refers to involving staff in the tutorial process as
trainers. Here, staff leam to guide observations, model, coach, and
give feedback to their colleagues.
Procedures for
Cognitive Problems
6
Cognitive deflcits in survivors oftraumatic brain injury frequently have been
deflned as impairments to the intellectual functioning ofthe individual. Spe-
ciflc cognitive problems often cited in the literature include memory loss,
attention deflcits, impaired concentration, decreased perception, difficulty
processing information, planning and organization deflcits, sequencing dif-
flculties, and decreased orientation (Fisher, 1985; Voganthaler, 1987). The
impact that cognitive problems have on individuals with brain injury is best
outlined by Ben-Yishay and Diller (1983). They state that cognitive problems
are the primary reason why survivors ofbrain injury fail at independent living,
social competence, and vocational endeavors. Although survivors of brain
injury often show similar cognitive deflcits, treatment effectiveness must be
determined on an individual basis. This chapter presents several successful
strategies used in treating cognitive deflcits.
MEMORY LOSS
Memory loss is the most frequently reported sequela of cerebral trauma
(Levin, Benton, & Grossman, 1982). Not only are memory disorders pervasive,
but they are also complex and difficult to remediate. The deflcit may be a
problem with long- or short-term storage, may be modality or material speciflc,
otthe problem may be in encoding, storage, or retrieval ofinformation. Func-
tionally, memory deflcits frequently interfere with one's ability to complete
vocational tasks and independent living skills and leam new information.
Individuals with brain injury and their families are likely to experience dif-
flculty in procuring treatment because few professionals have experience with
79
80 CHAPTER 6
memory problems. Even suggestions as to how to help them deal with this
devastating problem and the resulting difficulties in their daily lives may be
inadequate.
Several questions remain unanswered regarding the remediation of
memory loss in dients with brain injury. First, which strategies work and for
which types of memory deficits do they work? Second, are dients able to
generalize the use of remediation techniques to their everyday lives after initial
training? Third, how weH do they comply with learning and practicing the
techniques? Strategies are presented in this chapter that have been evaluated
in improving memory functions. These strategies are divided into two cate-
gories: cognitive retraining and compensatory strategies.
Cognitive Retraining
Developed by Luria (1969), the theory of cognitive retraining refers to
using brain tissue in areas of the brain other than those injured so that this
uninjured tissue can perform the lost function. Cognitive retraining is based
on a model of changes in neuronal mechanisms, like the rerouting of neural
connections. Luria hypothesized that the dynamic reorganization ofthe ner-
vous system is promoted by specific therapy. For memory loss, this can be
accomplished through several methods induding, but not limited to, written
and verbal rehearsal, acronym formation, visual imagery, chunking, associ-
ation, and rhyme formation.
Written Rehearsal
Written rehearsal refers to repeatedly writing information that has to be
remembered. This is done by having the dient write information that needs
to be remembered several times. Information can be rewritten as many times
as needed to facilitate recaH. To remember a new piece ofinformation, so me
dients may need to write it out ten times whereas another dient may only
need to write it three times.
Written rehearsal is most effective when the dient can self-initiate the
strategy. The technique may be more effective if it is used to remember only
a few things versus everything required daily. For example, the dient may
choose to use written rehearsal to remember the names of individuals in his
or her support group, to remember how to stock shelves at a grocery store,
or when he or she is remembering directions to a frequently visited place.
Verbal Rehearsal
Verbal rehearsal requires the dient to say the information aloud or whis-
per it several times. For example, in remembering what to buy at a grocery
PROCEDURES FOR COGNITIVE PROBLEMS 81
store, the client may say out loud what has to be purchased. When using
verbal rehearsal, the client again needs to pinpoint exactly what is to be re-
membered and be able to self-initiate the technique. Ifthe client cannot pin-
point what needs to be remembered, then staff or family members will need
to prompt the client when to use the technique. Verbal rehearsal may be
easier to implement than written rehearsal because it does require time to
write responses on paper. Written rehearsal, however, results in a permanent
visual cue that can be used for later reference. As with written rehearsal,
verbal rehearsal may be effective when attempting to remember a few select
items versus an entire daily schedule. Figure 6.1 is a rehearsal training form
that can be used for both written and verbal rehearsal. This particular form
uses seven columns for training trials.
Zencius, Wesolowski, and Burke (l990a) compared the effectiveness of
verbal and written rehearsal. The dependent measure was the frequency of
memory assignments recalled correctly. Assignments required participants to
find two job leads from the classified ads ofthe newspaper and remember the
employer, job title, and qualifications needed. Results suggested that both
written and verbal rehearsal increased recall of information in the higher
functioning group, and no change was observed in the second group of clients.
Thus, the use of rehearsal may be a method of improving memory if the
individual can remember to use the strategy and if the person's memory is
not severely impaired.
Acronym Formation
Acronym formation refers to developing code words from key letters
(usually initials) of material that needs to be remembered. One letter can be
picked from each word to form a code word. For ex am pie, in remembering
the five Great Lakes, one could remember the word HOMES. The letters in
this word would stand for Huron, Ontario, Michigan, Erie, and Superior. As
with rehearsal, the client must be able to pinpoint what is to be remembered
and be able to use the technique when needed. It is unlikely a client could
form acronyms for everything that needs to be completed in an entire day.
Acronym formation may be effective in situations such as studying for an
examination, remembering players on a team, and remembering ingredients
of a recipe. As shown in Figures 6.2 and 6.3, acronym formation resulted in
some ofthe clients recalling more want ad information. Acronym formation
may be a useful memory strategy in cases where only small amounts of in-
formation need to be remembered.
An illustration us:ng acronym formation is provided by a 24-year-old
individual with brain injury who was trained to develop a code word to aid
in his meal preparation. The client impulsively would eat whatever was in
82 CHAPTER 6
RBHIARSAL TRAIIIIIIG FORM
Wrtte informatioD to be remembered below.
Use ODe liDe tor each trial wIleD ostDg writteD rehearsal
1
2
3
4
5
6
7
&
9
10
FIGURE 6.1. Rehearsal training form.
sight and would not prepare meals from all four food groups. Some of his
typical meals included a bag of chips, a portion of potatoes, and apound of
hamburger. He developed the code word BRA VE: BR = breads and grains,
A = dairy products, V = vegetables and fruits, and E = meats. Once a day,
he was required to prepare a meal using this code word.
Chunking
Chunking refers to grouping pieces of information together. Chunking
can be used when several numbers, names, or other pieces of information
PROCEDURES FOR COGNITIVE PROBLEMS 83
BSU< VERBAl. W!VT1e' NOTmOOK ACRONVII
ReEARSAI. FeEARSAL LOG
6
". ".
- - iii
5 UZ
ffi
i
4
3
>-
iil
2
....
<I
!5
0
0
0
<I
fil
6
5
/
4
/
/
MAX
0
3
V)
....
2
I
0
V)
V)
<I
6
\
>-
0:
-
0 5
:::E
4
DOLORES
:s 3
V)
I
2
0
0
2 3 4 5 6 7 8 9 10
TEST TRIALS
FIGURE 6.2. Results [rom group 1 show that all strategies were superior to baseline, but notebook
logging was the best treatment.
need to be remembered. For example, in remembering three frequently called
area codes, each one is chunked individually, e.g., 612, 618, and 603. As with
all ofthe above techniques, the dient must be able to identify wh at needs to
be remembered and when to use the memory strategy. Chunking techniques
are most useful in situations like remembering phone numbers, tools needed
for a job, components of daily menus, or a shopping list by breaking the items
into four food groups.
Visual I magery
The most commonly used and most thoroughly researched mnemonic
strategy is visual imagery. In visual imagery, the dient forms an image or
mental picture of the information to be remembered. Images can be formed
oftasks to be completed, people to remember, directions to places, and one's
84 CHAPTER 6
WAITTEN Yel9Al. ACRONYM >IOTiBOOK
RaEARSAl. RBEARSAL CODE .OC*: l OG
4
JIM
3
'. 2
----- -----
'-
0
6
-
5
4
3
NELLY
-----
'.
0
6
5
4
3
HENRY
'.
-----
-----
0
3 4 5 6 7 8 9 10
TEST TRIALS
F1GURE 6.3. Results from group 2 show that notebook logging was the only condition that
improved memory.
daily schedule. It may be easier to use visual imagery if the information is
important to that person or if the image is unusual or humorous. Because
visual imagery is time-consuming, it too should be used only when sm all
amounts of information need to be remembered. Glitsky and Schacter (1986)
suggested that research using visual imagery has yielded mixed results. Ad-
ditionally, there is no evidence that a person with impaired memory can use
visual imagery without instructions from others.
Association
Association refers to pairing a piece of information that a person wants
to remember with an old or familiar stimulus. This can range from anatomical
similarities of people to job similarities. Clients can remember new people
they meet by associating them with common stimuli of people they already
know. For example, a dient can remember a girl named Ginger by pairing
PROCEDURES FOR COGNITIVE PROBLEMS 85
Ginger with the girl on Gilligan's Island. A dient can remember new vocational
tasks by associating them with a similar pastjob, e.g., achambermaid performs
several of the same deaning tasks as a janitor such as sweeping, vacuuming,
and deaning sinks. Other illustrations of association indude remembering a
new recipe by associating with a recipe frequently used, and remembering
equipment for a leisure event by associating it with another leisure event often
engaged in. An additional consideration in using association is that the dient
must be able to remember to use the technique when needed.
Rhyme Formation
Rhyme formation consists of having the individual make a rhyme from
the information to be remembered. It can be used to remember names, places,
and things. For example, in remembering the names Marge, Paul, and Rank,
one could form the rhymes Large Marge, TaU Paul, and Rank the Tank.
With all ofthese memory strategies, several important considerations for
their use have been introduced. (1) Can the dient self-instruct him- or herself
to use these techlliques or initiate them when needed or does he or she rely
on others to prompt their use? In other words, can the dient remember to
use the memory strategy when performing certain tasks or to recall important
information? If not, the primary caregiver will need to establish a system to
prompt the dient to use the technique. Parents whose son is taking continuing
education dasses, for example, may need to establish a prompting system for
their son to use acronym formation when studying course material. (2) It
may not be practical to use these techniques for everything that needs to be
remembered on a daily basis. That is, forming acronyms or rehearsing every-
thing that needs to be remembered is time consuming. Thus, these techniques
have limited application. It is recommended that they be used in facilitating
recalling specific bits of information, e.g., identifying steps of a task, identifying
vocational tasks to be completed. In Zencius et al. (1990a), for example,
acronym formation and written rehearsal required approximately 1 hour of
work to recall six simple pieces of want ad information. (3) Even though
leaming may occur, does generalization to other tasks or situations occur?
Glitsky and Schacter (1986) question whether newly leamed memory tech-
niques generalize. To illustrate this, a dient at arehabilitation facility was
taught to use written rehearsal to recaU information needed for grocery shop-
ping. Although she regularly used the technique for remembering items on a
shopping list, she did not apply the strategy to other situations where she
frequently forgot information. These other situations induded information
covered in therapy sessions and at apart-time vocational training site. (4)
Can dients with severe memory deficits leam new skills from consequences?
Frequently, dients with severe memory deficits leam with such difficulty that
these strategies are not practical. Individuals with severe memory deficits fre-
86 CHAPTER 6
quently forget the names ofpeople they interact with daily, get lost in familiar
settings, and fail to leam through consequences. In cases of severe memory
deficits, compensatory strategies are recommended.
Compensatory Strategies
In contrast to memory retraining strategies, the use of memory aids is a
way of supplementing memory functions, usually by adding an extemal
memory source. The use of memory aids in the form of functional compen-
sation is based on a behavioral model (Heilman & Valenstein, 1979). The
time and effort necessary to retrain brain-injured clients' memory may be far
in excess of the benefits derived from the use of such strategies. It may be
simpler and more efficacious to teach the use of compensation strategies and
aids to expand the memory capacity to include an extemal store. Furthermore,
it is easy for the brain-injured client to understand why these strategies
will help.
In a review of the literature, Glitsky and Schacter (1988) concluded that
extemal memory aids were superior to both drills and mnemonic strategies.
Many neurologically intact individuals routinely make use of such strategies
in the form oflists, appointment books, and diaries. Harris ( 1980) points out
that even after memory training, many people prefer such memory aids. In
addition, the training necessary to implement memory aids is simple compared
with mnemonic strategies. Moreover, since the individual is taught to use
these methods in everyday situations, generalization to other situations may
be easier. In the long run, they become generic problem-solving strategies
that serve to increase memory capacity.
Compensatory strategies can be divided into three types: (I) storage de-
vices, such as written checklists, memory notebooks, calculators, and com-
puters; (2) cuing devices including alarm clocks and watches, beils, and timers;
and (3) restructured environments, such as labeled cupboards and drawers,
signs, and rearranging the environment so that the individual can remember
better.
Written Checklists
Written checklists have numerous applications. They can be used to
outline specific steps of a task, list vocational skills to complete, and list daily
duties. Checklists should contain three components to make them effective.
First, a column identifying the information needed to be remembered should
be written. In many cases, this includes steps of one task or a list of tasks. For
example, a checklist may be provided to the client that has all ofthe steps of
cleaning a refrigerator listed. Another checklist may be less specific and lists
PROCEDURES FOR COGNITIVE PROBLEMS 87
all ofthe tasks to be completed at the vocational training site during one day.
Second, blank columns paralleling the column with the information should
be induded. The dient can use these blank columns to check off each task
or step after completing it. Third, a memory checklist should indude a title
at the top and aspace for the date.
A brief training session should follow the presentation of the checklist.
The staff member presenting the checklist should model how to check off
items subsequent to completing a step or task. For example, if the checklist
contained all of the steps necessary to prepare a ten-step lunch, the trainer
would begin by completing the first item on the checklist and then checking
it off. This sequence would be continued until all steps are completed and
checked off. On the next trial, the trainer would allow the dient to prepare
the lunch using the checklist. The trainer would direct the dient to consult
the checklist if the dient made any errors during trials. It is important that
the dient always check off each step on the checklist before progressing to
the next step. Figure 6.4, entitled "Daily Chores Checklist," is an example of
tasks that need to be done daily. In this checklist, the times for completing
these tasks are provided. Figure 6.5 is more specific and lists all steps of dusting
a table. Appendix B contains sampie blank forms for entire tasks and daily
schedules.
The number of steps in any task should be individualized or tailored to
the dient. That is, some dients may need a task broken down into ten steps,
whereas others may only require five steps. The number of steps in a task is
determined by baseline data. A more specific checklist is needed if the fre-
quency of errors is high.
Checklists can be beneficial when performing any task that can be broken
down into measurable units. Checklists are particularly helpful when the brain-
injured individual continually forgets to complete certain tasks, makes frequent
errors, or skips specific steps oftasks. Another benefit ofusing memory check-
lists is that they can be systematically faded out. That is, the checklist can be
faded out by withdrawing one step of the checklist; e.g., after completing a
ten-step woodworking task correctly five times, the last step of the task is
removed. This procedure is continued until all steps of the checklist are
eliminated.
Memory checklists are useful tools and may facilitate skill acquisition.
Zencius, Wesolowski, Burke, and McQuade (1991) demonstrated that three
brain-injured individuals increased skill completion and accuracy when
memory checklists were used. The first dient increased completion of groom-
ing skills, and the second and third participants increased performance on
multistep woodworking tasks (Figures 6.6-6.8). Before introducing memory
checklists, all individuals made frequent errors and seldom completed the
tasks. This led staff to label them as noncompliant.
88
CHAPTER 6
DAll Y CHORES CHECKLIST
TIME TASK CHECK-OFF
8:30am make bed
9:00am Empty garbage
IO:OOem Clean counter tops
1 0:30am Feed goldfish
11:00am Cl een ashtreys
6:00pm Wesh dishes
6:30pm Sweep kitchen
6:45pm Water plants
Comme!lts
FIGURE 6.4. Daily chores checklist.
Memory Notebooks
Memory notebooks can be used to facilitate remembering daily schedules,
appointments, daily and weekly tasks, recording daily entries, new information
to be remembered, and new people met. Appendix B is a memory notebook
that contains specific forms and sheets including a daily schedule form, a
weekly schedule form, a monthly calendar, an individual goal sheet, a daily
journal form, an assignment sheet, a notebook entry form, a blank memory
checklist form, a self-medication checklist, and a "new people I've met" form.
We recommend that memory notebook training begin with identifying
the rationale or justification for the memory notebook. That is, what will the
PROCEDURES FOR COGNITIVE PROBLEMS 89
T ASK( S) TO BE COMPLETED_D_U_S_T_I N_G__T__B_L_E ______ _
STEPS TO BE COMPLETED TR I ALS-------);
1.) gether materials: soft rag & polish
2) Remave items from taDle top
I
3.) Shake furmture polish
4) Spray polish on entlre surfoce.
5.) Wi pe toDI e top from one si de to
U18 other side until complete
6.) Return Items to taDle top
7.) Return materials.
FIGURE 6.5. A memory checklist for dusting a table.
memory notebook be used for? Memory notebooks can be used for a variety
of purposes induding appointment making, daily schedules, phone numbers,
addresses, recipes, directions, people met, homework assignments, and "things
to do" lists. After explaining the rationale for the memory notebook, the
trainer should model how to use the notebook. For example, if the purpose
of the memory notebook is to facilitate remembering one's daily schedule,
the trainer would demonstrate how to write a daily schedule in thc notebook
and refer to it every hour. An additional component of using memory note-
book training is to indude booster sessions to review use of the memory
notcbook. This can be done on a frequent basis such as every hour or as
infrequently as weekly. The focus should be on providing feedback and praise
to the dient on the use of the notebook.
90
o
o
BAseu.E MEMORY ClECI<US T
FOUOW-uP
l - MONTH
.... :
......... 1 \ .... 11 .
.........................
JVl .......... II .
: 11
. 11
1 2 3 4 5 6 7 8 '9 10 11 12 13 14 15 16 17 18 '9 20 50
DAYS
CHAPTER 6
FIGURE 6.6. The level and frequency ofprompts required for a dient to complete four grooming
skills during baseline, using memory checklists, and follow-up. R = refused, P = physical prompt,
1 and 2 = first and second verbal instruction.
One consideration when using memory notebooks is whether the brain-
injured individual can remember to use the notebook. If not, a cuing mech-
anism must be established to prompt the individual to use the notebook. To
illustrate this, a 24-year-old at arehabilitation facility was given a memory
notebook to increase attendance to therapy sessions and recall daily homework
assignments. The memory notebook was initially ineffective because the dient
frequently forgot the notebook and left it in his room. A cuing procedure of
providing one verbal cue to the dient before he left his room each moming
was initiated. This increased memory notebook use to nearly 100%.
Memory notebooks are useful when large amounts of information need
to be accessible. Dougherty and Radomski (1987) outline six guidelines for
using notebooks: (1) Anticipation. Anticipation of the notebook adds to the
motivation to use it. The dient should be given the chance to retain infor-
PROCEDURES FOR COGNITIVE PROBLEMS 91
-,
"""",,"w,,- ...,..
..... c.e<>IlaT oeo<uIT .... ,
100
----
----
>
r
75
1lI
50
ffi
<
25
!
0
100
.-...-.
---
I
'"
75
1lI
50
'-
<
25
0
U
(/)
100
(/)
.-...-.
<t
I- ...
75
lIi
50
<
25
0
100
..
75
lIi
50
<
<t
25
!z
0
1 2 3 4 5 6 7 8 9 10 11 12
W
U
TRIALS
FIGURE 6.7. The percentage of three woodworking tasks completed independently during
baseline, using memory checklists, withdrawing the checklists, problem-solving, and follow-up.
The fourth task had no intervention.
mation before using the notebook. (2) Organization. A therapist should help
organize the notebook and teaeh the dient ways to organize it. (3) Routine.
A routine for its use should be established. (4) Relianee. Assignments should
be used as tools to faeilitate the dient's relianee on the memory notebook.
Onee routines are established, then outside assignments ean be introdueed.
(5) Comprehension. The dient must dearly understand notes taken, daily
sehedules, and all information reeorded in the notebook. (6) Rehearsal and
reinforeement. Continual supervision of the dient using the notebook must
oeeur followed by reinforeement for proper use of the notebook.
In spite of the widespread use of memory notebooks, there is little in the
rehabilitation literature doeumenting its effeetiveness. Zeneius, Wesolowski,
Krankowski, and Burke (1991) demonstrated that memory notebooks were
effeetive in inereasing appointments kept. The primary dependent measure
was the frequeney of homework assignments eompleted eorreedy. Every
homework assignment consisted of meeting a specific person at a certain time
and place and turning in a written assignment. Subsequent to baseline, par-
ticipants were given memory notebooks and a rationale for using them. The
teacher then modeled the use of the notebooks. Figure 6.9 reveals that the
completion ofhomework assignments increased only after introducing mem-
ory notebook training.
Visual Cues
Visual cues are written or graphie cu es that serve as reminders to engage
in certain responses. Typical visual cues include labels on cupboards to show
where certain utensils and foods are located, posting chores on the refrigerator
to aid in completing household tasks, posting daily menus to help clients
PROCEDURES FOR COGNITIVE PROBLEMS 93
BSLN MEMORY NOTEBOOK TRAINING
'Ji
0:
1
W
m
1
3
1
::I 1
Z
2
1
e
1
NEO
1
IJ) 1
1
I-
1
Z
W
0 1 _ _ ,
Z
3
1
CJ
1
in
1
IJ)
2
1
LlZ
1
1
1
0: 1
0
0
;:
W
1
3
1
0
J:
1
BOB
11..
2
1
0
1
IJ)
1
1
I-
1
Z
0
W
1
Z
-- I
0
11.
3
1
-v-::
1
0 2 1
0
1
1
1
0
1
2 3 4 5 6 7 6 9 10 11 12 13
FIGURE 6.9. The effects of memory notebook training on completing homework assignments.
prepare meals, and labeling dOOfS to show clients the location of rooms. Il-
lustrative ofthis, a visual cue was posted on a brain-injured individual's dOOf
to decrease entering other clients' apartments, which occurred daily. This
confusion was eliminated by putting his first name on the front door of his
apartment.
Visual cues also can be pictures or maps. Pictures are especially useful
for the nonreader. For example, pictures can be used to outline steps of a
vocational task, prepare lunch, or playagame. As with memory notebooks,
visual cues are widely used with clients in rehabilitation centers; however,
little research is available demonstrating their effectiveness. Zencius, Weso-
lowski, and Burke (1 990b) used a visual cue to decrease profanity in a brain-
injured survivOf with memory deficits. The client often became verbally abu-
sive to others in classroom settings. This behavior became so disruptive that
several classes had to be terminated because of verbal and physical confron-
tations. Treatment consisted of placing an 8! by lI-inch piece of paper in
94 CHAPTER 6
front of hirn in dass. Written on the paper was the word "Swearing" in bold
red ink. The paper was plaeed in front of hirn in all three dasses he attended,
i.e., soeial interaetions, speech therapy, and oeeupational therapy. Figure 6.10
shows that only when the visual eue was plaeed in front of hirn did profanity
deerease in the three dassroom settings.
In another study using visual eues, Zencius, Wesolowski, Burke, and
MeQuade (1989) demonstrated that two dients benefited from visual eues
where other behavioral teehniques failed. In one study, a man who took fre-
quent, unauthorized breaks was kept on task by plaeing a sign at eye level at
his work station. The sign listed break times. Before initiation of the visual
eue, the dient left the worksite one to ten times daily for as long as 80 minutes
eaeh time. This was redueed when the visual eue was introdueed. Figure 6.11
shows that when the sign was used, unauthorized breaks deereased.
In the seeond study, a female refused to attend therapy sessions. A written
invitation and a map to eaeh dass were given to her 5 minutes prior to the
session. The written invitation eontained the name of the therapy, the time,
and the instruetor. This procedure resulted in the dient attending nearly 100%
of all seheduled therapies. Figure 6.12 shows the results of the map and in-
vitation on the pereentage of therapy sessions attended.
BSLN
VISUAL CUE
FEEDBACK
1Il ,.
.
r -\IV
s:
f g ,
t= <1)0
z >-
10
U.
o .... :
I%: "
a.. 0,
u.
o III ,
I%: 1
>- 0
::i: !2 I.
.... ,
.
,
F
.. ,
!!s ,
g ;
........
.
........ ........ .
CLASS DAYS
FIGURE 6.10. The number ofprofanities occurring in three different settings during baseline,
using a visual cue, and using verbal feedback.
PROCEDURES FOR COGNITIVE PROBLEMS 95
BASEUNE VERBAL CONTRACT WRITIEN INSTRUCTIONS
10
9
>
8
<x:
C
ce
7
W
CL
CI)
6
<x:
5
W
ce
al 4
C
W
3
!:::!
ce
0 2
:r:
\
I-
30 t.lHJTES
<x:
z
0
I l' l 4 6 7 8 9 10
WORK DAYS
FIGURE 6.11. The effects of a verbal contract and written instructions to decrease unauthorized
breaks.
Environmental Restructuring
Restructuring the environment in such a way that prompts the client to
engage in certain responses is considered environmental restructuring. Physical
changes can be made in the environment or changes can be made in the
client's schedule. Examples of changing the environment include placing
medication by the bed to remember taking medication at bedtime, placing a
cane at the door to remember to use the cane any time the room is left, and
having all of the correct tools and materials located on a workbench to com-
plete a project. In an example using environmental restructuring to facilitate
memory, a 28-year-old brain-injured male working part-time in a wood-
working shop frequently forgot daily assignments. While performing a task,
he would forget what his assigned task was so that he had to leave his work-
station to get additional tools or materials. This was remediated by moving
his workstation to a small room in the back of the workshop and providing
an of the tools and materials required each day.
Examples of changing a client's schedule are scheduling a fun day of
preferred activities for a client with memory deficits and depression, scheduling
therapies in close proximity to each other, providing pictures or maps on a
client's daily schedule. Clients with severe memory deficits may not be able
96
o
Z
W
(/)
z 75 -
o
(i)
(/)
W
(/)
>-
D.. 50 -
IX:
W
J:
U.
o 25 _
W
o
I-
Z
w
()
ffi 0 -
D..
BSlN
CHAPTER 6
COHT
tNn' A noHS A MAP OAl" Y SCtEDU..E
MQtEy DAL V SQH)lL[
.....
;
,
i j i ii j i i I i f I i I i i j , i I f i j
THERAPY DA YS
F1GURE 6. J 2. The effects of using a map and written invitations as compared with baseline,
contingent money, and a daily schedule to increase attendance to therapy sessions.
to provide themselves with environmental cues (e.g., set out medication), thus
a staff or family member will have to perform this. Although these techniques
may be useful in familiar environments, e.g., in a daily workshop, kitchen,
or bedroom, they may not be as useful in an unfamiliar environment.
ORIENTATION
Individuals with brain injury often demonstrate orientation deficits, that
is, confusion and disorientation to person, place, and time. Corrigan, Arnett,
Houch, and Jackson (1985) state that these characteristics are usually observed
during periods of amnesia following coma. Some c1ients, however, may ex-
perience some confusion and disorientation for years following brain injury.
Orientation Groups
Daily orientation groups are frequently conducted in TBI rehabilitation
centers. They are often directed by an occupational or speech therapist and
PROCEDURES FOR COGNITIVE PROBLEMS 97
occur as the first session of the day. The focus is usually on a review of daily
schedules, goals, the current time, day, date, and special appointments that
week. To illustrate, an orientation group may begin with the therapist re-
questing that all participants write down the current day and date, their in-
dividual schedules for the day, and one current event. Next, the therapist asks
for volunteers to share their responses and provides corrective feedback. We
recommend tailoring the orientation process to each dient in the group. For
example, the individual who is often disoriented as to location would receive
extra attention on current location, address of residence, phone number, and
a contact person. If the dient is often confused about other people, then
orientation would focus on members ofthe group, staffmembers, roommates,
and roles of these people. Corrigan et al. (1985) developed an orientation
package at arehabilitation facility. The group package was initiated to improve
attentional deficits, confusion, and disorientation. Daily 30-minute sessions
induded specific information regarding time and day, location of environ-
ments at the facility, orientation to other group members, and orientation to
general facts such as current events, geography, and personal facts. Three case
studies showed that the orientation package was effective in increasing weekly
performance of assignments relating to orientation.
Individual Orientation Sessions
Orientation provided on a one-to-one basis is preferred when severe dis-
orientation is observed. The main advantage is that more material can be
continually reviewed and corrective feedback can be provided immediately.
The material also can be individualized. The disadvantage of the individual
session is that the dient misses the opportunity to interact with a group.
Individualized orientation begins with the therapist asking the dient an ori-
entation question (e.g., "What is my name?"). The dient is given 3 seconds
to respond. Ifthe correct response is given, the therapist provides verbal praise
(e.g., "That's correct, my name is Willie"), and moves to the next orientation
question. Ifthere is no response or an incorrect response is given, the therapist
provides a verbal cue, e.g., "My name begins with the letter W." Again, the
therapist pauses for 3 seconds. If no response is given or an incorrect response
is made, the therapist provides the dient with the correct response (e.g., "My
name is Willie"). Finally, the therapist asks the dient to repeat the correct
response. When he or she does, verbal praise is provided.
This sequence is continued until the dient answers each question cor-
rectly. The number of times orientation questions are reviewed in a session
should be determined in advance. For example, orientation questions can be
reviewed three times (a set number). An alternative strategy is to review ques-
tions until a criterion is met, e.g., all questions are reviewed until they are
98 CHAPTER 6
answered correctly on two consecutive trials. Figure 6.13 shows examples of
17 routine orientation questions that can be used in individual or group train-
ing. A column is provided to score responses on all trials.
Orientation questions mayaiso be presented in a written format. Written
questions can be used alone or in conjunction with verbal instructions. If
used in conjunction with verbal instructions, the therapist should present the
DBtes: _______ _
Routine questlons
1.) What i8 the name
of th18 place ?
2.) What cl ty are we
in now?
3.) What stete are we
in now?
4.) What day 18 th18 ?
5.) What 18 the date?
6.) What time is it
now?
7.) Name other people
in this group
8.) What Is the
temperature now
9.) Name one current
event
10.) What time
does thi 8 group beg! n ?
1 1.) What 1 s on the
schedule for tOdey ?
12.) Name any hol1deY8
th! s weelc or month.
13.) Who is the current
Presldent of the U.S. ?
14.) Any special
ennouncements ?
15.)Whllt Is the U.S.
capital ?
16.)Whet is the
address here ?
17.) What 1 s the phone
number here ?
FlGURE 6.13. Examples ofroutine orientation Questions.
PROCEDURES FOR COGNITIVE PROBLEMS 99
written part (orientation question) simultaneously with asking the question.
If presenting written orientation questions alone, it is recommended to provide
only one question at a time. For example, one question would be written on
a separate piece of paper, index card, or flash card.
ATTENTIONAL DEFICITS
Lezak (1983) points out that deficits in attention and concentration are
one ofthe most commonly observed in brain-injured persons. Attention def-
icits are often defined and measured in terms of an individual's ability to
attend to a stimulus, task, or situation. Posner and Rafal (1987) further define
attention to include three components: alertness, vigilancejcapacity, and se-
lection. Alertness is the readiness of an individual to respond to information.
Vigilance or capacity refers to the degree of mental effort invested in an act.
The amount of information we can pay attention to at any given time is quite
limited (Posner & Rafal, 1987). The final component, selection, refers to the
allocation of attention to a specific and limited amount of information.
Guare, Dawson, and Warren (1988) stressed the importance oftreating
attention deficits in rehabilitation settings since the first step of learning in-
volves attending to a stimulus and encoding information. Before introducing
specific techniques for dealing with attentional deficits, assessment of atten-
tional deficits will be discussed.
Guare, Dawson, and Warren (1988) outlined two assessment approaches
including situational observations of a specific task and observing behaviors
throughout the day. With situational assessments, a specific task is targeted,
and the client is observed in trials performing the task. Examples could include
attending to a lecture, attending to a videotape session, working on projects
in a woodshop, or completing math problems in a classroom. The second
assessment technique involves observing the client in his or her daily routine
(i.e., performing vocational, leisure, domestic, or educational tasks). The sec-
ond technique is divided into three specific steps that must be performed to
complete the assessment. First, the behavior being assessed must be identified
and defined precisely. The behavior is defined so precisely that it is scored
similarly by everyone observing the behavior. Second, the behavior must be
measured. Measurement includes establishing a baseline. The baseline is used
to measure the effects oftreatment. Third, a functional analysis ofthe behavior
is conducted. That is, the behavior is studied as to its interaction with the
environment. Antecedents and consequences ofthe behavior are studied. An-
tecedents include anything in the environment that precedes the behavior
and can include other individuals, room size, pictures in the room, time of
100
CHAPTER 6
day, and tone of voice. Consequences are anything that follow the target
behavior and can include praise, feedback, and reprimands.
In addition to observing behaviors, several scales have been used to assess
attentional deficits. Widely used in acute care settings is the Glasgow Coma
Scale (Teasedale & Jennett, 1974). This scale measures various motor re-
sponses, verbal responses, and provides a rating oflevel of coma. The Glasgow
Coma Scale also measures alertness and arousal. The Rancho Los Amigos
Levels Cognitive Recovery Scale (Malkmus, Booth, & Kodimer, 1980) outlines
severallevels of recovery from cognitive deficits. This scale provides indirect
measures of attention. The Galveston Orientation and Amnesia Test (GOAT)
measures orientation and alertness (Mack, 1986).
Attentional Training Strategies
Several training strategies are listed in the literature as being effective.
Little empirical data, however, exist on their proposed effectiveness.
Environmental Restructuring
Environmental restructuring refers to physically changing the environ-
ment by increasing, decreasing, or eliminating stimuli in the environment.
This can be done to both decrease maladaptive behaviors and facilitate skilI
acquisition. Changing the environment may be necessary when working with
clients who become distracted easily and is an especially useful technique
when the existing environments are highly stimulating, Le., noisy, bright, or
densely populated. Actual changes in the environment that can occur include,
but are not limited to, using less distracting colors, designs, and styles of
artwork, reducing the noise level in a room by using individual study carrels
versus tables, limiting the number of people in the room, and the use of
indirect lighting. For example, a client working in a classroom is continuously
distracted by other students, sounds, and noises. In this example, the teacher
may place the c1ient into a study carrel when doing homework assignments.
Illustrative of this, a 44-year-old brain-injured individual participating in a
vocational training program became easily distracted, wh ich resulted in a lack
of production. Within the environment were several distracting stimuli in-
cluding ten other c1ients, three vocational trainers, power tools, and direct
lighting. His attention increased when a study carrel was provided to hirn in
the storage area of the workshop.
Salience ofTarget Stimuli
Guare et al. ( 1988) emphasized the importance of increasing the salience
of a stimulus in certain conditions. So me of these conditions arise when it is
PROCEDURES FOR COGNITIVE PROBLEMS
101
not possible to change the environment. Salience of a stimulus can be changed
by altering its color, size, shape, location, or dimension. For example, a dient
may not attend to certain steps on his or her daily checklist. The salience of
the stimulus could be changed by placing these steps on a checklist in a different
sequential order, changing their size, or highlighting them. One benefit of
changing the salience of a stimulus is convenience. It may be easier to change
one stimulus than rearranging parts of or the entire environment. Figure 6.14
shows an example of changing the salience of a stimulus by enlarging the size
of the last step of a vocational checklist.
VOCATIONAl TASK: CUTTING & PlANING lUMBER
STEPS OF THE T ASK TRIALS-----------
1.) Select 10 boards from lumber pile.
2.) Cut eech board to 36".
3.) Bring boards to planer.
4.) Plene all boards to 7/8" thickness.
5) Put completed boards on storage rack.
6) Turn off power & clean plener.
1. 1llIIITI!lIIllIOO 'ii'1!ll 'ii'1!ll1!ll1!. 1llI1!ll1!ll1l'll.
HGURE 6.14. Changing the salience of a stimulus by enlarging the size of the last step of a
vocational checklist.
102 CHAPTER 6
Checklists
Checklists are useful in situations where the elient must perform multiple
steps of a task or several tasks throughout the day. When using checklists, it
is important that the checklist be in elose proximity to the elient. As discussed
in the memory section of this chapter, the specificity of the checklist is im-
portant. A checklist could be used to perform grooming skills in the moming
or to list all of the vocational tasks for the day, or a checklist could be more
specific and list the steps to complete one task. An advantage ofusing checklists
is that they are easy to implement and do not involve much preparation by
family members and staff.
Self M onitoring
Self-monitoring refers to the elient observing his or her own behavior.
Frequently, when individuals observe their own behavior, a change in that
behavior occurs. In its simplest form, elients can be trained to score an "X"
on a data sheet ifthey are attending to their vocational task when a particular
cue is presented. Figure 6.15 is a self-monitoring form used to measure at-
tending behavior every 15 minutes.
Self-monitoring also can inelude the use oftape-recorded messages, tim-
ers, or bells. For example, a beep on a tape-recorded message cues the elient
to record "yes" or "no" to his or her attending behavior. One consideration
in using self-monitoring is that elients may have the tendency to score those
behaviors that look most favorable. One strategy for dealing with this is to
have the primary caregiver collect the same data on a few observations to
determine their accuracy. Thus, the reliability or objectivity of the elient's
observations can be established. In an illustration ofthis, a 26-year-old male
was required to monitor and record attendance to task at a culinary arts
program every 30 minutes. The elient always recorded his responses as on-
task; however, when a second individual observed the elient's on-task behavior,
a large discrepancy was noted. This disparity was reduced by having the vo-
cational supervisor model what was on- and off-task behavior every day. The
vocational trainer also added feedback to these daily sessions. In addition to
self-monitoring vocational behaviors, elients can be taught to self-monitor
social behaviors, academic performance (number of math, social studies, or
language problems completed), or leisure and recreational activities attended
per week.
SelfTalk
Similar to self-monitoring, self-talk involves elients monitoring their be-
havior and talking to themselves abaut it. Meichenbaum and Goodman (1971)
PROCEDURES FOR COGNITIVE PROBLEMS 103
SElF-MONITORING CHECKLIST
TIME TASK ASSIGNMENT YES NO OBSERVER CHECKS
9:00am
9:15am
9:30am
9:45am
10:00am
IO:15am
10:30am
1 0:45am
11:00am
11:15am
11:30am
comments
FlCURE 6.15. A self-monitoring checklist.
describe se1f-ta1k as teaching peop1e to talk to themse1ves. Camp and Bash
(1981) developed the "Think A10ud" procedure. C1ients are taught to ask
themse1ves questions. Four specific questions they ask are "What is my prob-
lem?," "How can I do it?," "Am I using my plan?," and "How did I do?"
Self-talk may be effective when teaching dients to attend to routines or
specific tasks throughout their day. For example, it could be used with a dient
working in a woodshop setting where he has 15 routine tasks to complete
each day. Self-talk also may be beneficial when used in conjunction with self-
monitoring. The dient could use self-talk while simultaneously recording re-
sponses of the target behavior.
104 CHAPTER 6
Overlearning
Guare et al. (1988) state that if the dient has demonstrated some learning
capacity, then overlearning may be tried. With overlearning, multiple learning
trials of the target behavior occur. In other words, the same task is repeated
several tim es, rather than completing one task and then beginning a new one.
As with rehearsal techniques, the number of training trials is individualized.
That is, one dient may need to repeat the task as many as 10-15 times daily,
whereas other dients may need to repeat the task 2-3 times per day. Over-
learning may be most successful with behaviors that occur on a frequent basis
(e.g., sanding blocks, putting sewing kits together, filling dessert cups with
fruit, doing dishes). Illustrative of overlearning, a dient receiving outpatient
services frequently completed vocational tasks improperly. This was corrected
by having hirn only perform two tasks a day.
Altering Consequences
Providing more reinforcement for on-task behavior and reprimands for
off-task behavior may influence attending skills. When altering consequences,
one must be sure that the reinforcing stimulus presented following the target
behavior is indeed reinforcing, that is, the frequency of on-task behavior in-
creases. On the other hand, the stimulus presented after off-task behavior
must result in a decrease in that behavior. For example, a 12-year-old brain-
injured male was provided extra break times and social praise in the dassroom
for being on-task. Initially, the student would get up from his chair and walk
around the room or leave the dassroom. The teacher was trained to provide
social praise intermittently to the student for sitting in his chair and doing
work. The student also was given a lO-minute break each hOUT if he didn't
leave the room. This resulted in an increase in the number of dassroom
completed assignments.
Feedback
Used in either written or verbal form, feedback lets the dient know how
he or she is responding. It is easy to use when the dient is working on per-
manent products (i.e., the number ofproducts can be counted). To illustrate,
"Frank, you completed 25 math problems this hour," or "Sally, you completed
15 woodblocks this past 30 minutes." Feedback regarding attention to task
should indude three components. First, the trainer should make contact with
the dient in a positive fashion (e.g., handshake, pat on the back, smile). Second,
positive feedback should be provided (e.g., "You did a good job reporting to
school today" or "Last hour you completed five wooden jigs, that's great!").
PROCEDURES FOR COGNITIVE PROBLEMS 105
Finally, the dient should be given information about how their performance
compares with previous behaviors or short-term goals. For example, "Bill,
although you completed 10 math problems, your goal is to complete 15. Let's
try again next period." Figure 6.16 is a blank copy of a feedback sheet that
provides information on attention or on-task behaviors. The behavior or task
is first identified, and then information on dients' current performance and
their goal is provided.
Cuing Devices
Cuing devices are any mechanisms that prompt a behavior to occur and
indude alarm docks, watches, timers, and beUs. The cuing device serves as
an antecedent stimulus to engage in a certain response. For example, a beeper
on a wristwatch is an antecedent cue for the dient to take his or her medication,
or a beep played on headphones is an antecedent cue for attending to task in
a dassroom or vocational training site. Before using cuing devices to serve as
reminders to remain on task, an association between the cuing device and
the on-task behavior must be established. This can be established through
training trials. That is, the dient is first informed of the function of the cuing
device (i.e., to help them remain on task). Once the rationale is provided, the
dient should be given frequent opportunities to use the cuing device. Initially,
the dient should be provided frequent reinforcement for using the device. It
is also important that the dient experience positive results of using the cuing
device. That is, the dient should see the success he or she has made or the
benefits of using a device (e.g., more work is completed or more money is
made). Illustrative of using cuing devices to increase on-task behavior, a 22-
year-old brain-injured male participated in apart-time horticulture program
planting seedlings. It was noted that he only planted 10-20 seedlings every
ho ur. Because the dient remained at one workstation at the vocational training
site, a dock was placed directly in front of hirn. The dock would dick every
minute when the second hand reached the 12. This procedure increased the
number of seedlings planted every hour.
SELF-A WARENESS
Impaired self-awareness is often cited in the literature as a pervasive and
serious deficit. Several specific strategies have been offered to change "poor"
self-awareness; however, data on their effectiveness have not been reported.
Prigatano et al. (1986) defined denial of deficits as the process of an individual's
need to lessen the reality of cognitive, perceptual, and motor deficits. Guth,
Wesolowski, and Burke (1988b) noted that other authors have viewed denial
106 CHAPTER 6
as having a physiological basis. When denial is neurologically based, we call
it anosognosia. Methods of assessing denial and strategies often used in treating
it will be addressed.
Assessing SelfAwareness
Casual Observation
Probably the most frequently used method of assessing self-awareness is
casual observations made by direct care staff, dinical staff members, friends,
and family members. Observations of dients' skills by staff, family, and friends
often differ greatly from what dients believe they can do. For example, a
family member and a friend may believe that the individual will never drive
again, but the dient may believe he will drive once he can walk again. Some
frequently reported observations of denial occur in the areas of walking, em-
ployment, driving, and relationships.
Competency Rating Scale
Prigatano et al. (1986) used the Competency Rating Scale as a self-report
measure where dients evaluate themselves on various items (e.g., grooming
skiIls, domestic skiIls, time management, memory, social skiIls, emotions,
and other behaviors). Clients are given the questionnaire and asked to check
how they would respond to 30 items. Clients are to score from "Can't do" to
"Can do with ease" on a Likert-type rating scale. To determine a score, the
scale is given to a staff person who knows the dient weIl and to the dient.
When the staff member and dient finish the rating scale, the scales are com-
pared. The greater the disparity in scores between staff and dient, the greater
is the degree of denial.
Treating Denial
TBI Education
In TBI education, dients are taught about head injury. Clients should
be introduced to demographics about TBI; anatomy and physiology of the
brain; residual effects following TBI induding cognitive, physiological, and
executive sequelae; and facts about recovery.
The purpose of TBI education is to increase dients' awareness of TBI.
Guth et al. (1988b) outlined seven goals of a TBI education group. These are
to increase understanding of (1) brain function, (2) ways the brain can be
damaged, (3) how the brain recovers, (4) disabilities that can follow brain
PROCEDURES FOR COGNITIVE PROBLEMS 107
injury, (5) various treatment modalities, (6) personal brain injury, and (7) the
treatment plan.
The specific training methodology for teaching TBI education should
indude four aspects. First, training should occur in sm all groups (i.e., four to
five dients). In small groups, dients can share experiences oftheir individual
head injury and deficits. Also, group therapy offers an alternative instructional
method when one-to-one therapy is not feasible and results in more dient
contact. Second, characteristics of personalized instructional methods can be
used. Personalized system of instruction allows dients to proceed at their own
pace through instructional units with help from study guides. Also, the per-
sonalized system ofinstruction has a unit perfection requirement [i.e., before
dients can move to the next unit, they must master the preceding unit, dem-
onstrated by a mastery quiz (Keller, 1968)]. Third, interspersal training can
be used. That is, previously learned material should be reintroduced with new
course material (e.g., while learning new material on brain function, course
material on demographics would be reintroduced). Maintenance of skills and
information has been demonstrated by using interspersal training (Neef, Iwata,
& Page, 1978). Interspersal training is recommended for this population be-
cause ofthe memory deficits exhibited by the majority ofbrain-injured persons.
Finally, all course material should be divided into instructional units. Appendix
C outlines a specific training methodology for TBI education and an example
of pre- and posttesting procedures.
Personal Adjustmenl Groups
The aim of personal adjustment groups is to increase self-awareness of
one's abilities and limitations. This is accomplished by repeated feedback and
support via small groups. Ideally, personal adjustment groups are conducted
with two to six dients and one or two group facilitators.
Guth cl al. (I 988b) outlined three goals ofpersonal adjustment groups.
First, the facilitator should attempt to educate participants about the residual
effects of TBI (e.g., cognitive and physiological effects). This should be ac-
complished by using real-life situations. Second, emphasis should be placed
on recognizing individual strengths and weaknesses. Third, the group should
provide emotional support that will facilitatc the individual's participation in
the rehabilitation process.
The actual process of the personal adjustment group is further outlined
by Guth el al. (l988b). Thc groups should begin with a review of the goals
and rules of the group. Second, a group activity involving all participants
should be introduced. Next, the facilitator introduces the topic for the session.
The topics should reflect real-life situations of the group members (e.g., a
problem a dient experienced, share an experience a dient observed). Partic-
108 CHAPTER 6
ipants should then role-play situations that relate to their experiences. For
example, a participant in the group who has difficulty initiating conversations
with members of the opposite sex may role-play these situations. The group
is ended by the facilitator assigning homework assignments to all participants.
Again, the homework assignments should pertain to real-life situations (e.g.,
the client who has difficulty initiating conversations with members of the
opposite sex may be assigned initiating a certain number of conversations).
Team Integration
Team integration refers to encouraging the client to participate in his or
her individualized rehabilitation program. This can be accomplished through
three strategies: providing individualized rehabilitation programs, having
clients help select their rehabilitation goals and strategies, and involving clients
in staff meetings. Clients should receive treatment based on individual as-
sessment data rather than being included in traditional ongoing therapies
(e.g., group occupational therapy, a facility vocational training program, a
morning orientation group).
The client also should be encouraged to express individual needs (e.g.,
clients should be part of decisions in determining vocational training place-
ment). Clients should help develop treatment goals versus being provided
rehabilitation goals by therapists. Granted, individuals with limited self-
awareness should not be allowed to write all of their treatment goals, but
rather decide with the team the goals that are realistic.
Clients also should be encouraged to select treatment methods to over-
come their barriers. For example, the client who has anger problems should
help decide on the treatment of choice with the behavior analyst. Finally,
dients should attend the staff meetings regarding themselves. At these meet-
ings, the dient would receive feedback from team members about progress
made, changes in treatment, and criteria for discharge. Frequently, it is not
possible for the dient to attend an entire staffing meeting because of low
tolerance levels and denial. In these cases, Guth et al. (1988b) suggest abbre-
viated staff meetings. Here, dients are provided with an overview of the staffing.
It is recommended this occur in comfortable surroundings with a trusted and
preferred staff member.
Goal and Journal Group
Goal and journal review groups provide a forum for dients to identify
specific goals, monitor progress on identified goals, and receive feedback from
peers and a group facilitator. Generally, a goal and journal review group will
begin by having all participants identify both short- and long-term goals.
PROCEDURES FOR COGNITIVE PROBLEMS 109
Short-term goals are those that can be met within a week; long-term goals
take longer than a week to attain. Examples of short-term goals are to attend
a support group meeting, to use a quad cane 5 minutes longer than the previous
week, to prepare one's lunch. Some long-term goals are to obtain part-time
employment, to move to a group horne, and to walk without a cane.
After goals are identified and written down, they are reviewed at least
two times per week in the group. Additionally, dients are to write down
specifically what they have done to meet their goals. Clients often set goals
but do not initiate behaviors toward attaining them. For example, a dient
who wants to obtain employment but does nothing to prepare for employment
can be given this feedback. The third component of goal and journal review
is requiring that dients share their goals with peers. Feedback on how to meet
goals is provided. To illustrate, if one dient sets a goal to increase his or her
walking distance, others can provide feedback on how he or she can meet
that goal. This is also the area in which the therapist must address unrealistic
goals. Unrealistic goals must be addressed in a nonthreatening and supportive
fashion. The trained goal and journal facilitator does not argue or reject goals,
but rather points out the dient's strengths and weaknesses.
Natural Consequences
Natural consequences are those events following behavior that occur in
the natural environment. Frequently in rehabilitation centers, dients are pro-
tected from natural consequences. Illustrative of this, a 24-year-old male at
arehabilitation facility touched and kissed women without their permission
when he visited the community. When accompanying staff apologized, the
usual response was "That's OK." In this case, natural consequences were not
applied because the dient was viewed as being different. Using natural con-
sequences can be effective for those individuals who have unrealistic goals
and are unwilling to pursue professional recommendations. For example, a
dient at arehabilitation facility desires to seek employment in a position she
held prior to her injury. Using natural consequences, the dient would be
provided support if she were unsuccessful. After several unsuccessful en-
counters, the dient may become aware of her unrealistic employment expec-
tations. She then should be counseled about occupations for which she would
be qualified.
Video Therapy
Video therapy often can be used to increase self-awareness by allowing
clients to observe themselves in a variety of situations. For example, a dient
who believes he always uses good social skills could be videotaped in aseries
110 CHAPTER 6
of situations requiring the use of certain social skins. The tape can be repeatedly
played back to the client while giving him corrective feedback.
Illustrative of using videotape therapy, a 42 year old woman at a reha-
bilitation center engaged in continuous conversation, interrupted others, and
did not respond to social cues to stop talking. Treatment consisted of video-
taping her in various social situations in different environments. She viewed
the videotapes twice a week. After several weeks of watching herself on TV,
she began identifying the problem behaviors and took steps to correct them
with the help of therapists.
PROBLEM-SOLVING DEFICITS
Survivors of traumatic brain injury often are viewed as poor decision
makers and problem solvers. That is, rather than pinpointing problems, they
respond impulsively about possible solutions or consequences oftheir behav-
ior. On the other hand, they may demonstrate a lack ofresponding (i.e., they
do not self-initiate problem-solving). To define problem-solving, Szekeres,
Yilvisaker, and Cohen (1987) outlined several components involved in the
problem-solving process. These include identification ofthe problem, gathering
and considering information about the problem, exploring possible solutions,
formulating a plan, executing a plan, and monitoring the plan for its effec-
tiveness. Szekeres et al. (1987) outlined three important reasons for teaching
problem-solving skins: (1) Because ofthe brain injury, the patient's previously
automatic reasoning and decision making may no longer be serviceable, (2)
the change in the client'senvironment and activities also may require more
deliberate decision making, and (3) the number and significance of the new
problems caused by the injury require greater thoughtfulness than was nec-
essary before the accident or injury.
Functionally, the lack ofproblem-solving skins can interfere with one's
ability to cope with routine problems in vocational and educational settings,
independent living situations, and interpersonal relationships. In this section,
several strategies that have been used to treat problem-solving deficits will be
discussed.
Problem-Solving Groups
Traditionally, problem-solving groups are facilitated by a trained therapist
(i.e., a speech or behavior therapist) and occur in small group settings, i.e.,
four to six clients. The group facilitator presents problems to the group and
leads them through the problem-solving process. Problematic situations that
resemble real-life situations for survivors ofhead trauma are introduced. The
PROCEDURES FOR COGNITIVE PROBLEMS 111
trainer begins the session by providing a problematic situation to the group.
Problematic situations should be presented that closely resemble those ofthe
participants (i.e., situations that are encountered often by traumatically brain-
injured individuals). After allowing participants to generate solutions to the
problem, the trainer provides feedback to these solutions and walks them
through the three crucial steps in solving a problem, that is, accurately pin-
pointing the problem, developing solutions, and selecting a solution with regard
to advantages and disadvantages of each solution. For example, in dealing
with the hypothetical problem of an untidy roommate, one participant re-
sponds by stating he would have his roommate kicked out of the apartment.
The facilitator would first outline the consequences ofthis solution, i.e., "you
would be responsible for the entire rent payment or you would have to find
a new roommate." Next, all solutions to the problematic situation would be
examined considering advantages and disadvantages, and the best solution
would be selected.
In arecent study, Foxx, Marchand-Martella, Martella, Braunling-
McMorrow, and McMorrow (1988) trained six brain-injured individuals in
problem-s01ving skills in four areas: community awareness and transportation;
medication, alcohol, and drugs; stating one's rights; and emergencies. Training
occurred in a small group setting where participants responded to a variety
of problematic situations that were printed on index cards. Participants also
were provided with a cue card that listed all of the components necessary to
solve problems correctly. An additional component oftraining included a $2
bonus for responding to a predeterrnined number of problem-solving situations
correctly. Results of this study suggest that this training procedure greatly
increased the number of problem-solving situations answered correctly.
Problem-Solving Vignettes
Staged problematic situations that closely resemble problems of members
of the group are videotaped and participants observe and identify solutions
to these situations. As with problem-solving groups, training occurs in a small
group setting and is facilitated by a trained therapist. Problematic situations
for a wide variety of problem areas are videotaped including problems at a
workplace, problems with a roommate, problems in community situations,
and problems with interpersonal relationships. It is recommended that prob-
lematic situations be derived from situations that participants of the group
often encounter. Training begins by having participants view the videotape
of aseries of problematic situations. One vignette is shown at a time and
participants are asked to pinpoint the problem and develop solutions. For
example, one vignette may show an individual who has inadvertently taken
a double dose ofTegretol. Participants would generate solutions to this problem
112 CHAPTER 6
(e.g., call the 911 emergency number, call a friend for help, call your family
doctor). After revealing all possible solutions, each is considered as to advan-
tages and disadvantages. For example, although several solutions may be
available, some may be more practical to implement than others. When asking
participants to solve problems, it is important not to provide names of persons
who often display these behaviors. Rather, the trainer should state that this
is a situation somebody you know has encountered. How would you help
them? Participants are more willing to partake in these exercises if they are
not threatened.
Flow Sheets
Flow sheets are visual reminders outlining the steps necessary to solve a
problem correctly. The first step ofthe problem-solving flow sheet pinpoints
the problem. This is followed by selecting possible solutions and evaluating
them according to their advantages and disadvantages. Teaching an individual
with brain injury to use a flow sheet should occur in the following sequence:
(1) Provide a rationale for use of the flow sheet and define the parameters of
its use. For example, one dient may use the flow sheet to facilitate problem-
solving at a job site, while another individual may use it to help cope with
social conflicts. (2) Model how to use the flow sheet for the problem most
often observed. For example, ifthe flow sheet will be used to handle a conflict
situation, then the trainer would follow the steps on the flow sheet for a
hypothetical social conflict. (3) Allow the dient to use the flow sheet for hy-
pothetical situations. The dient should be observed using the flow sheet in
several hypothetical situations. This will provide opportunities for dients to
gain experience using the flow sheet and will allow them to succeed by prac-
ticing. (4) Finally, the dient should always be praised for self-initiating use of
the flow sheet in both practice sessions and real-life situations.
Flow sheets may be the treatment of choice for problems that occur on
a frequent basis. That is, the problem has occurred often in the past or is
currently occurring at a high frequency. Flow sheets also are useful in situations
where behaviors occur in a routine sequence. For example, a dient used a
flow sheet at a job site where he was responsible for completing a ten-step
task. If he became distracted, he would consult the flow sheet to determine
what step of the task he was working on. Flow sheets may not be the best
option in treating problem-solving skills if the individual cannot self-initiate
use ofthe flow sheet. Additionally, flow sheets are not practical to use in all
problematic situations that occur on a daily basis.
Current Events Groups
Current events groups typically begin by having participants read a section
of the newspaper or watch a TV news special or a documentary. Following
PROCEDURES FOR COGNITIVE PROBLEMS 113
this, the trainer asks participants to go through the problem-solving process.
That is, the problem is first pinpointed, possible solutions are formulated,
and fmally the best solution is selected. Because a wide variety ofproblematic
situations can be generated using newspapers or watching TV, all participants
can individually select topics of interest to them. The main disadvantage,
however, is that problems portrayed in the media tend to be social issues
rather than those faced by a brain-injured individual. Thus, it is recommended
that the trainer intersperse problems that are more prevalent among survivors
of head injury and especially those members of the group.
Scheduled Problems
Scheduling problems refers to setting the occasion for the brain-injured
individual to experience a problem in a controlled environment. That is,
problems are predetermined and scheduled to occur at a specific time and in
a targeted environment. For example, a brain-injured individual who lacks
social skills could be brought into the community and placed in situations
where he or she would have frequent contact with others. Zencius et al. (1991)
scheduled problems where the participant had to problem-solve at a vocational
training site. The trainers hid tools and altered machinery which made it
impossible to complete his assigned tasks. The dient had to respond by
searching for the correct tools, reset the power tools, or obtain help from a
supervisor or co-worker. When scheduling problems, the trainer must attend
to three critical considerations. First, the dient must know how to respond
in the specific problematic situation; e.g., if the correct response is to seek
help or to engage in a specific response, then this must be trained first. Second,
the trainer must provide feedback on trials in which the dient encounters a
scheduled problem. Feedback must consist of informing the dient what he
or she did correctly, incorrectly, and what the expected response iso Third,
the trainer must not schedule a problem that is unsolvable or too difficult for
the dient. If the dient does not experience success, he or she will be resistant
to participating in training sessions. Scheduled problems may be the treatment
of choice when preparing brain-injured individuals to respond in new envi-
ronments where they will require specific skills.
PLANNING DISORDERS
Planning is defined as the ability to develop alternatives, consider con-
sequences ofthese alternatives, choosing one ofthese alternatives, developing
a plan, and executing the plan. Planning deficits often have been referred to
as an executive functioning disorder. Lezak (1983) defines executive func-
114 CHAPTER 6
tioning disorders as those involved in the ability to engage in independent,
purposeful, self-directed, and self-serving behavior. Traumatically brain-
injured individuals with planning deficits demonstrate inability to plan events
required in some or all functional domains such as leisure and recreational,
domestic, vocational, educational, and interpersonal. For example, brain-
injured individuals may experience difficulty planning a social activity, plan-
ning steps to obtain employment, organizing a trip, or listing the items needed
at the grocery store to prepare meals for the next week. Burke, Zencius, We-
solowski, and Doubleday (1991) present several strategies for improving ex-
ecutive function disorders. In this section, planning groups, planning checklists,
repeated exposure, and current events groups will be discussed.
Planning Groups
Frequently, rehabilitation centers host menu planning and recreational
planning groups. Three to ten clients and support staff congregate to plan
weekend outings and meals for the week. Although the outcome of a recre-
ational planning group is ultimately to have fun, and the goal of the menu
planning group is to prepare tasty and nutritious meals, several steps are
involved in this planning process including developing alternatives, considering
consequences, selecting one of the alternatives, and developing a plan. For
example, a recreational planning group planning an outing for Saturday eve-
ning would include the following. First, alternatives or options for Saturday
night are identified; e.g., go to the movies, shopping at the mall, attending a
basketball game. Second, consider any consequences that may affect the se-
lection ofthe alternatives; e.g., the cost ofthe activity, what transportation is
available, the location ofthe activity, accessibility for wheelchairs. Third, one
activity is chosen based on the advantages and disadvantages; e.g., although
several alternatives were listed, only one ofthe activities met the criterion for
staying within the budget. Finally, a plan is developed.
All plans are outlined, ensuring that the selected activity will occur suc-
cessfully. For example, if the selected activity was attending a movie and
stopping for ice cream afterwards, then securing transportation to the cinema,
developing time lines and rules, and establishing a budget for all individuals
would have to be done. It is recommended that the information discussed
during the planning group be written down or recorded on a planning form.
Figure 6.16 is an example of a planning checklist. A column for checking off
things to do is provided. Several advantages exist for using a planning form
including: (1) serving as visual reminders, being especially helpful for clients
with memory deficits; (2) providing visual feedback and specifying what has
been completed and what needs to be done; (3) facilitating sequencing of
events; (4) responsibilities can be assigned to individuals; (5) special consid-
PROCEDURES FOR COGNITIVE PROBLEMS 115
PLANNING CHECKLIST
GOAL OR FINAL OUTCOME: ________________ _
TODAVSDATE _______________ _
WHEN IS GOAL TO BE MET? _________________ _
Things That Need To Be Done
Due Date yes no
I.)
2.)
3.)
4.)
5.)
6.)
7.)
B.)
9.)
10.)
11.)
12.)
13.)
14.)
15.)
FlGURE 6.16. An example of a planning checklist.
erations can be outlined, e.g., time lines, transportation schedules, monetary
costs, mIes and regulations; (6) they also can be used for individuals specifying
individual goals.
Planning Checklists
Checklists have been elaborated on earlier in this chapter, and numerous
examples have been provided applying to memory deficits. With planning
disorders, the first step is to determine the goal ofthe checklist. Some examples
116 CHAPTER 6
indude making a phone call, interviewing with an employer, and grocery
shopping. Once the goal is identified, it is written on top of the checklist.
Steps to meet the goal are listed in the sequence to be performed. This could
indude listing all items needed at a grocery store, listing all topics to be dis-
cussed during a phone conversation, listing steps required to enroll in an adult
education course. The final step is to check off each item on the checklist
when completed or attended to. Figure 6.16 is an example of a planning
checklist. It is different from a memory checklist in that there is only one
column for checking off steps. Specific training procedures involved in teaching
a brain-injured individual to use a checklist indude: (1) define the purpose
ofthe checklist, (2) model its use by first selecting a goal and then listing steps
in the proper sequence, (3) observe the brain-injured individual actually use
the checklist both in practice sessions and in real situations. As with training
ofthe problem-solving flow sheet, the trainer should always praise the dient
for using the checklist and provide feedback pertaining to using the checklist
correcdy and incorrecdy.
Illustrative of using a planning checklist to improve planning skills, an
18-year-old brain-injured male at a rehabilitation center made continuous
calls to his mother. He would call his mother collect every evening and talk
for up to 30 minutes without disdosing the purpose of the phone call. After
the phone call, the dient became agitated because he did not discuss all of
the issues. This was resolved by having the dient use planning checklists to
identify the purpose of each call and list all specific topics to be discussed. He
was taught by having staff model filling out a planning checklist and checking
off each item after it had been addressed.
Repeated Exposure
This refers to allowing the brain-injured person to practice planning skills
in real situations over repeated trials. Individuals are provided the occasion
to practice and experience natural consequences in the community. Repeated
exposure consists of three components: (1) identifying the appropriate goal,
(2) formulating a plan to obtain the goal (this consists of identifying all steps
necessary to obtain the goal; it is recommended that the actual goal be written
down or a planning form is used at this step), and (3) use repeated trials.
Feedback is given to the dient by the trainer and in some instances individuals
ofthe community. For example, a 26-year-old male at arehabilitation facility
wanted to obtain employment so he obtained the want ad section from a
newspaper. He began by cirding all available openings and called for inter-
views. Next, he obtained transportation to the interviews. He neglected, how-
ever, to prepare a resume and did not fully understand qualifications for all
ofthe openings. He was turned down at the first interview because he did not
PROCEDURES FOR COGNITIVE PROBLEMS 117
have any experience. Feedback from the employer consisted of informing
hirn that he was not qualified. On his next interview, he obtained help from
staff to understand the want ad information more comprehensively. When
using repeated exposures to community settings, it is important to allow the
individual to experience natural consequences; however, support should be
provided for failures.
Current Events Groups
In addition to teaching problem-solving skills, current events groups are
useful in teaching planning skills. Training occurs in a similar fashion; how-
ever, the focus on training is on the actual formation of a plan once a problem
has been targeted. When the problem is identified and a goal has been pin-
pointed, participants of the group begin formulating a plan. This consists of
identifying all steps or sequence of events that need to occur to obtain the
final outcome. Special attention is given to time lines to be observed, resources
needed, economic considerations, individual responsibilities, and mIes and
regulations.
SUMMARY
Memory Deficits
1. Memory loss is the most frequently reported sequela of cerebral
trauma.
2. Memory deficits can greatly interfere with one's ability to complete
vocational tasks and independent living skills and leam new infor-
mation.
3. The deficits may be a problem with long- or short-term storage, they
may be modality or material specific, or the problem may be in
either encoding, storage, or retrieval of information.
Cognitive Retraining
4. The theory of cognitive retraining refers to retraining brain tissue in
areas of the brain other than those injured so that the uninjured
tissue can perform the lost function.
5. Methods of cognitive retraining include, but are not limited to, writ-
ten rehearsal, verbal rehearsal, acronym formation, chunking, visual
imagery, association, and rhyme formation.
118
CHAPTER 6
6. Five important considerations exist when using cognitive retraining:
(a) Can dients instruct themselves to use the techniques? (b) It is
not practical to use these techniques for everything that needs to be
completed on a daily basis. (c) Several ofthese techniques are time-
consuming. (d) Does generalization to other tasks, situations, or be-
haviors occur? (e) Can the dient with severe memory deficits re-
member to use these techniques?
Compensatory Strategies
7. Compensatory strategies consist of using memory aids to supplement
memory. This is generally established by adding external memory
sources.
8. Compensatory strategies can be divided into three types: storage de-
vices, cuing devices, and restructuring the environment.
9. Written checklists can be used to identify steps of a single task or to
identify tasks that need to be completed on a daily or weekly basis.
10. Memory notebooks have multiple applications induding outlining
daily schedules, listing daily appointments, listing tasks to be com-
pleted, making routine daily entries, and recording new information
learned.
11. Visual cues refer to visual stimuli in the environment that serve as
prompts to engage in a certain behavior.
12. Environmental restructuring involves physically manipulating the
environment in a specified fashion that prompts the dient to engage
in a certain behavior.
Orientation Training
13. Commonly cited characteristics of orientation deficits indude con-
fusion and disorientation to persons, places, and times.
14. The focus of orientation training sessions is on daily schedules; cur-
rent time, day, and date; special appointments; members ofthe ori-
entation group; current events; and current location.
15. Orientation training can be conducted using written information.
Written information is recommended for dients who respond better
to written material.
Attentional Deficits
16. Attentional deficits are defined and measured in terms of an indi-
vidual's ability to attend to a stimulus, task, or situation.
PROCEDURES FOR COGNITIVE PROBLEMS 119
17. The Glasgow Coma Scale, Rancho Los Amigos Levels Cognitive
Recovery Scale, Galveston Orientation and Amnesia Test, and direct
observation are ways to assess attentional deficits.
18. Using environmental restructuring consists of increasing, decreasing,
or eliminating stimuli in the environment to increase attention.
19. Salience of stimuli refers to highlighting the target stimulus to which
the dient is to respond.
20. Other techniques used to increase attention include checklists, self-
monitoring, self-talk, overlearning, altering consequences, and feed-
back.
Self-Awareness Deficits
21. Impaired self-awareness is frequently cited as a serious deficit among
TBI survivors; however, minimal research on effective strategies is
reported in the research literature.
22. Casual observation and the Competency Rating Scale are means of
evaluating self-awareness deficits.
23. TBI education refers to teaching survivors about head injury. Several
components regarding head injury should be introduced including
demographics, anatomy and physiology ofthe brain, residual effects
following head injury, and facts about recovery.
24. Personal adjustment groups attempt to increase self-awareness via
repeated feedback and support.
25. Team integration pertains to including the client in his or her in-
dividualized rehabilitation to the fullest extent possible. Strategies
to obtain this are involving the client in identifying, selecting, and
planning his or her rehabilitation goals, providing individualized
programs for each dient, and inclusion in monthly progress meetings.
26. Allowing TBI survivors to experience natural consequences is a
strategy of increasing self-awareness; however, it is often necessary
to plan safeguards for failures.
27. Video therapy refers to having clients view themselves in problematic
situations. Self-awareness is increased through repeated observation
of oneself.
Problem-Solving Defits
28. The problem-solving process involves identification ofthe problem,
gathering and considering information pertaining to the problem,
exploring possible solutions to the problem, and formulating and
initiating a plan.
120 CHAPTER 6
29. Problematic situations that closely resemble problems of members
of the group should be introduced to problem-solving groups.
30. Problem-solving vignettes are videotaped situations that are prob-
lematic. Participants viewing the vignettes provide possible solutions
to the problems.
31. Flow sheets are visual reminders listing the steps necessary to solve
a problem correctly.
32. Training TBI individuals to use flow sheets includes four components:
providing a rationale for use of the flow sheet, modeling its use,
providing occasions to practice using the flow sheet, and providing
praise for using the flow sheet in both practice and real-life situations.
33. It is recommended that current events groups intersperse real-life
situations that TBI individuals frequently encounter.
34. Scheduling problems consists of setting the occasion for the TBI
individual to experience a problematic situation in a controlled fash-
ion. Problems are predetermined and scheduled to occur at a specific
time in a specific situation and environment.
Planning Disorders
35. TBI individuals with planning deficits demonstrate the inability to
plan events required in some or all functional domains such as leisure
and recreational, domestic, vocational and education, and interper-
sonal.
36. Frequently rehabilitation facilities address planning deficits by having
clients participate in recreational planning groups and weekly menu
planning groups.
37. A planning form has several advantages including: it serves as a
visual reminder, it facilitates sequencing of events, it assigns respon-
sibility to individuals, it outlines special considerations, and it can
be used on an individual basis as weIl as with groups.
38. The purpose of the planning checklist is to identify the goal or final
outcome and list all steps or events, in sequential order, that need
to be completed in order to obtain the goal.
39. Repeated exposure pertains to providing the occasion for the TBI
individual to practice planning skills and experience natural con-
sequences.
Procedures for
Behavior Problems
7
Behavior problems associated with head injury are weIl documented. Authors
often cite the following as common behavioral sequelae of head injury: irri-
tability, impulsivity, egocentricity, impaired judgment, noncompliance, de-
pendency, apathy, tension, sexual disinhibition, and verbal and physical
aggression (Fisher, 1985; Wood, 1988; Zahara & Cuvo, 1984). Many profes-
sionals regard these behaviors as the most difficult barriers to understanding
and treating brain-injured individuals (Lewis, Burke, & Carrillo, 1987). Zahara
and Cuvo (1984) point out that even though many behavior problems exist
prior to injury or are the direct result of injury, many problem behaviors
demonstrated by persons with brain injury are shaped and positively reinforced
by staff and family members. Behavior problems in brain-injured persons
have been treated effectively with applied behavior analysis (Burke & We-
solowski, 1988; Wesolowski & Burke, 1988; Zahara & Cuvo, 1984). In this
chapter, several common behavior problems shown by brain-injured survivors
will be discussed, and approaches that have been effective with these behaviors
will be presented.
NONCOMPLIANCE
Survivors ofbrain injury are often noncompliant with their rehabilitation
regimen. Noncomp1iance can be defined as refusing to participate in treatment
and disobeying the facility's or society's mIes. Zencius, Wesolowski, and Lane
(1991) outlined seven frequent causes of noncompliance: positive reinforce-
ment, negative reinforcement, age, cultural background, memory deficits, ri-
gidity of programming, and neglect of individual interests.
121
122
CHAPTER 7
Staffsometimes inadvertently positively reinforce (attend to) misbehavior
rather than adaptive behaviors. The old saying "the squeaky wheel gets the
grease" applies here. For example, a dient refuses to take her daily prescribed
medication. As a result, caring staff immediately spend additional time with
the dient informing her of the importance of taking medication. In this case,
the presentation of attention maintains the behavior of refusing medication.
Noncompliance resulting in avoidance of an event (e.g., a therapy session
or dass) is negatively reinforced. For example, Sally becomes verbally abusive
when staff tell her to attend dass. As a result, staff discontinue telling Sally
to attend dass. In this case, verbal abuse may increase.
Age and cultural background also contribute to noncompliance. In some
facilities, dients are placed in treatment groups regardless of age or cultural
background. For example, a 52-year-old married male became noncompliant
with his treatment program. An interview revealed that he refused treatment
because of the age of his peers, most of whom were about 22 years old. An
individualized treatment package was implemented for him, which resulted
in 100% attendance.
Memory deficits can cause noncompliance. Individuals with severe
memory deficits often cannot remember their schedules. In a study by Zencius,
Wesolowski, Burke, and McQuade (1989), two dients were initially viewed
as being noncompliant. The first dient would not attend scheduled therapies
and would not use her cane. The second dient often left his workstation for
extended time periods; however, further analysis showed they could not re-
member their daily schedule and expectations.
Facilities usually provide rigid programs, placing dients into groups
without regard for their interests. Illustrative of this is a dient who ran away
from his vocational site at a barn. When the client was questioned about this,
he said he was uninterested in working with animals but liked photography.
He was given a position as the team photographer where he attended 100%
ofthe sessions.
Staff seldom indude the dient in planning the treatment program. AI-
though developing individualized curricula creates more work, individual-
ization increases participation. Functional skills that promote interest could
be induded in curricula such as first aid, automobile maintenance, income
tax preparation, or others.
Consequence Management
Premack Principle
The Premack Principle refers to reinforcing a low-frequency behavior
with a high-frequency behavior (Premack, 1959). That is, doing the dishes or
PROCEDURES FOR BEHA VIOR PROBLEMS 123
using a memory notebook could be reinforced by watehing TV or playing
video games. This approach is useful for prompting behavior (e.g., "Ifyou go
to class in 10 minutes, then we can play cards afterwards"). Several other
advantages ofthe Premack Principle include ease ofimplementation and use
with a variety of noncompliant behaviors, and it can be used immediately
and frequently.
Individualized Point Systems
Points often are used as currency in a token economy (Ayllon & Azrin,
1968). Points can be earned for the occurrence or nonoccurrence of certain
behaviors. In an individualized system, clients receive points for different
behaviors. For example, Joe receives points for going to classes, getting up
on time, and attending his vocational site. Sarah receives points for going to
classes, not exhibiting temper tantroms, and practicing stress management
but does not get points for getting up on time or attending her vocation-
al site.
The most important thing to remember about point systems is to use
points to address the client's needs. Figure 7.1 shows behaviors that could
earn points for a noncompliant adolescent. Points are exchanged for items
or privileges usually on a daily or weekly basis (e.g., choice of video, money,
community outing). Figure 7.2 shows items and activities that could be pur-
chased. Point systems are useful when several behaviors have been targeted
for change.
Individual point systems sometimes include response cost contingencies,
i.e., points are subtracted for occurrences of misbehavior. For example, not
onIy would a client not earn points for skipping therapy, but there also would
be a fine for this behavior. We recommend starting point systems on a positive
basis (i.e., points are only earned). Ifthe behaviors are still not under control,
then response cost can be initiated. It is important with an individual point
system to reinforce behaviors that are incompatible with noncompliant be-
haviors. For example, ifthe behavior is violating roles, then reinforce following
roles with a large number of points.
Zencius, Wesolowski, and Burke (1989) placed two adolescents on be-
havior contracts, individual point systems, and daily check systems to increase
compliance. In both cases, behavior contracting was introduced first. The
adolescents could earn a special activity if they participated in 90% of programs
for 5 consecutive days. Next, both adolescents were placed on individual
point systems. Points could be earned for punctuality, attending an entire
session, participation, and hygiene activities. Points were redeemable for pre-
ferred activities, community outings, and money. The point system was con-
tinued for 13 days with the first adolescent (Linda). Because her compliance
124 CHAPTER 7
6EHAVIORS THAT EARN POINTS
6eing on time ........................................................................ 50 pOints
Attending entire work session ...................................... 75 points
Attending entire therapy session ................................. 60 pOints
Working on task .................................................................... 1 0 pOints
Following instructions ...................................................... 1 0 pOints
Accepting criticism ............................................................ 15 pOints
Accepting "NO for an IInswer ......................................... l 0 points
Asking permission... ............................................................. 5 points
Helping others or sharing .................................................. 5 pOints
Extending compliments to others .................................. 5 pOints
6eing honesl.. .......................................................................... 5 points
Watehing educational progrom .................... " ................. 15 points
Watching TV news or reading newspaper .................. 20 pOints
Working on homework assignments ............................. l 0 points
Reoding books ......................................................................... l pt/page
Cleaning room ........................................................................ l 0 points
Completing daily chore ...................................................... 15 points
Completing a bonus chore ................................................. l0 points
Ooing own lllundry on time ...................... " ....................... 20 points
Setting the table .................................................................. 10 points
Preparing a side dish for dinner .................................... 15 pOints
Washing the dishes .............................................................. 15 pOints
FlGURE 7.1. Examples ofbehaviors that could eam points in token economy.
was maintained at high levels, she was next placed on a daily check system.
That is, she received a daily check worth $2.00 if she participated in 100% of
activities. Following 13 days on the check system, she was told that if she
attended all therapy sessions, she could participate in evening and weekend
outings.
The second adolescent (Al) remained on a point system for 20 school
days. Response cost contingencies were then added to the point system. Al
was fined for not attending therapy sessions. The point system was continued
with a response cost system for 35 school days, and Al was placed on acheck
system similar to Linda's. Results suggested that all motivational systems
were effective in increasing compliance (Figures 7.3 and 7.4).
PROCEDURES FOR BEHA VIOR PROBLEMS 125
THINGS POINTS CAN BUY
Money. . ............................. 1 pt. = 1 cent
Bonus TV time.......... . .......... 200 pts.lhour
up past bed ti me ............................... 200 pts.lhour
Additional snacks ....................................... 50 points
First choice of video ................................. 100 points
Vi si t the game room .................................. 300 pts.lhour
Playing games with favorite staff ..... 150 pts.lhour
Wal k to the store ...................................... I 00 poi nts
Trip to shopping mal1... ............................. 500 points
Movi e theater ................................................ 500 poi nts
Pizza out... ..................................................... 600 pOints
Weekend pass ................................................ 1 000 points
Trip to facility gymnasium .................... 300 points
[anoe on the lake (Saturdey) ................. 600 points
Help make cookies ...................................... 200 points
Use polaroid camera .................................. 50 pts.lhour
First choice to menu plan ....................... l00 pOints
FlGURE 7.2. Examples of items and activities that could be purchased with points in a token
economy.
Group Point Systems
Point systems can also be applied to groups of clients. In group systems,
an individuals are equally reinforced for a set ofbehaviors (e.g., clients receive
the same amount of points for attending therapies, following instructions,
cleaning their room). One advantage ofusing group point systems is that they
are easy to implement (i.e., all clients receive the same number of points for
targeted behaviors, one documentation system serves all clients, and all target
behaviors apply to all clients). The obvious disadvantage of group point systems
is that they are not individualized.
1
2
0
-
B
A
S
E
C
O
N
T
.
B
A
S
E
P
T
.
S
Y
S
T
E
M
C
H
E
C
K
S
Y
S
T
E
M
A
C
T
M
T
I
E
S
0
1
0
0
U
J
-
,
.
.
6
0
-
1
!
3
I
n
I
n
(
.
>
6
0
-
0
I
4
0
.
,
,
.
.
.
-
w
a
.
.
2
0
o
1
0
2
0
3
0
4
0
5
0
6
0
S
C
t
K
X
X
.
O
A
Y
S
F
I
G
U
R
E
7
.
3
.
T
h
e
e
f
f
e
c
t
s
o
f
a
p
o
i
n
t
s
y
s
t
e
m
,
c
o
n
t
r
a
c
t
s
,
a
n
d
a
c
h
e
c
k
s
y
s
t
e
m
t
o
i
n
c
r
e
a
s
e
L
i
n
d
a
'
s
d
a
s
s
a
t
t
e
n
d
a
n
c
e
.
N
'
"
(
j
:
:
c
:
:
>
t
T
l
:
:
:
e
-
.
)
s
C
l
f
I
3
t
n
t
n
:
s
l
)
L
I
.
.
o
:
s
w
I
l
.
.
.
1
0
0
.
.
.
,
"
'
"
T
"
1
.
"
6
0
.
.
4
0
2
0
B
S
P
O
I
N
T
S
Y
S
T
E
M
&
R
E
S
P
O
N
S
E
C
a
S
T
1
T
T
T
n
1
1
1
1
0
0
'
)
'
.
f
a
,
3
0
c
a
n
s
e
c
u
t
i
v
e
d
a
y
s
o
j
.
'
'
.
I
I
"
,
I
o
2
0
4
0
6
0
6
0
S
C
I
I
O
O
l
O
A
Y
'
S
F
I
G
U
R
E
7
.
4
.
T
h
e
e
f
f
e
c
t
s
o
f
c
o
n
t
r
a
c
t
s
,
a
p
o
i
n
t
s
y
s
t
e
m
,
a
n
d
a
p
o
i
n
t
s
y
s
t
e
m
w
i
t
h
r
e
s
p
o
n
s
e
c
a
s
t
t
o
i
n
c
r
e
a
s
e
A
J
'
s
d
a
s
s
a
t
t
e
n
d
a
n
c
e
.
"
'
0
;
x
l
X
t
'I
'1
o
c
:
:
;
x
l
t
'I
'1
V
J
C
l
;
x
l
0
'
t
'I
'1
:
:
c
>
-
<
;
x
l
"
'
0
;
x
l
o
0
'
V
J
N
-
.
J
128 CHAPTER 7
Leveled Programs
Leveled programs are token economies in which different behaviors are
expected at different stages (levels). Initial levels require easy-to-perform be-
haviors to obtain reinforcers. Higher levels require more difficult behaviors
with more potent reinforcers. For example, at the lowest level, dients are
expected to attend only 60% of all therapies, follow 60% of all house mIes,
and earn 60% of all points at a vocational training site. For this, they would
be entitled to only one community outing a week and house privileges. At
the highest level, dients are expected to attend 95% of all therapies, follow
100% of house mIes, and earn 100% of all points at the vocational site. For
this, dients would qualify for three community outings a week, a later curfew,
independent sign-out, and first choice of a video.
The advantage ofleveled programs is similar to that of group point systems
(i.e., easy to implement by staffand convenient to use in small group settings).
The disadvantage of leveled programs is they are not individualized. Figure
7.5 shows the availability ofreinforcers and expected behaviors at those levels.
Note how availability of reinforcers varies from level 1 to level 4.
Behavior Contracts
A behavior contract is a written agreement between the dient and a
family or staff member. The contract specifies which behaviors are to occur
and not occur. Ifthe dient adheres to the contract, then certain consequences
follow. Ideally, a behavior contract should indude seven elements: (1) defi-
nition ofthe behavior, (2) some criterion for meeting the contract, (3) positive
reinforcers for fulfilling the contract, (4) aversive consequences for not fulfilling
the contract, (5) bonuses for exceeding the original criterion, (6) specification
of observation methods, and (7) scheduling of positive reinforcers.
One advantage of behavior contracts is that they are individualized to
dient needs. A second advantage is later contracts can be used to increase
demands or extend the interval of reinforcement. The disadvantage is that
once the contracts are met, the behaviors may reoccur unless a new contract
is initiated immediately (Zencius, Wesolowski, & Burke, 1989). Once a con-
tract is met, a new contract should be initiated immediately. Figure 7.6 is an
example of a behavior contract used to increase attendance to physical therapy
sessions. Figure 7.7 is a blank behavior contract form.
The interval of the contracts can become longer. For example, the first
contract could be 2 days in duration, the second could be 3 days, and the
third could be 4 days. This results in the interval between reinforcements
being extended. The contract also can become more difficult to meet by raising
the criterion (e.g., the first contract could specify 50% attendance, and the
PROCEDURES FOR BEHA VIOR PROBLEMS 129
LEVEL EXPECTATIONS & REINFORCER AVAILABILITT
LEVELS EXPECTATIONS & BEHAVIORS REINFORCERS
Leve1
6
1
1.) 1.)
2.) 2.)
3.) 3.)
Level -2
1.)
1.)
2.) 2.)
3.) 3.)
4.) 4.)
5.) 5.)
Level -3
1.) 1.)
2.) 2.)
3.) 3.)
4.) 4.)
5.) 5)
0.) 0.)
7.) 7.)
Level -4 1.) 1.)
2.) 2.)
3.) 3.)
4.) 4.)
5.) 5.)
0.) 0.)
7.) 7.)
6.) 6.)
9.) 9.)
10.) 10.)
Graduated token economy. Specify expectations to remain
off the token economy be10w U.e . contracts. etc.).
FIGURE 7.5. A form to show the availability ofreinforcers and expected behaviors at different
levels in a token economy.
second contract could increase this to 60%). It is important that the dient
easily complete the first few contracts, thus experiencing reinforcement. A
behavior contract should never be initiated that is too difficult or impossible
to attain.
Antecedent Control Techniques
Antecedent control techniques refer to manipulating the variables that
evoke a behavior. Antecedent control techniques should be considered when
130
NAME: JOAN JOHNSON
FROM: SAMUAL ADAMS
DATE: JUNE 20, 1993
Beh.vlors to occur:
Attendance to physical therapy sessions.
Crlterlo n to meet contrsct:
CHAPTER 7
Joan mus! attend all 5 scheduled physical therapy sessions during the week
01 June 22-27th. She mus! be present for 50 minutes of the scheduled session.
Rewsrd for meeting contrsct:
Lunch out.
Rewsrd to occur when .nd where (explsln event or sctlvlty):
Reward to occur on June 27th at 11 :45 am. Samual will pick up Joan at her
residential setting. They will proceed to the Route16 Diner for lunch. Money
will be provided by the team leader ($6.00 limit).
Bonu88s for exceedlng orlglnsl contrsct:
For attending 10 consecutive physical therapy sessions, Joan will be entitled
to an additional 15 minute long distance phone call. This can occur between
the hours of 7:00 pm-10:00 pm on any Thursday or Friday.
Observstlonsl Method:
The physical therapist will observe and record the duration 01 minutes that
Joan was present at each physical therapy session. This will be recorded on
the daily treatment summary form following each scheduled therapy session.
Wrltten Agreement:
Joan Johnson ___________ _
Samual Adams, __________ _
Team Leader ___________ _
FIGURE 7.6. Example of a behavior contract.
severe memory deficits have been observed, when consequence management
techniques have failed, or when the dient often forgets components of his or
her daily schedule (Wesolowski & Burke, 1988; Wesolowski, Zencius, & Burke,
1988). Antecedent interventions were discussed in Chapter 6; however, an-
tecedent control techniques that have been effective in dealing with noncom-
pliant behavior will be introduced in this section.
Maps
Zencius, Wesolowski, Burke, and McQuade (1989) used maps to increase
a client's attendance to therapy sessions. The map enabled her to find her
way to the sessions. Landmark discrimination training is also a useful strategy
(e.g., marking trees, telephone poles, buildings, roadways, signposts) providing
cues in the environment.
PROCEDURES FOR BEHA VIOR PROBLEMS
131
BEHAVIOR CONTRACT
NAME: ________________ __
FROM: ________ _
DATE: _________ _
Behavior(s) to occur:: ________________________ _
Criterion to obtuin contract: __________________ _
Rewanl tor obtaining contract:. __________________ _
Reward to occur when & where (explain event): __ _
Bonus tor exceedlng original contract:. ____________ _
Observatlonal methods: ______________________ _
Notes:: ____________________________________ __
FIGURE 7.7. A blank behavior contract form.
Pictures
Pictures can be used for nonreaders or clients who respond better to
pictorial versus written information. For example, pictures can be used to
show clients steps for preparing a meal, setting a table, or changing oil in a
car. Illustrative ofusing pictures, a 21-year-old female client could not perform
routine tasks in a culinary arts program. This was resolved by taking a picture
of each step of the task and presenting her the pictures in the proper sequence.
Verbal Cues
Verbal cues function as reminders to perform a behavior. Examples in-
clude: "We are leaving for grocery shopping in 5 minutes," "Remember, you
132 CHAPTER 7
get five points for going to therapy," and "Using your dayminder helps you
be more independent." It is important not to nag the dient when providing
verbal cues. Rather, asking them to help you or asking for their advice are
good ways to provide verbal cues, e.g., "Its three o'dock now, could you help
me copy schedules for tomorrow's activities?" or "I could use help in my
session today, could you give me ahand?"
Environmental Design
Any changes made in the physical environment or dient's daily schedule
are environmental design techniques. Some examples indude labeling cup-
boards, use of pictures, audio cassettes for cooking, tape on the floor to help
identify boundaries, automated cues (docks, alarms, and timers), placing a
cue card at somebody's workstation, and changing the location of a study
table. To illustrate this, a dient was viewed as noncompliant in completing
his vocational tasks in a woodshop. Observations revealed that the dient was
distracted by peers, staff, and noises. A study carrel was built around his
workstation, which helped reduce distractibility.
AGGRESSION
Aggression is the most troublesome behavior that occurs in persons with
brain injury. Uncontrolled aggression speIls rehabilitation failure. In the early
stages of recovery, most aggression is caused by confusion and compounded
by the alien surroundings of the acute hospital ward. As confusion resolves,
the most common problem is one of general irritability which settles over
days or months. As disabilities become evident and the individual's awareness
of limitations increases, it is not uncommon for the survivor of brain injury
to become frustrated and angry. The anger seems most prominent as the
individual's denial diminishes. The resulting anger over lost function is nat-
urally directed at family members and therapists. This anger can quickly turn
to aggression as individuals will destroy property or assault family and staff
members. To understand the treatment of aggression, we must first consider
some of its causes.
Causes of Aggression
Learning
Aggression can be either positively or negatively reinforced. With positive
reinforcement, aggression is followed by a stimulus that results in increased
PROCEDURES FOR BEHA VIOR PROBLEMS 133
aggression. For example, a dient has atemper tantrum and turns over fur-
niture. Staff immediately attend to the outburst and provide attention. In this
case, the stimulus of staff attention is reinforcing the tantrum. With negative
reinforcement, the aggression is followed by the removal ofa stimulus, which
results in increased aggression. For example, an aggressive dient (Joe) does
not like the presence of another dient (Bill) in the recreation room. When
Bill enters the room, Joe strikes Bill. This results in Billleaving the room. In
this case, Bill is the stimulus being removed thus reinforcing assaultiveness.
Aversive Treatment
Aggression can be caused by certain aversive antecedents. In most cases
of aggression, several stimuli are antecedents to the behavior. Aversive treat-
ment such as name calling, staff saying "no," unrealistic expectations, and
dients' requests being turned down can cause aggression. When asking staff
about their dients' aggression patterns, they frequently daim there are no
antecedents. Although this may appear true, there are almost always ante-
cedents to aggression. Some aversive antecedents to aggression that are difficult
to detect can indude anniversary of injury date, realization of deficits, for-
getting things, hearing voices, and an inability to communicate needs.
Pain
Azrin (1967, 1970) and his colleagues have extensively investigated the
relationship between pain and aggression. The more intense the pain and the
longer its duration, the greater is the likelihood of aggression. Attack responses
are indiscriminately aimed at people and inanimate objects. It is common
for dients to experience some level of physical pain such as neck pain, joint
and muscular pain, body aches, headaches, and dizziness. For example, a
dient at arehabilitation facility became aggressive and destroyed property. It
was later observed that these episodes covaried with headaches. The dient
was taught to isolate himselfwhen experiencing a headache, thereby reducing
aggression.
Changes in Reinforcement
Unfavorable changes in positive reinforcement also may be aversive and
produce aggression. After individuals come to expect their actions to be re-
warded at a certain level, withdrawal or reduction of positive reinforcement
serves as an aversive event. For example, a dient was usually rewarded for
performing house chores. When moved to a new residence, he was no longer
expected to perform these chores. Every time the dient completed a chore,
134 CHAPTER 7
no consequence followed; this resulted in aggression. When the nature of
aggression was revealed, completing chores again received reinforcement.
Physiological Causes
With survivors ofbrain injury, it is not uncommon to observe aggression
that is explosive, dramatic, and usually brief. These types of aggressive episodes
are called episodic dyscontrol syndrome, temporal lobe epilepsy, or limbic
epilepsy. This syndrome usually occurs some months after the head trauma,
though it may be delayed for years. Outbursts appear to be unprovoked or
triggered by trivial frustrations and never by substantial provocation. These
symptoms are clearly associated with anterior-medial temporaliesions affecting
limbic structures and may even occur after moderate head injury.
It must be remembered, however, that even though aggression may be
elicited physiologically, learning does occur. Physiological aggression will take
on instrumental properties if it has functional value.
Skill Deficits
Research has shown that people who have a propensity for getting into
fights are lacking in verbal and social skills. Socially adept individuals are able
to defuse potentially explosive situations through various social techniques
including pacifying moves, humor, and friendly persuasion. Clients who have
limited verbal and social skills are more likely to become aggressive on slight
provocation. By enlarging their social repertoire, aggressive clients can leam
new strategies in dealing with a potentially violent situation. For example, a
newly admitted client with dysarthria and minimal verbal skills became phys-
ically aggressive and destroyed property when he was unable to communicate
his needs. Daily therapy with a speech therapist and behavior analyst focused
on expressing his needs. This resulted in a decrease in aggressive episodes.
Treatment 01 Aggression
The leaming principles that account for the development of aggressive
behavior apply equally to its treatment. Since aggression is largely under sit-
uational, cognitive, and reinforcement control, these are the events to which
treatment must address itself, rather than to traits, presumed drives, or his-
torical causes. Treatment programs based on learning principles differ from
those relying on counseling. With regard to content, treatment procedures
are applied to the actual problem behaviors requiring change, instead of verbal
reports of trouble. Staff should devote their efforts to altering social conditions
PROCEDURES FOR BEHA VIOR PROBLEMS 135
rather than conversing about them, as so often happens in approaches using
the interview as the vehide for modifying behavior.
Consequence Management
Several consequence management techniques can be used in treating
aggression. These indude token economies, behavior contracts, and the Pre-
mack Principle. When using consequence management, the nonoccurrence
of aggression usually is reinforced. An emphasis is placed on behaviors in-
compatible with aggression. For example, cooperation, participation, relax-
ation, and good social skills might be heavily reinforced because they are
incompatible with aggression. Several consequence management programs
have been published. Wood (1988) placed a 17 -year-old adolescent male on
a token economy for participation in therapy sessions. Prior to implementing
the token economy, the adolescent became aggressive and argumentative in
dass. Intervention entailed giving the adolescent tokens contingent on par-
ticipation in therapies. The tokens were exchanged for food or extra break
periods. As the level of participation increased in therapies, a decrease in
aggression was noted.
Consequence management also was used successfully by Wesolowski and
Zencius (1992), where an adolescent exhibited aggression requiring physical
intervention. A point system with response cost and contingent horne visits
was used to reward appropriate behavior and fine specific misbehavior. Spe-
cifically, points were earned for attending dasses, using good social skills, and
not becoming physically aggressive. The adolescent exchanged points daily
and weekly to redeem individual outings, extra snacks, additional basketball
time, additional time to listen to the stereo, and money. In this case, the
aggressive behavior was suppressed over 11 weeks (see Figure 7.8). Staff re-
ported that in addition to eliminating aggression, the point system increased
attendance to dasses, waking up on time, and prosocial behaviors.
Verbal and physical aggression was decreased in a brain-injured male
using differential reinforcement of low rates of behavior (Turner, Green, &
Braunling-McMorrow, 1990). Ifthe participant demonstrated a low frequency
of aggression over a certain intervaI, he was awarded points. Points were
totaled for a weekly goal.
In another study, Zencius and Wesolowski (1991) eliminated verbal
aggression in a 26-year-old male dient through behavioraI contracts for special
outings (e.g., rock concerts, trips to the mall, dining out, cookouts with pre-
ferred staff). During baseline, the dient demonstrated two to eight verbal
outbursts per week. The outbursts lasted as long as 10 minutes. Behavior
contracts decreased the occurrences of verbal outbursts to near zero levels.
In a second dient, verbal aggression was eliminated using restitution (apology),
136
c
o
'00
CI)
Q)
OJ
Cl
<{
"iii
u
'Vi
>-
..c
0..
5
4
3
2
o
CHAPTER 7
BASELINE PT.SYSTEM & V1SITS BASE POINT SYSTEM
10
20 30
Time in Weeks
FlGURE 7.8. The effects of a point system and horne visits on aggression.
response cost in a point system, and a bonus 15-minute phone call if there
was no aggression that day.
Videotape Feedback
Videotape feedback occurs in small group settings (two to five clients)
where new modes of behavior are modeled and practiced. Nonviolent ways
of handling antagonists and troublesome situations can be demonstrated ef-
fectively through role-playing. Actual demonstrations may be supplemented
with videotaped modeling of successful responses to common problems. To
produce skills that can apply to many situations, the treatment should em-
phasize general strategies rather than specific responses. In other words, show
models handling diverse problems in similar ways. For example, a videotape
could show a model handle a problematic person in different situations.
Performance feedback, which provides information for corrective action,
is thus required to realize the full benefits of rehearsal. Reports of onlookers
may be of some help, but the explicit feedback by videotape is ideally suited
for this purpose. Through immediate videotape playback, clients can observe
their performance including tone of voice and mannerisms. Successful ac-
complishments are noted while aspects oftheir performance requiring further
improvements are pointed out.
PROCEDURES FOR BEHA VIOR PROBLEMS 137
If videotape equipment is not available, role-play can occur without it.
Again, situations that are problematic should be role-played. Each role-play
session should indude non violent ways of handling the problem situation.
These can be introduced by the group facilitator. For example, for the dient
who becomes agitated by a roommate, several role-play situations could be
established (e.g., talking to the roommate, asking the roommate to make a
written agreement, consulting staff regarding the problem). Following the role-
play situation, contingent feedback should be provided to the dient. Infor-
mation regarding how the situation was handled, use of social skills, and
positives and negatives should be addressed.
Alternative Behaviors
Individuals may be reluctant to discard aggressive modes of responding
as long as the behavior remains valued or reinforced. Cultivation of social
competence may have to be accompanied by devaluation of assaultiveness.
In altering a person's basis for self-evaluation, one must consider the ethical
issues involved. Anyone who sets out to change standards of self-reinforcement
should be prepared to teach new styles of behavior that serve as more self-
satisfying alternatives. For example, a dient at a facility becomes aggressive,
wh ich results in additional attention from staff. In this case, the dient would
be taught to obtain staff reinforcement in a more appropriate fashion. The
dient could be taught to compliment others, volunteer to help others, and
share with others, which would result in more staff attention.
When teaching alternative behaviors, it may be convenient to tie in a
motivational system. That is, use reinforcing contingencies for the new alter-
native behavior. The self-evaluative consequences of aggressive behavior can
be alte red to some extent through the judgments expressed and modeled by
staff and family members. lt might be pointed out, for example, that the risk
of permanent physical injury is a high price to pay for glory or a temporary
boost in self-esteem, that it is much smarter to dispose of an antagonist by
one's wits than by one's fists, and that hasty fighters become easily manipulated
by others who discover how to provoke them to foolhardy acts. An assaultive
person is apt to exercise better control over his behavior if he also knows
which things easily goad hirn into violent actions.
Repeated Use
When people are taught new ways of responding, there may be a tendency
to view the changes as artificial. For example, significant others may report
that changcs only occur at certain times and in the presence of select people.
Any new skilI, regardless ofhow it is acquired, is initially performed awkwardly
138 CHAPTER 7
and self-consciously. With repeated use, however, the actions are executed
spontaneously as part of one's natural style. To illustrate, an aggressive dient
was taught to use "good social skills" to get along better with others. Initially,
these social skills occurred in front of the primary trainer. Next, the use of
good social skills appeared in the presence of other staff, family members,
and finally in the presence of peers. But participant modeling does more than
teach skills. If people behave in new ways, eventually their attitudes change
in the direction oftheir action. Indeed, numerous studies have demonstrated
that one of the most effective methods of altering attitudes and values is by
producing a change in the behavior.
In addition to repeated use ofnew or alternative'behavior, the individual
must experience reinforcement for engaging in that behavior. If reinforcement
is not experienced for engaging in a new behavior, then the new behavior will
not continue to occur. Thus, it is important when teaching new behaviors
that we ensure the individual experience reinforcement for the new nonag-
gressive behavior. To illustrate, a physically aggressive dient was taught to
leave the environment when he was being teased by others. In the past, when
the dient was teased, he became aggressive. In this case, every time the dient
left the environment, he was praised by staff who spent additional time with
him. Eventually, the dient required no praise. The behavior ofleaving became
intrinsically reinforcing to the dient. When providing reinforcement to the
dient, it is important to remember to use reinforcers that can be easily faded
out across time or can be changed to natural reinforcers.
Redirection
Head-injured dients frequently become confused and disoriented. This
is especially true in the acute stage of recovery but may occur for several
years. Sometimes this confusion facilitates aggression. Redirection refers to
refocusing the dient's attention away from the provoking stimulus (person,
situation, event) onto a different subject. Two types of redirection can be
used: specific and generic. With the latter, redirection to any stimulus can be
used (using a joke, focusing on a TV show, asking questions). With specific
redirection, the person providing the redirection does so to a predetermined
script. All caregivers use the specific script to redirect the dient at the first
sign of agitation. For example, when the dient is becoming agitated, staff
respond consistently by asking the dient to come with them to read the news-
paper. What has been effective in the past will determine what the standardized
script will be. Some dients may be redirected by reading, leaving the immediate
environment, listening to jokes, or playing agame. With both types of redi-
rection, the caregiver should change the conversation from the provoking
stimulus to a new topic. Most importantly, the staff should not perseverate
PROCEDURES FOR BEHA VIOR PROBLEMS 139
on topics that are agitating the client. For example, if the client is becoming
agitated over her meal, a staff or family member should not make statements
such as "Y ou better eat your meal right now" or "Y ou like this." Rather, the
caregiver should redirect by asking questions such as "What was the final
score ofthe game last night?," "Did you see the end ofthe movie last night?,"
"What should we do for a leisure activity tonight?" As noted above, redirection
is best used when stated in the form of a question. This forces the client to
briefly change topics. Questions that require a simple yes or no response are
not as effective. One consideration when using redirection is that it does not
actually change the behavior. It can be used to "buy time," however, while
other strategies are being tried. Also, redirection is most effective with people
with severe memory deficits. That is, individuals with severe memory deficits
frequently do not learn as weIl from repeated consequences and sometimes
do not remember their aggressive behavior. Thus, antecedent interventions
versus consequence management techniques may be the treatment of choice.
Stress Management Training
Stress management training has been used for years to treat anxiety
(Suinn, 1975; Suinn & Richardson, 1971). Stress management training consists
of at least two components: recognizing early signs of stress and relaxation.
Individuals with brain injury often have increased stress resulting in aggression.
Thus, it is important to recognize the early signs of aggression so action can
be taken to avoid it. The following three-step stress management procedure
has been effective in dealing with aggression: (1) The client should be taught
to identify a stressful state. The individual is trained to identify stressful be-
haviors in self (e.g., muscle tension, pacing back and forth, clenched fists).
Every client demonstrates different characteristics when experiencing stress.
Thus, it is important to watch for these rather than use the same indicators
for all clients. (2) The client should leave the immediate environment and go
to adesignated relaxation area. Clients may want to choose several environ-
ments as targeted relaxation areas. Arelaxation area may be selected for each
environment they are in each day. For example, a client may have a targeted
relaxation area at the vocational training site, at the residential setting, and
at his or her parents' horne. When selecting a relaxation area, one should
choose an environment that is easily accessible and free of distraction. (3) A
form of relaxation training should be selected. Several options include deep
breathing, counting backward, visual imagery, autogenie training, and pro-
gressive muscle relaxation. Whatever technique is selected, the client should
be able to use it independently after a few training sessions since the trainer
will not always be available.
140 CHAPTER 7
When using the above procedure, it is recommended that training sessions
occur at least twice a week. The client also should practice using the relaxation
procedure twice a day independently. Zencius and Wesolowski (1990) used
this three-step stress management technique to treat a 29-year-old brain-
injured female who ran away from the facility and refused medication when
she became agitated. Training consisted of role-playing stressful situations
and then engaging in the three-step stress management procedure. The client
was to practice relaxation procedures three times a week and whenever she
feit anxious. In this case, relaxation consisted of deep breathing and an ab-
breviated form of progressive muscle relaxation. After 8 weeks of treatment,
only one episode of running away occurred. Also, no runaways occurred
during 26 weeks of follow-up. Figure 7.9 shows the effects of baseline, stress
management training, and follow-up. Figure 7.10 is a stress management
form that highlights these three main components of stress management.
INAPPROPRIATE SEXUAL BEHAVIOR
Sexual dysfunction is not rare followipg brain injury (Blackerby, 1987,
1988; Lezak, 1978). Kosteljanetz and colleagues (1981) found sexual dys-
function (reduced libido or erectile dysfunction) to be related to the postcon-
cussion syndrome in 58% of the 19 men studied. BoIler and Frank (1982)
found that 35% of brain-injured clients experienced decreased frequency of
sexual relations. Sexual disorders and alterations of sexual relationships caused
by brain injury have been neglected in the literature. Many treatment programs
from acute care to independent living either ignore these issues or deal with
them in a superficial way. Indeed, many professionals are uncomfortable dis-
cussing sexual issues.
Sexually inappropriate behavior can be defmed as behavior, explicitly
sexual in nature, that is harmful physically or emotionally to the individual
or persons in one's environment. Little data are available on hypersexuality
after head injury. Ducharme (1987) suggested that hypersexuality is not com-
mon; however, a high degree ofimpulsivity involving inappropriate sexuality
may appear in clients with frontal lobe injury. Hypersexuality also can occur
with either temporal lobe seizures or surgical rem oval of the temporal lobes
or limbic lesions (e.g., Kluver-Bucy syndrome). Research suggests that hy-
posexuality occurs more often than hypersexuality. Miller, Cummings,
McIntyre, and Ebers (1986) studied eight clients after brain injury described
as hypersexual or homosexual. Neuroanatomical correlates ofhypersexuality
were found to be the medial basal-frontal or diencephalic areas, and changing
sexual preference was seen with limbic system damage.
8
b
I
J
)
C
I
J
)
Q
)
-
E
m
Q
)
:
:
:
:
I
0
.
-
o
Q
)
_
C
I
l
o
u
>
-
'
6
U
Q
)
2
:
:
:
:
1
"
0
C
T
C
C
I
l
U
-
0
B
a
s
e
l
i
n
e
-
,
0
S
t
r
e
s
s
M
a
n
a
g
e
m
e
n
t
1
0
T
i
m
e
i
n
W
e
e
k
s
b
M
O
N
I
H
N
O
E
P
I
S
O
D
E
S
o
r
E
L
O
P
E
M
E
N
I
S
O
R
M
E
D
I
C
A
I
I
O
N
\
2
0
F
I
G
U
R
E
7
.
9
.
T
h
e
e
f
f
e
c
t
s
o
f
s
t
r
e
s
s
m
a
n
a
g
e
m
e
n
t
t
r
a
i
n
i
n
g
o
n
t
h
e
f
r
e
q
u
e
n
c
y
o
f
e
l
o
p
e
m
e
n
t
s
a
n
d
m
e
d
i
c
a
t
i
o
n
r
e
f
u
s
a
l
s
.
"
'
0
'
"
g
t
T
1
o
C
'
"
t
T
1
[
/
)
;
:
g
'
"
t
t
I
t
T
1
:
:
r
:
:
;
p
<
'
"
"
'
0
t
t
I
r
t
T
1
s
:
:
[
/
)
+
>
-
142 CHAPTER 7
PRACTITIONER/CLIENT STRESS MANAGEMENT FORM
LIST SIGNS OF EARLY AGITATlON, __________ _
[ LIST SlG", 0' 'ATE AG'TATOON
1
IOENTIFY & LIST RELAXATION AREAS FOR ALL ENVIRONMENTS:
IJ Home
2J Work
3JSchool
4 .)Pllrents home
SJOther specify
6,) other specify
WHAT TYPE OF RELAXATION PROCEDURES WILL BE USED ?
LIST SPECIFIC PROCEDURES BELOW
(1.)
)
)
)
)
FIGURE 7.10. A stress management form.
Valentich and Gripton (1986) present a psychological framework for the
sexual functioning of brain-injured individuals and recommend systematic
evaluation of sexuality of brain-injured persons. They suggest intervention
for inappropriate sexual behavior to include social skills training, cognitive
restructuring, assertiveness training, and behavioral assignments. Wesolowski
and Burke (1988) also discussed interventions for maladaptive sexual behavior
in brain-injured individuals. These include dating skills training, self-
PROCEDURES FOR BEHA VIOR PROBLEMS 143
monitoring of sexual urges and fantasies, scheduled staff feedback with re-
inforcement, and massage therapy to shift stimulus control to appropriate
settings.
Before any therapeutic intervention for sexual misbehavior is attempted,
a private, detailed interview with the dient must be performed. It should
probe the dient's sexual urges, feelings, desires, and fantasies regarding the
target behavior and sexuality in general.
Dating Skills Training
Dating skills training should occur in small groups (e.g., two to four
dients). Both male and female therapists should be present. Training begins
by providing a rationale for the skill being taught. For example, if the skill
were introducing oneselfto a member ofthe opposite sex, the therapist would
verbally describe why the skill was important. The therapist then models the
skill being taught. Next, the therapist should ask one of the members to role-
play the situation with another dient or trainer. Finally, feedback is given.
Feedback should always begin by pointing out the things done well followed
by behaviors that could be improved upon. This sequence should be used in
introducing all new skills to the group. Specific dating skills should be deter-
mined by the group's needs. Skills such as maintaining eye contact, saying
"Ri," initiating conversations, making phone calls, greetings, and conversa-
tions on a date are good to start with followed by real-life situations. Through
these situations, sessions become more individualized. To illustrate this, a
shy adult male had difficulty interacting with females. In his case, dating skills
training emphasized role-playing conversations with females in various sit-
uations (e.g., asking for assistance, introducing hirnself, making a phone call).
Another component of dating skills training is homework assignments. In
this illustration, the shy individual's homework assignment was to initiate at
least one conversation per day with a female.
Clients demonstrating dangerous sexual behaviors should be taught ap-
propriate ways to interact with members ofthe opposite sex. Too frequently,
the dient demonstrating maladaptive sexual behaviors is only punished. This
decreases the behavior; however, it does not teach the dient appropriate re-
sponses. Another common reaction by staff is to isolate the dient dem on-
strating sexual misbehaviors from the other sex. Again, the sexual misbehavior
decreases, but the dient has not leamed the correct way to respond. For
example, consider an adult brain-injured male who approached women by
making comments about their bodies and touching them. Staff showed dis-
approval and isolated hirn from females. Although a decrease in misbehavior
was noted, the dient was not taught to interact with women. In a dating skills
group, he was taught to state his name and offer ahandshake. Staff reported
144
CHAPTER 7
a further decrease in sexual misbehaviors and increased interaction with
females.
It is important to follow dating skills training conducted in the dassroom
with in vivo sessions in the natural environment. This will promote general-
ization of skills learned. If possible, skills taught in vivo should be at a lower
level than those taught in dass, e.g., asking a girl out for a date on the phone
in vivo could be practiced while teaching conversing with a woman at dinner
in dass. It also is important to teach dients to expect and handle rejection
both in dass and in vivo.
Scheduled Feedback
Scheduled feedback refers to providing written and verbal feedback on
a scheduled basis. Frequency of feedback varies from every 15 minutes to
once a week. In determining a schedule, the current frequency ofthe behavior
must be established. The more frequent the behavior, the more frequent is
the feedback. If sexual misbehaviors are occurring 5-10 times an hour, then
feedback may be given every 30 minutes. On the other hand, ifthe misbehavior
occurs 5-10 times a day, then one or two feedback sessions a day may be
adequate. Feedback should start on a frequent basis and, as success is attained,
slowly decrease in frequency. Three components should be induded: First, a
written format for providing feedback must be selected. This can be a three-
ring binder or a data sheet listing the target behavior and divided into specific
time frames. Second, a scoring code must be developed and taught to the
dient. The scoring code must be specific to the behaviors. One effective, easy
scoring code is to use the letter "A" for appropriate interactions and the letter
"I" for inappropriate behavior. When giving feedback, examples of the ap-
propriate interactions would be provided as weIl as misbehaviors (e.g., "John,
I scored an "I" this time period because you touched Sally when she walked
by you"). Figure 7.11 shows a data sheet using the "A" and "I" code hourly.
Finally, feedback should always begin with a positive statement. That is, state
at least one good thing the dient did since the last feedback session. The
therapist would then present the dient with scored data sheet and explain it.
Zencius, Wesolowski, Burke, and Hough (1990) used scheduled feedback
to decrease touching in a 19-year-old female. During baseline, she touched
males on about 55% of an half-hour intervals. The behavior induded touching
genitals, kissing, and inviting males to touch her breasts and genitals. The
behavior was problematic because it occurred in the living room and in com-
munityestablishments. Subsequent to 7 days ofbaseline, half-hour feedback
was conducted for 25 days. At this point, nearly 100% of the intervals were
appropriate interactions with males (see Figure 7.12). Feedback then was
changed to one evening session concerning interactions occurring during that
PROCEDURES FOR BE HA VIOR PROBLEMS 145
INDIVIDUAL FEEDBACK SHEET
TIME SUN MON TUES WEDN THUR FRI SAT
7:00am
8:00am
9:00am
10:00am
11:00am
1200N
1:00pm
2:00pm
3:00pm
4:00pm
5:00pm
6:00pm
7:00pm
8:00pm
9:00pm
FIGURE 7./1. A data sheet for recording occurrence or nonoccurrence of sexual behavior on
an hourly basis.
day. This was done for 12 days. Following this, feedback was delivered on a
biweekly basis to promote maintenance of treatment effects (feedback was
given regarding the previous 2-week period).
Transfer of Stimulus Contral
Transfer of stimulus control refers to controlling misbehavior by providing
conditions where it is deemed appropriate. Certain behaviors are socially ac-
ceptable under certain conditions. For example, it is appropriate to be sexually
146
VJ
105
:::E 100
:
:
o 75
<t 70
ffi 65
Z 50
55
S 50
:
<t 25
BASELINE
CHAPTER 7
HALF-HOUR FEEDBACK
EVENNQ FEEDBACK
I :
20
15
<t 10
!z 5
0
DAYS
FIGURE 7.12. The effects ofhalf-hour and evening feedback to decrease inappropriate interaction
with males.
intimate in private places but not in public. In Zencius et al. (1990c), a 24-
year-old male gave females unwanted back massages. The dient was informed
that back massages were acceptable; however, they had to occur only in proper
places. The dient was allowed to give back massages to dients and staffmem-
bers during a 30-minute daily yoga dass. Figure 7.13 shows a 50% reduction
in inappropriate touching after allowing hirn to give back rubs during yoga
dasses. In this case, the dient learned to discriminate among environments.
Se/f M onitoring
Self-monitoring teaches individuals to record their own behavior. This
could indude sexual interactions, urges and feelings, fantasies, and conver-
sations with members of the opposite sex. For example, a dient is taught to
record all of his conversations with females hourly. That is, every hour, he
makes a notation as to who he talked to, what they talked about, how he feIt,
and how he handled the situation. Self-monitoring is done when the dient
has the urge to act out sexually, providing impulse control. It also can be used
on a schedule (e.g., the dient self-records every 30 minutes). For example,
the dient may be taught to use a data sheet specifying sexual behaviors to be
monitored (e.g., talking to a female, touching a female, sexual comments
made to females).
Three components should be induded. First, the therapist should identify
the behaviors to be self-monitored. For example, if one ofthe target behaviors
PROCEDURES FOR BEHA VIOR PROBLEMS 147
BASEI..INE BACK-fllllS l.M)ER STIMIJ..US CONTROl COI'l:lITlONS
o
'0
20 30
DAYS
FIGURE 7./3. The effects of transferring stimulus control to decrease inappropriate touching.
were sexual touching, then examples of what appropriate touching is and is
not should be provided. Second, the therapist should model how to use the
recording system. Third, the therapist must review all entries with the client
on a daily or weekly basis. One disadvantage of self-monitoring is that often
the client records only situations that were handled well. By frequent review,
the therapist can provide feedback regarding accuracy.
Self-monitoring should be used in conjunction with dating skins training.
Sessions can be followed by homework assignments tailored to the client's
needs. If she is working on initiating conversations, then homework assign-
ments could entail having her self-monitor an conversations initiated.
Zencius et al. (1990) used self-monitoring to treat a 32-year-old male
referred for exhibitionism. It was an episode of exposing himself that led to
his arrest. During the first week at the facility, the client exposed himself
twice. Following an intake interview, self-monitoring and dating skins training
(both in class and in vivo) began. After discontinuing treatment for 18 months,
only one episode of exhibitionism occurred. At this point, the client was
dating a female who also resided at the facility. Figure 7.14 shows the effect
of treatment on exhibitionism. A 4-year follow-up revealed no occurrences
of exhibitionism.
Behavior Contracting
As discussed under the noncompliance section, behavior contracts are
written agreements between the brain-injured individual and a family or
148
BASE
3 ,.-
TREATMENT PACKAGE
CHAPTER 7
FOllOW-UP
, 2 3 4 11 e 7 8 g 10 11 12 13 14 15 1e 17 18 1D 20
WEEKS
FIGURE 7.14. The elfect ofthe treatment for exhibitionism.
staffmember. Behavior contracts specify the target behaviors and a criterion
for meeting the contract. Areward for meeting the contract is dearly out-
lined. For inappropriate sexual behaviors, the contract specifies what ap-
propriate behaviors are to occur and what inappropriate sexual behaviors
are not to occur to comply with the contract. Before initiating a behavior
contract, the frequency of the inappropriate sexual behavior must be es-
tablished. Comparisons then can be made contrasting baseline and the
behavior contract intervention. Also, once a baseline is established, a cri-
terion for reduction can be established. If the frequency of inappropriate
sexual behavior is 20 times a week, for example, the criterion for meeting
the first contract would be slightly lower than this (e.g., 16, 17, or 18).
Once the first contract has been met by the dient, a second contract can
be initiated. The criterion for the second contract would be a little more
stringent than the first (e.g., 14 or 15 occurrences ofthe target behavior or
less would meet the contract).
Illustrative of using behavior contracting, Wesolowski and Zencius (1993)
used behavior contracting and scheduled feedback to decrease inappropriate
touching with two brain-injured females. In both cases, feedback was used
initially to decrease inappropriate touching. Next, behavior contracts were
negotiated along with the scheduled feedback procedure to further decrease
inappropriate touching. This resulted in near zero occurrences of inappropriate
touching in both cases (Figures 7.15 and 7.16).
PROCEDURES FOR BEHA VIOR PROBLEMS
BS Feedback BS Feedback
Ol
..c.
u
::J
Q)
iii
e
a.
a.
m
c
>-
u
c
Q)
::J
0"
u.. o 10 20
BS
30
FeedbacK ano
Contracting
40
Weeks ----.
149
50
FlGU RE 7.15. The elfects of scheduled feedback and behavior contracting to reduce inappropriate
touching.
INTERPERSONAL SKILL DEFICITS
Interpersonal skill changes occur in approximately 60-72% of individuals
with brain injury (Brooks & McKinlay, 1983; Jennett, Snoek, Bond, & Brooks,
1981). Crossen (1987) attributes this change in interpersonal skills to neurologie
injury, emotional reaction to injury, premorbid personality, or some com-
bination ofthese. In addition, Wesolowski (1987) dearly demonstrated that
social networks of disabled individuals get smaller as the person ages. Re-
gardless ofthe cause, it is important to treat interpersonal skill deficits because
ofthe variety of domains where they are used. Interpersonal skills are required
in relationships, domestic living situations, employment, and recreational
pursuits.
Before initiating treatment for interpersonal skill deficits, some assessment
should be done. McFall (1982) lists four commonly used assessment strategies
to measure interpersonal skill deficits. (1) Paper-and-pencil tests in which the
evaluator asks various questions from rating scales and checklists, and the
dient provides short answers or "yes" and "no" responses. Some rating scales
ask questions regarding specific social skills such as maintains eye contact,
shakes hand when offered, says "Thank you" when given something. Other
scales are less specific and ask questions pertaining to concepts, e.g., problem-
C
l
c
:
:
c
(
)
:
:
>
C
I
>
i
i
i
"
[
e
a
.
a
.
I
c
:
>
.
(
)
c
:
C
I
>
:
l
C
'
"
L
L
1
5
B
a
s
e
F
e
e
d
b
a
c
k
B
a
s
e
B
e
h
a
v
i
o
r
C
o
n
t
r
a
c
t
i
n
g
1
0
5
1
o
I
"
.
.
I
,
W
o
l
Q
2
0
3
0
d
O
W
e
e
k
s
"
"
"
-
-
F
I
G
U
R
E
7
.
1
6
.
T
h
e
e
f
f
e
c
t
s
o
f
s
c
h
e
d
u
l
e
d
f
e
e
d
b
a
c
k
a
n
d
b
e
h
a
v
i
o
r
c
o
n
t
r
a
c
t
i
n
g
t
o
r
e
d
u
c
e
i
n
a
p
p
r
o
p
r
i
a
t
e
t
o
u
c
h
i
n
g
.
.
.
.
.
.
.
U
l
o
(
)
:
:
z
:
:
;
J
>
t
T
l
i
t
I
-
.
J
PROCEDURES FOR BEHA VIOR PROBLEMS 151
solving skills, social competency. The main advantage of these scales is con-
venience. The results can be compared with what family or staff members
report. The disadvantage is that they are self-report measures, and the brain-
injured individual may not report accurately. This is especially true of dients
who cannot remember or have limited self-awareness of their deficits. (2)
Behavior role-playing tests use simulated samples or situations where various
skills are assessed. For example, if the evaluator is interested in assessing
accepting criticism, following instructions, or handling a problematic situation,
he or she would set up these situations. The major advantage of role-playing
tests is that the evaluator can assess specific skills and can vary the assessment
from one individual to another. One disadvantage of this procedure is that
the situations are done in a simulated and controlled environment. When
using role-playing, one should make the environment as natural as possible.
(3) Observe subjects in semistructured, quasinatural environments. Obser-
vations are done in environments where various social skills can be seen.
Confederates often are used to interact with the subjects. (4) Interviewing
parents, spouse, other family members, co-workers, staff, and friends regarding
the interpersonal skill problems of the dient can be useful. Questions can be
open, such as asking how the dient interacts with others. Or they can be
specific: "00 they maintain eye contact?" "00 they say 'Please'?" This measure
is best used in conjunction with the dient's self-report; the two then can be
compared to arrive at a discrepancy score.
A final assessment procedure we recommend is to perform a functional
analysis of the targeted social skill deficits. As outlined in Chapter 2, the
accompanying antecedents and consequences of the behavior are observed
and documented. If the targeted social skill was accepting criticism, then
every time the dient was given criticism, the antecedents and consequences
of providing criticism would be noted. For example, the antecedents to the
criticism being given induded: the time was 1 :00 PM, it occurred in the vo-
cational training site, the dient was painting. The criticism was given by her
immediate supervisor. As a consequence ofbeing criticized, the dient shouted
at her supervisor and left the work area. She returned 1 hour later. This is a
sequence analysis and is the first step in conducting a functional analysis,
which also consists of collecting data on the target behavior under various
antecedent conditions. By completing a functional analysis, valuable infor-
mation regarding frequency and duration of occurrence, when and where the
behavior occurs, and under what stimulus conditions the behavior occurs can
be expected.
Social Skills Training
Traditional social skills training (Hopewell, Burke, Wesolowski, & Zaw-
locki, 1990) usually occurs in small groups (e.g., two to five dients). Sessions
152 CHAPTER 7
begin with the therapist introducing the social skill and providing a rationale
as to its importance. The therapist then lists the necessary steps of the skill.
If the skill were following instructions, the therapist would say, "Today, we
are going to practice following instructions. It is important to follow instruc-
tions from staff and supervisors so that we get along better with others. Fol-
lowing instructions consists of the following four steps:
1. Maintaining eye contact with the person giving you instructions
2. Acknowledging that you understand the instructions
3. Performing the instructions
4. Checking back with the person who gave you the instructions."
The therapist would then model following instructions. She would do
this by having a dient or a cotherapist play the role of a supervisor and model
the steps in following instructions. The fourth step is to engage a dient in
role-playing where he would have to follow instructions. Finally, the therapist
and dients would provide feedback as to how he followed instructions. Feed-
back would be specific to the components of the skill. For example, if the
dient followed instructions but did not maintain eye contact, this would be
mentioned to hirn. With all feedback, the therapist would first point out things
the dient did well.
This four-step method is continued until all dients have the opportunity
to practice it. Some criterion is usually established specifying the number of
times a dient has to correctly role-play a social skill. Appendix D is a repre-
sentative list of 20 commonly used social skills.
The most common method of keeping data on social skills is to use a
task analysis listing the necessary steps to perform the social skill. The therapist
observes the role-play and simultaneously scores the component on the task
analysis. This can be done by using "+" to show the component was performed
correctlyand "-" to indicate an error. Accepting "No" for an answer, for
example, is divided into the following tasks: (a) Maintain eye contact; (b)
acknowledge what the personsays, and say "OK"; (c) don't argue, whine, or
pout; and (d) ifyou don't understand why the person said "no," then calmly
ask for a reason. In this example, if the dient performed all steps correctly, a
"+" mark would be recorded for each step on the task analysis. For any
errors, a "-" mark would indicate that a step was incorrect or was not at-
tempted. One major concern of using social skills training is generalization
of the skills outside the dassroom.
Point Systems
Point systems are valuable when more than one social skill has been
targeted for change. These can indude both prosocial and maladaptive social
PROCEDURES FOR BEHA VIOR PROBLEMS 153
behaviors. Onee speeifie behaviors have been seleeted, point values are as-
signed. More important behaviors are assigned higher values. For example,
giving eompliments and saying "Thank you" may get 2 points whereas fol-
lowing instruetions may earn 10 points. A menu of reinforeers should be
seleeted and eosts of these items or aetivities are assigned. Items or aetivities
that are more reinforcing should be more expensive. For example, a trip to
the mall or a movie may cost 200 points. Other back up reinforeers such as
free time, phone calls, and money may cost 50 points. When selecting rein-
forcers, ask clients what they like or observe what they do in their free time.
TARGET SOCIAL OEHAVIORS
Accepting criticism at work station ..... .
Volunteering to help others ....
Requesting permission from staff.. ...
SolvinQ problems ...
Following instructions from staff... ...
Giving compliments to others ...
Sweari ng at others ..
Teasing others ...
...... 10 poi nts eoch ti me.
. .... 5 points each time.
. ... 5 points each time.
. ...... 15 points each time.
. ..... 10 points each time.
. ....... 5 points each time.
. ... 10 point loss.
. ...... 5 point loss.
MENU OF REINFORCERS
Trip to the mall..
Lunch out ..
Extra break time ....
Addi ti onal phone call ..
First choice of video .. .
Additional TV time .... .
Choice of evening activity
Pool room ...
Walk around campus ....
Use facility headphones.
Go out for i ce cream ...
Trip to the music store ....
...... 200 points.
..... 150 points
. .......... 30 points.
. ........... 35 points.
. ............ 50 poi nts.
. ........... 20 pOints/hour.
. .......... ..40 points.
.............. 50 pOints/hour
. .... 30 points.
. ........... 30 poi nts.
.80 points.
. .. 100 points.
FICURE 7.17. A sampie of social behaviors, point values for these behaviors, and a menu of
reinforcers.
154 CHAPTER 7
Figure 7.17 presents a sampie of social behaviors, point values for these be-
haviors, and a menu of reinforcers.
Illustrative of decreasing maladaptive social behaviors, Burke and Lewis
(1986) used a point system to decrease three maladaptive behaviors in a 21-
year-old male. The three maladaptive social behaviors were loud outbursts,
interrupting others, and nonsensical talk. Points could be earned in five 4-
minute intervals during lunch for nonoccurrence ofthe three behaviors. Fol-
lowing lunch, the dient could redeem points for items on a reinforcement
menu. These induded a 7-minute walk with staff, soft drinks, candy bars,
magazines, and free time to listen to music.
Contingent and Scheduled Feedback
Feedback can be provided on a scheduled basis. That is, after a prede-
termined time, feedback is given to the dient regarding the target behavior.
If the target behavior is complimenting others and saying "Thank you," then
feedback would be provided regarding the number of times she engaged in
these social skills. The frequency of feedback is usually determined by the
frequency of the behavior. The more frequent the behavior, the more frequent
is the feedback. For example, ifthe target behavior is name calling and occurs
only twice a day, feedback would need to be given only once or twice a day.
If name calling occurred several times an hour, then feedback may occur as
frequently as every hour.
One important consideration when using feedback is to target prosocial
behaviors. Too frequently, maladaptive social behaviors are targeted for re-
duction but no effort is made to increase prosocial behaviors. It is important
to increase prosocial behaviors when decreasing maladaptive social behaviors
for two reasons: to teach an alternative way to respond, and to set the occasion
fr the dient to be reinfreed.
In Zencius and Wesolowski (1991), two brain-injured dients at a reha-
bilitation facility were viewed as having poor social skills by staff, family, and
peers. Rather than decreasing maladaptive social behaviors, the foeus was on
teaching prosocial behaviors. These prosocial behaviors were volunteering to
help others, expressing appreciation, and extending compliments. Treatment
initially consisted of training these three social skills in a small group setting.
Within 1 week, both dients could use the three targeted social skills with
100% accuracy within the group; however, no increase was noted outside the
group. Both dients, therefore, received one session of feedback at the end of
the seeond shift (7:00 PM), consisting of showing the dients their data for that
day. The codes "V" indieated volunteering, "T" indicated expressing appre-
ciation (thank you), and "e" indicated the dient extended a eompliment.
Figures 7.18 and 7.19 show the frequency of these behaviors during baseline,
PROCEDURES FOR BEHA VIOR PROBLEMS
5
4
Vl 3
C
Q)
Ci 2
E
o
c
.Q
Cii
'0
a.
a.
Cl
c
'00
Vl
a.
x
W
Cl
C
Q)
C
::J
g
5
Probe Data BS S. S. Probe Feedback Sessions
o 10 20 30
o 10 20 30
Days of Data Collection and Training
155
40
40
FIGURE 7.18. The effects of scheduled feedback on increasing the use of prosocial behaviors
of volunteering, expressing appreciation, and extending compliments.
Probe Data BS S. S. Probe Feedback Sessions
8
(/)
c
(IJ
4
E
0..
E
0
2
0
0 10 20 30 40
8
c:
b
.Q
iii
.(3
(IJ
Ci
4
Cl.
<{
Cl
c:
w
2
(/)
(IJ
Ci
x
W
0
0 10 20 30 40
b
5
4
Cl
c
C
3
(IJ
(IJ
C
:::l
2
g
o 10 20 30
40
Days of Data Collection and Training
F1GURE 7.19. The effects ofscheduled feedback on increasing the use ofprosocial behaviors
of volunteering, expressing appreciation, and extending compliments.
PROCEDURES FOR BEHA VIOR PROBLEMS 157
social skills training, and feedback. Results show that only after scheduled
feedback was initiated did the frequency ofthe three target social ski1\s increase.
Contingent feedback occurs immediately after the behavior is observed.
Ifthe social behavior being observed is following instructions, then the dient
receives feedback every time he or she receives instructions. Feedback would
be provided when instructions were fo1\owed correctly and incorrectly. Again,
with all feedback, the caregiver providing the feedback always points out at
least one thing the dient did weil. The caregiver then comments on things
that could have been handled better. To i1\ustrate, a dient at a vocational
training site receives instructions to sweep out the tool room. The dient main-
tains eye contact with his supervisor, acknowledges the instructions, and then
goes outside and has a cigarette. In this case, contingent feedback would be
"Y ou did a great job maintaining eye contact and listening to me, but now
you need to sweep out the tool room." The major advantage ofusing contin-
gent feedback is that it can be provided anytime in the natural environment.
For example, if the targeted behavior is observed at the grocery store, then
this is where the feedback occurs. Contingent feedback also fosters general-
ization, wh ich is enhanced by providing feedback consistently across various
environments, different situations, and with different people. A concern with
using contingent feedback is that a1\ caregivers must respond consistently.
Illustrative of using contingent feedback is an ex am pIe of a young brain-
injured male who would hug any female upon meeting them. The dient was
then informed that this often made people fee! uncomfortable and that the
appropriate way to introduce oneself was by offering ahandshake. After this
explanation, contingent feedback was provided to the dient by all female staff
who interacted with him regarding meeting people.
Preteaching
Preteaching refers to teaching the expected behavior prior to entering a
situation where the skill will be required. To illustrate, an individual has
difficulty accepting criticism from the vocational trainer. Using preteaching,
training would begin by practicing giving the dient criticism in a contro1\ed
environment (e.g., in a therapy room, away from the vocational training site).
A therapist who works weil with the dient would begin giving criticism. Ini-
tially, the therapist would prepare the dient with "OK, I'm now going to
practice giving you criticism." Once the dient can accept criticism under
these conditions with one trainer, other people begin to give the dient criticism
in different settings. When the dient can accept criticism in various conditions
and with different people, criticism is introduced in the environment where
it was viewed as problematic. When using preteaching, several training sessions
158 CHAPTER 7
should occur throughout the day to enable the dient to practice the skill. We
recommend at least three to five practice sessions each day.
Group Psychotherapy
Crossen (1987) cites group psychotherapy as useful for dealing with emo-
tional reactions to injury. Specific techniques used in group settings that ad-
dress social behaviors indude direct confrontation and expression of anger.
If confronted by a therapist and peers in a group setting, the dient will more
likely accept feedback. It is important not to confront in a threatening, chal-
lenging fashion but in a neutral, calm fashion.
Another tactic recommended by Crossen (1987) is to encourage dients
to express anger in groups. The rationale is that anger may not be directed at
those outside the group. For example, a dient who becomes angered quickly
and engages in profanities may be better handled in a group setting versus
outside the group. To benefit from group psychotherapy, Crossen (1987) states
that candidates must possess some memory and reasoning skills.
IMPULSIVITY
Survivors of traumatic brain injury frequently demonstrate impulsive
behaviors. That is, they act before they think. Professionals often attribute
impulsivity to frontal lobe damage. More specifically, Stuss and Benson (1984)
note that injuries to orbitofrontal undersurfaces are associated with uninhibited
and impulsive behavior. Although impulsive behaviors are not always apparent
through casual observations, impulsivity can be easily detected in structured
settings such as dassrooms, workshops, and small groups. Impulsivity can
interfere with one's ability to function in social relationships, perform activities
of daily living, participate in vocational and avocational situations, and per-
form independent domestic functions.
Thompson (1974) interviewed families and found that impulsive and
restless behaviors were most problematic for families to cope with. Further,
Luria (1973) notes that of all head injuries, those associated with significant
frontal lobe damage have the poorest prognosis for successful return to work
and family. In this section, treatment strategies focusing on impulsivity will
be discussed.
Treatment o/Impulsivity
Checklists
Checklists can be used to replace verbal instructions and sequence items
that need to be completed. The focus of using checklists is to replace verbal
PROCEDURES FOR BEHA VIOR PROBLEMS 159
instructions or requests with written instructions. Some brain-injured indi-
viduals are so impulsive that they engage in tasks or activities prior to receiving
complete instructions or considering a plan of action. For example, a typical
response to a problematic social situation is to yell and scream at another
person rather than considering other solutions. Recently, Burke, Zencius,
Wesolowski, and Doubleday (1991) used a written checklist to replace verbal
instructions at a vocational training site. Initially, the dient would begin
working on tasks before he received complete instructions from his vocational
supervisor. This resulted in completing the majority of tasks incorrectly and
subsequently leaving the workshop because he became agitated and frustrated.
Treatment consisted of handing the dient a checklist (task analysis) of the
task to be completed, discontinuing verbal instructions. Each task was divided
into four distinct steps for all three routine tasks he completed daily. The
three tasks were sweeping, cutting lumber, and planing lumber. Initiation of
the checklist resulted in completion of nearly 100% of all three tasks.
Several variables must be considered when using checklists to alter im-
pulsivity. First, the trainer must maintain the individual's attention long
enough to explain the rationale for using the checklist. This can be done by
training in an environment with low stimulation and keeping training sessions
brief. Second, the trainer must model how to use the checklist. Third, the
dient must experience success using the checklist in natural situations. This
can be accomplished by having the dient use the checklist in situations where
he or she is most likely to succeed and failure is improbable. For example, a
checklist could be initiated to complete a two-step task. Once success is ob-
tained on this task, then achecklist could be extended to a four-step task.
This sequence could be continued until the dient is using checklists for a
wide variety of tasks in different situations.
Feedback
In addition to using feedback for treating maladaptive sexual and social
behaviors, feedback can be used to provide speciflc information to brain-
injured individuals regarding impulsive behaviors. lt is recommended that
scheduled feedback be used versus contingent feedback. That is, feedback
occurs on a regular time schedule as often as every ho ur to as infrequently as
once a week. The schedule of delivery is dependent on the frequency of the
behavior (i.e., the more frequent the behavior, the more frequently feedback
should be provided). The rationale for using scheduled feedback is that when
a brain-injured individual is engaged in an impulsive behavior, he or she is
less likely to accept feedback when the behavior occurs. For example, an
individual may become more agitated and less likely to listen when another
160 CHAPTER 7
person provides feedback when they are agitated. Ifthe feedback is given 10
minutes later, however, the dient is more likely to accept it.
Several components must be induded when providing feedback. (1) The
trainer always begins with a positive statement. That is, the trainer should
inform elients ofat least one thing they did weH, e.g., "You used goodjudgment
by coming to stafffor help." (2) Pinpoint and define specifically what impulsive
behavior they demonstrated, e.g., "Y ou left the work site without permission
when you became angry." "As an alternative to leaving, you could have asked
permission to leave from your supervisor." (3) Combine verbal feedback with
written feedback. Written feedback can be provided in the form of either an
individualized data sheet or an A-B-C data sheet (see Chapter 2). One ad-
vantage of using an A-B-C sheet is that specific impulsive behaviors can be
described and later shown to the dient. Also, more information about the
impulsive behavior can be determined using A-B-C data sheets. An individ-
ualized data sheet should be used when antecedents and consequences ofthe
impulsive behavior have been established. Illustrative ofusing feedback, a 12-
year-old male participating in an academic program at arehabilitation facility
completed the majority of his dassroom assignments rapidly. This resulted
in nearly all assignments being completed incorrectly. The instructor reported
that he would complete questions before reading the entire question. Feedback
consisted of having the dient perform 5 problems and then notifying the
instructor. Only 5 problems were presented to the dient at one time, although
a total of20-30 problems would be attempted by the end ofthe session. The
instructor would correct his work by placing a "+" mark to indicate correct
responses and would cirele questions responded to incorrectly. This procedure
increased correct responding by more than 50%.
Se/f Recording
In the simplest form, self-recording can consist of making daily journal
entries. At a more sophisticated level, self-recording can occur on a regularly
scheduled basis using a formalized data sheet. When impulsive behaviors
occur in only one environment or in one situation, implementation of self-
recording is fairly simple. For example, if an impulsive behavior only occurs
at a vocational training site, then self-recording would only occur in this
environment. The dient may score yes or no on a data sheet if he or she
demonstrated any impulsive behaviors. As with feedback, self-recording can
occur on a regular time schedule or on a contingent basis. With the scheduled
recording strategy, the elient records if he or she was impulsive during a
specified time interval, e.g., every 15 or 30 minutes. With contingent self-
recording, the dient self-records every occurrence of the target behavior. The
obvious disadvantage of using self-recording is that dients often have a ten-
PROCEDURES FOR BEHA VIOR PROBLEMS 161
dency to score their behaviors more favorably than others. This can be ad-
dressed by having a staffmember collect data on the same impulsive behaviors.
This can be illustrated in the following example. A 26-year-old male at a
rehabilitation center would continuously ask repetitive, irrelevant questions
regarding tool location while in the vocational training site. Although the
dient could show and verbalize to others where all tools were, he impulsively
asked his supervisor where they were kept every time he needed to locate a
too1. Intervention consisted ofhaving the dient self-record all irrelevant ques-
tions on a contingent basis. That is, every time he asked his supervisor where
tools were located, he was required to record this on a data sheet located on
the wall over his workstation. To determine the reliability of self-recording,
the supervisor simultaneously recorded all irrelevant questions. When they
compared data sheets, a large discrepancy was noted, i.e., the dient under-
scored the actual number of irrelevant questions asked. The supervisor then
cued the dient every time he observed an irrelevant question regarding tool
location. After 2 weeks of this procedure, the dient began to record irrelevant
questions accurately. When providing cues to the dient, the supervisor was
positive and provided praise when the dient self-recorded irrelevant questions.
When using self-recording, a staff member also should collect data on the
frequency of the target behavior as in this illustration.
Self-recording procedures are most useful when staff want dients to be-
co me more aware oftheir behavior. If dients become aware ofbehaviors they
are demonstrating, then a decrease often will occur. Self-recording is effective
when the number of permanent products produced is a concern. The dient
can record the number of products produced hourly or daily and assess im-
provements or change.
Self-recording also is useful in social interactions. The individual can
record the number of interactions, who the interaction occurred with, and
the type and quality ofinteraction. Self-recording can be used in any situation
in wh ich the behavior can be easily quantified, i.e., number of interactions,
number of outbursts, number of work breaks taken, number of cigarettes
smoked. Another illustration of self-recording involved a 29-year-old female
who left her horticulture training program without authorization. Her voca-
tional trainer reported that she left the work site as many as 10-15 times
during a 3-hour workday. When confronted with the number of breaks she
took, she would become verbally and physically aggressive. Intervention con-
sisted of providing the dient with a dipboard and data sheet on wh ich she
self-recorded the number of breaks she took daily. No consequences were
given for leaving the work site; the vocational trainer simply reminded her
to self-record breaks. This procedure did not totally eliminate unauthorized
breaks, but resulted in a 50% reduction.
162 CHAPTER 7
Preteaching
As defined previously, preteaching consists ofteaching the alternative or
desired behavior outside of the situation where the behavior usually occurs.
Preteaching is recommended for teaching specific behaviors rather than general
responses that can be used in all situations. Preteaching can be effective for
teaching dients to respond to problematic situations in social situations. Also,
preteaching is effective in situations where a skill is required on a routine and
frequent basis. For example, preteaching may be used to teach an individual
who becomes impulsive to receive criticism and follow instructions in a vo-
cational setting.
The teaching methodology for preteaching was outlined earlier in this
chapter. Training sessions are initiated on a one-on-one basis with a therapist
in an artificial environment (dassroom or therapy room). Once success is
achieved under these circumstances, other individuals are programmed to
engage in preteaching interactions. Finally, teaching occurs in the natural
environment in which the impulsive behavior frequently occurs. For example,
if following instructions at a training site results in impulsive behaviors such
as leaving and aggression, then training initially would occur in another en-
vironment on a one-on-one basis. The dient would be given instructions to
follow. Finally, instructions would be given to the dient at the training site.
When giving instructions, the trainer would prepare the dient by verbalizing,
"I'm now going to give you instructions."
Illustrative ofthis, an 18-year-old male at apart-time vocational training
program would often leave the work area if he was given feedback and crit-
icism. Preteaching consisted of conducting three training sessions per day
held outside of the work site. He was given feedback and criticism during
these training sessions. The trainer always prepared the dient by informing
hirn that it was time to praetice receiving feedback and eritieism. Onee he
aecepted feedback and criticism without incident, feedback and criticisms
also were given by other individuals in other environments. Finally, feedback
and criticism were provided at the vocational training site. Throughout train-
ing, staff always told the dient when they were about to provide feedback or
criticism.
When individuals demonstrate impulsivity in a wide range of situations
and environments, it is recommended that the trainer prioritize which im-
pulsive behaviors are most in need of intervention. A prioritization matrix
can be used to determine which impulsive behaviors are most debilitating
and, therefore, in need of immediate training. In other words, one might
assign weights to three characteristies ofthe behaviors induding frequency of
the behavior, how problematic the behavior is, and how long-standing the
behavior iso
PROCEDURES FOR BEHA VIOR PROBLEMS 163
Minitraining Sessions
Minitraining sessions consist of providing training for short periods of
time interrupted by frequent breaks during which the client is encouraged to
leave the immediate environment and then return. Rather than providing
therapy in traditional 45 to 50-minute blocks, training or evaluations occur
in 10- to 15-minute segments. When away from the training session, the client
should be engaged in activities requiring movement. We have observed that
adolescent clients are less physically active and impulsive during training
sessions if they engage in movement exercises between breaks. For example,
in a workshop setting using mini training sessions, the client would work for
only 10 minutes and be expected to complete only live products. By providing
sm aller units of work or training time, the client is more likely to succeed
because the demands are limited. Once success is achieved, a gradually in-
creased work load is presented. In a classroom setting, rather than presenting
60 math problems to be completed in one session, the client may begin with
having to complete only 5 problems and then leave the area.
In essence, the amount of work or instructional time is shaped. That is,
closer approximations of the desired behavior are achieved and reinforced
while prior approximations are extinguished (not reinforced). The most im-
portant consideration is that the initial level is easily attainable.
An example of using the minitraining sessions involves three clients
working in an auto shop program who often left their work area or would
begin participating in a new task before completing the present task. This was
resolved by placing the clients on a minibreak system. That is, clients received
a break every hour rather than one lunch break and two 15-minute breaks.
During breaks, the clients were encouraged to leave the area and return when
the break was over. This resulted in a decrease in unauthorized breaks. Mini-
training sessions are recommended when teaching academics, functional skills,
vocational skills, and when conducting intake evaluations.
SUMMARY
Behavior Problems
1. The following are common behavioral sequelae of head injury: ir-
ritability, impulsivity, egocentricity, impaired judgment, noncom-
pliance, dependency, apathy, tension, sexual disinhibition, and verbal
and physical aggression.
2. Behavior problems have been treated effectively with applied behavior
analysis techniques.
164
CHAPTER 7
Noncompliance
3. Noncompliance can be defined as refusal to participate with reha-
bilitation services, outpatient services, family expectations, and social
roles and regulations.
4. Positive reinforcement, negative reinforcement, age, cultural differ-
ences, memory deficits, rigidity of programming, and neglect of in-
dividual needs and interests all can contribute to noncompliance.
5. Treatment strategies demonstrated to be effective in dealing with
noncompliance have included individual point systems, group point
systems, leveled programs, behavior contracts, and the Premack
Principle.
6. A behavior contract delineates an agreement between a client and a
family or staffmember. The noncompliant behavior is clearly defined
and areward for meeting the contract is also clearly outlined.
7. Antecedent control techniques refer to setting the occasion for the
targeted behavior to occur. Antecedent control techniques should
be considered when severe memory deficits are apparent and con-
sequence management techniques have failed in changing the non-
compliant behavior.
8. Frequently used antecedent control techniques include maps, verbal
prompts, physically changing the environment, and pictures.
Aggression
9. Common reasons for aggression include learning history, aversive
treatment, pain, changes in reinforcement, episodic dyscontrol syn-
drome, and skill deficits.
10. When using contingency management techniques, the nonoccurrence
of aggression or decreased levels of aggression result in reinforcement.
11. Teaching alternative behaviors refers to teaching the client how to
engage in behaviors opposite to aggression which produce reinforcing
consequences.
12. Once an alternative behavior to aggression has been trained, the
client should be given opportunities to practice the new behavior
and experience reinforcing consequences.
13. Redirection refers to redirecting the client to any new stimulus not
associated with the provoking situation. With specific redirection, a
predetermined script is used to redirect the client from the provoking
situation.
14. Stress management training usually consists of two distinct com-
ponents including recognition of early signs of stress and agitation
and initiation of some type of relaxation technique.
PROCEDURES FOR BEHA VIOR PROBLEMS 165
Sexual Dysfunction
15. Sexual dysfunction is common following TBI. Interestingly, the ma-
jority of sexuality problems have been with hyposexuality rather
than hypersexuality.
16. Dating skills training consists ofteaching individuals sodally appro-
priate ways of interacting with members of the opposite sex.
17. Scheduled feedback refers to providing written and verbal feedback
on a scheduled basis regarding the individual's interactions with
members of the opposite sex.
18. With behavior contracting, the inappropriate sexual behavior is tar-
geted for reduction. Decreased levels of inappropriate sexual behavior
result in the contract being met.
19. Transfer of stimulus control refers to controlling the inappropriate
sexual behavior by providing stimulus conditions where the behavior
is deemed appropriate.
20. Self-monitoring consists ofhaving the individual monitor and record
sexual behaviors he or she engages in. This can indude verbal be-
havior, thoughts, and actual behaviors.
21. Components of a specialized treatment package for exhibitionism
indude a detailed interview of the dient, self-monitoring, dating
skills training, impulse control delay techniques, and supervised in
vivo training.
Interpersonal Skill Deficits
22. Social skills training begins with a rationale of the skill to be trained
and is followed by a modeled demonstration by the trainer. Next,
the dient engages in role-play situations with the trainer and other
group members. Lastly, the trainer provides feedback to the dient
regarding behaviors demonstrated in role-play situations.
23. Motivational techniques can be used to reinforce appropriate social
behaviors and decreased levels of inappropriate sodal behaviors.
24. Feedback can be provided on a contingent basis or a scheduled basis
regarding occurrences of social behaviors.
25. Preteaching consists ofteaching the expected behavior prior to getting
into a situation where the target behavior will be required.
26. Group psychotherapy can be used to confront dients with social
behavior deficits in a supported environment.
Impulsivity
27. Impulsive behaviors are frequently demonstrated by traumatically
brain-injured individuals. This is often characterized by impulsive
and unplanned actions.
166 CHAPTER 7
28. The focus of checklists is to replace verbal directions with written
information.
29. When training individuals to use checklists, the trainer must maintain
the dient's attention long enough to explain the rationale and model
its use. The trainer must also ensure the dient experiences success
using the checklist.
30. When providing feedback, it is recommended that scheduled feed-
back be used when treating impulsive behaviors.
31. The trainer provides feedback by beginning with a positive statement.
Subsequently, the dient is given specific information regarding his/
her impulsive behavior and is given an alternative appropriate re-
sponse. Finally, feedback should be provided in verbal and written
fashion.
32. Contingent self-recording consists of scoring every occurrence ofthe
impulsive behavior following its occurrence.
33. When self-recording occurs on a scheduled basis, the dient records
the occurrence or nonoccurrence of the behavior on a regular basis.
34. Preteaching is effective in those situations concerned with teaching
appropriate social responses and those that occur on a routine basis.
35. A prioritization matrix should be used when a wide variety of im-
pulsive behaviors are demonstrated by a brain-injured individual.
36. Minitraining consists of instructional time and encouraging move-
ment during breaks.
Procedures for Health and
Medical Problems
8
Behavioral medicine is a popular and rapidly growing field in applied behavior
analysis. Applications ofbehavioral principles to health and medical problems
indude eliminating headaches, controlling hypertension, weight reduction,
improving compliance to medical regimens, controlling epileptic seizures,
and reducing chronic pain, to name just a few. For a more complete discussion,
the interested reader is referred to Williams and Gentry (1977). In working
with brain-injured individuals, we have applied behavioral principles to prob-
lems in using assistive devices, operant seizures, bulimia, obesity, hypochon-
driacal statements, and diabetic dients manipulating staff through noncom-
pliance with their medical regimens.
USING ASSISTIVE DEVICES
Assistive devices used by survivors of brain injury often indude wheel-
chairs, walkers, quad canes, straight canes, heimets, and leg and arm braces.
On occasion, dients refuse to use these devices or become overly dependent
on them. For example, a young man at a rehabilitation center was supposed
to wear a heimet while walking because a portion ofthe skull had been resected.
The dient refused to wear the heimet because of its appearance and
inconvenience.
The individual who always uses a cane even though the physical therapist
has recommended walking without it is an example of someone who has
become overly dependent on a device. In this illustration, the dient may have
had negative experiences when trying to ambulate without the cane (e.g., the
person may have fallen, it takes too long to walk from one place to another
167
168 CHAPTER 8
without the eane, he or she had diffieulty ambulating over rough terrain).
Consequenee management and anteeedent control techniques ean be used to
improve these problems.
Consequence Management
Chapter 7 outlined various motivational teehniques for inereasing and
deereasing behaviors. These teehniques ean be used to both inerease eompli-
anee in using assistive deviees and deerease overdependenee on them. In the
illustration of a elient who would not wear a prescribed heImet, a point system,
behavior eontracting, or the use ofthe Premaek Principle eould be employed
to inerease heImet wearing. In this case, wearing the heImet would be reinforced
for a specified period eaeh day and specified number of days (e.g., the dient
must wear the heImet for at least 90 minutes a day for three eonseeutive days
to meet the eontract).
The same motivational systems ean be used to decrease dependency on
assistive deviees. For example, ifthe goal were to have the dient use a walker
more frequently and relyless on a motorized wheelchair, these behaviors
would be reinforeed. If a point system were used, then the elient would reeeive
points every time she was observed out of her wheelchair.
We used a reinforcement program to inerease a 44-year-old male dient's
use of a manual wheelchair instead of exdusively using a motorized wheelchair.
The team physica1 therapist reeommended that the elient use a manual wheel-
ehair to exercise his arms since he reeeived no formal physica1 therapy or
exercise programming. The first intervention eonsisted ofrewarding the dient
with an item from a menu of reinforeers on a daily basis ifhe used his manual
wheelchair during the morning hours. Items on the menu of reinforeers in-
duded one nonalcoholie beer, a sports magazine, ehewing gum, ehoeolate
bars, soda, and eigarette lighters. Prior to treatment, the elient used his manual
wheelchair less than once a week. This inereased to 4! days per week when
the reinforeement program was initiated. Subsequent to areversal, peer
prompting was added to the daily reinforcement, whieh resulted in the manual
ehair being used all of the time. Figure 8.1 shows the data for all eonditions.
Antecedent Control Techniques
Numerous applications of antecedent eontrol teehniques ean be effeetive
for dients who forget to use assistive deviees. For example, a dient at a re-
habilitation center frequently forgot to wear a hand splint preseribed by a
physician. An anteeedent intervention of placing the hand splint on achair
loeated in front of her bedroom door was initiated. This resulted in the dient
wearing the hand splint more often. Another example of using an anteeedent
PROCEDURES FOR HEALTH AND MEDICAL PROBLEMS 169
REINF and
aSE REINF aSE REINF Peer P.
Peer Prompting
6
(1l
Ol
I
5
Cf)
::::>
....
. iij
4
.r::
0
Qj
(1l
3 .r::
'0
2
>-
0
C
(1l
:J
0-
(1l
u:
0
0 10 20 30
TIme in Weeks
FlGURE 8.1. The effects ofreinforcement and peer prompting on the use ofa manual wheelchair.
intervention is the case of a dient who was prescribed a heImet when walking.
Although the dient agreed to wear the heImet, he often forgot to put it on.
The antecedent intervention of securing the heimet to the dient's waist with
astring was used. The heimet secured to the waist was a permanent visual
and physical cue to wear the heimet when ambulating.
Zencius, Wesolowski, Burke, and McQuade (1989) increased cane usage
in a dient with severe memory deficits. The dient frequently left her room
without bringing her cane. The team's physical therapist pointed out the ne-
cessity of using the cane when walking because she often fell down without
it. This was especially true when she walked more than 100 feet or across
uneven terrain. Techniques such as social praise for using her cane, male
escorts to her room to get her cane, and money all failed to increase ca ne
usage. An antecedent intervention called the "AM routine" greatly increased
cane usage. This consisted ofhanding the dient her cane following completion
of grooming skills as she left her room for breakfast. If she were handed her
cane at this time, she was likely to use it thc entire day. As shown in Figure
8.2, cane usage occurred more often when the antecedent intervention ofthe
"AM routine" was used than when several consequence management strategies
were tried.
OPERANT SEIZURES
perant behaviors are those that are affected by contingencies operating
on the environment. perant seizures, therefore, are phenomena that occur
170
w
Z
<t:
u
I
f-
VI
-..l
<t:
>
Q::
w
f-
Z
LI...
0
w
0
<t:
f-
Z
w
U
0::
w
D...
100
80
60
40
20
0
CHAPTER 8
A.M.
ROUTI E
BL
SOCIAL
PRAISE
5 10 15 20 25 30 35 40 45
DAYS
FIGURE 8.2. The effects of consequence management versus antecedent control in increasing
cane usage.
when dients get attention for having seizures or escape from or avoid certain
events because of their seizures. For example, a dient receiving outpatient
therapies often demonstrated seizures prior to leaving for therapy sessions.
The result was that the dient's mother canceled the therapy session. In this
example, seizures were being negatively reinforced (i.e., the individual avoids
therapy sessions by demonstrating seizures). In another example, a dient at
arehabilitation facility demonstrated daily seizures. As a result of having
seizures, the dient spent time in the nurse's office, and staff spent additional
time with her. In this example, seizures were positively reinforced (i.e., the
occurrence of seizures was maintained by contingent attention).
Extinction
Extinction is a procedure in which reinforcement of a previously rein-
forced behavior is discontinued. Behaviors put on extinction will eventually
disappear.
Illustrative of using extinction was ignoring the seizures of a 12-year-old
male dient. He displayed five to ten seizures per week. As a result of dem-
onstrating seizures, he was excused from therapy sessions and received atten-
tion from staff at the nurse's station. Treatment consisted of ignoring the
dient's seizures. Staffwere trained to break eye contact with the dient, leave
the immediate area, not to converse with the dient, and to engage in con-
PROCEDURES FOR HEAL TH AND MEDICAL PROBLEMS 171
versation with other staff or dients who were acting appropriately. When the
adolescent was not demonstrating a seizure, staff were to attend to hirn and
praise hirn for not having seizures. Characteristic of extinction procedures,
the seizures initially increased in frequency but then gradually decreased. An
important consideration when employing extinction is to ensure that all staff
and family members are aware of the program and conduct it consistently.
Motivational Techniques
Contracts and points can be used to reinforce the nonoccurrence of op-
erant seizures. Reinforcement is provided for a decreased rate or absence of
seizures. For example, ifweekly behavior contracts were used, the dient would
comply with the contract by reaching a criterion (e.g., the contract was met
if five or less seizures occurred during a week). Ideally, the contract then
becomes progressively more stringent. The next contract would specify that
four or less seizures could occur to meet the contract. If using point systems,
a certain number of points would be given to the dient for not demonstrating
seizures. For example, for a specified duration (e.g., every hour, every day)
that a dient did not demonstrate a seizure, he or she would be awarded several
points. Points could be redeemed for items or activities from a menu of
reinforcers.
Reinforcement also can be provided for behaviors incompatible with
seizures. These reduction procedures are called differential reinforcement of
incompatible behaviors (DRI). With a DRI, behaviors that are topographically
incompatible with operant seizures are reinforced whenever they occur. For
example, behaviors incompatible with seizures are going for a walk, sitting at
a table, and playing a game. These behaviors cannot occur simultaneously
with seizures and are behaviors we want to see increase. A consideration when
using DRI is that all staff must consistently rein force the designated incom-
patible behaviors. For example, ifthe behavior incompatible with seizures is
walking without falling, then all caregivers would reinforce this behavior.
Reinforcers must be selected according to individual preference. Rein-
forcers are defined by their effect on behavior (increases or maintains behavior);
they are not defined by what staff, peers, or relatives believe is reinforcing. If
reinforcement is provided at a high frequency, certain activities or items are
easy to use. These indude points, verbal praise, social attention, and certain
activities. These items or activities should be presented immediately. Rein-
forcers that may not be as easy to use indude community outings, dinner
out, and other reinforcers that have to be delayed. We recommend using
social praise with other reinforcers so they acquire conditioned reinforc-
ing value.
172
CHAPTER 8
Combining Techniques
When possible, it is desirable to combine extinction with reinforcement
rather than using one technique alone. The rationale for combining techniques
is that desirable behaviors are being taught (e.g., engaging in activities, holding
a conversation without talking about seizures, how to gain attention correctly)
while seizures are reduced.
Zencius and Wesolowski (1989) combined ignoring seizures and weekend
outings contingent on nonoccurrence to decrease operant seizures in a 20-
year-old female. Before treatment, the dient received excessive attention from
staff during and after a seizure. She was excused from scheduled programming,
received meals and medication in bed, and a staff person observed her one-
on-one. After it was determined that there was no organic basis for the seizures,
ignoring and contingent weekend outings were initiated. Staff were trained
to break eye contact with the dient and leave the immediate area anytime
she engaged in a seizure. It was explained to the dient that if she had a seizure
during the week, the risk was too great that she might have another while on
an outing and injure herself. The dient, however, was permitted to attend all
weekend outings ifno seizures occurred throughout the week. Weekend out-
ings consisted of trips to the shopping malls, movie theaters, bowling alleys,
dances, and dining out. Figure 8.3 shows that the seizures were eliminated
by using these combined procedures.
Base TX Baseline
Contingent Outings and Ignoring
6
LlNDA
4
2 ..
o __
o
10 20 30
Time in Weeks
FIGURE 8.3. The effects of planned ignoring and contingent weekend outings on operant seizures.
PROCEDURES FOR HEAL TH AND MEDICAL PROBLEMS 173
HYPOCHONDRIACAL STATEMENTS
Frequently, survivors of brain injury suff er pain from the initial injury.
For example, an individual who was in a motorcyde accident and fractured
several bones may experience pain several months and even years following
the accident. Ifpain becomes chronic (i.e., lasting more than 6 months), pain
behaviors will be positively and negatively reinforced. With positive rein-
forcement the dient receives attention for complaining or showing signs of
pain (e.g., facial grimaces, statements about pain, holding the lower back).
For example, a dient at arehabilitation facility complained of headaches
where he had hit his head during a car accident. As a result, caring staff
members would sit hirn down, bring hirn an aspirin, spend time talking with
hirn, and tell hirn that he would be fine. In this case, the presentation of the
contingent attention from staff reinforced complaints of headaches.
With negative reinforcement, activities or events are avoided because of
statements of pain. For example, a dient complained of severe pain during
physical therapy sessions. As a result, the physical therapist excused the dient
from the group. In this case, contingent removal of an activity (physical therapy
exercises) was negatively reinforcing statements ofpain.
Extinction
As discussed with operant seizures, extinction is the procedure in which
a previously reinforced behavior is no longer reinforced. Using extinction,
hypochondriacal statements would be ignored. If the dient complained of
headache, for example, caregivers would ignore the comment and give atten-
tion to the individual when he or she was not complaining of pain. Although
extinction techniques sound procedurally easy, they are difficult to carry out.
All staffmust respond consistently. One important consideration when using
extinction is that the behavior usually gets worse before getting better. For
example, if a dient complained of pain 40 times a day, when extinction is
first implemented, complaints may increase to 50-60 times a day. It is im-
portant to continue the procedure even though the behavior is getting worse.
Extinction programs developed to reduce hypochondriacal statements should
indude breaking eye contact, leaving the immediate area if possible, and
responding to another person who is acting appropriately.
Reinforcement
All of the reinforcement techniques discussed under the operant seizure
section also can be used to decrease hypochondriacal statements (e.g., behavior
contracts, point systems). With behavior contracts, the contract would be met
174 CHAPTER 8
if a specified number of hypochondriacal statements were made during a
contract period. For example, a contract could specify that only five or less
statements could be made each day. Contracts could be used on a frequent
basis such as daily or less often such as once a week.
Differential reinforcement of incompatible (DRI) and other behaviors
(DRO) also can be used to decrease the frequency of hypochondriacal state-
ments. When using a DRI, statements incompatible with pain statements
would be reinforced (e.g., statements about feeling good, holding a conver:
sation without complaining). If a DRO were used, any other behavior besides
verbal complaints would be reinforced on some time schedule, the interval
of time being slightly shorter than the time between occurrences of the hy-
pochondriacal statements.
As an example of using a DRI procedure to decrease hypochondriacal
statements, a young male dient was released from arehabilitation facility and
placed in apart-time vocational site. He initially complained daily about pain
and illness at the work site. Treatment consisted ofhaving the two vocational
supervisors reinforce behaviors incompatible with complaining. They praised
the dient for working, conversing with others, not complaining, being on
time from breaks, asking permission, and accepting and following instructions.
After 3 months, the supervisors reported that verbal complaints of pain had
disappeared.
Combining Techniques
We recommend that extinction and reinforcement be combined when
attempting to reduce hypochondriacal statements. That is, use extinction every
time statements are made and use a reinforcement when hypochondriacal
statements are not made.
We (Zencius and Wesolowski, 1990) decreased complaints ofillness by
using extinction and behavior contracts. After the dient was examined by the
facility's physician for medical problems, intervention was initiated. The ex-
tinction procedure consisted of staffbreaking eye contact, discontinuing con-
versation, and leaving the immediate area. Behavior contracts were written
once a week. On the day the contract was written, the behavior specialist,
team leader, and dient agreed on how many verbal complaints could occur
throughout the week. The contract was met if the dient made that number
or less. The initial contract specified that 20 complaints a day was acceptable.
Within 10 weeks, this decreased to an average of one a day.
BULIMIA
Bulimia is a condition particularly prevalent among young females and
is characterized by the binge-purge phenomenon. That is, the person eats
PROCEDURES FOR HEAL TH AND MEDICAL PROBLEMS 175
large amounts of food and then vomits. Bulimia can cause dental decay and
ion imbalances that, in extreme cases, can result in death.
The prevalence of bulimia in the nondisabled population is largely un-
known, but recent surveys indicate that as many as two-thirds of college fe-
males have engaged in binging and purging (Foreyt & Kondo, 1985). This
being the case, it would not be surprising to find persons with bulimia among
survivors of head injury. We have successfully treated three females who
exhibited symptoms of bulimia. The treatment package included seven
components.
1. Reinforce weight gain. Clients suspected ofhaving bulimia should be
weighed at least twice a day, and weight maintenance or gains should
be reinforced.
2. Self-monitoring ofbinging, associated thoughts and feelings, presence
or absence of others, and the particular environment involved should
be initiated. Self-monitoring serves not only as a reduction technique
but also as an impulse delay strategy.
3. Stimulus control to limit the environmental cues leading to binge
eating. These include removal of binge foods and avoidance of prob-
lematic eating situations (e.g., particular restaurants or being alone
during specific hours, particularly after eating). In a residential facility,
one might try using preprepared meals.
4. Staff monitoring of purging episodes should augment client self-
monitoring of binging. In so me cases, this might necessitate staff ae-
companying clients into the restroom (a possible violation ofprivaey),
but we have found disconnecting the bulb on the toilet so it will not
flush to be a useful method of monitoring vomiting. Clients suspected
ofbulimia should be tightly programmed (given activities) far 2 hours
after eaeh meal to avoid opportunities to vomit.
5. Social skills training for bulimics is useful because interpersonal deficits
are often observed in noninjured bulimics with respect to assertiveness,
communication, and basic problem-solving capabilities. Among brain-
injured persons, the lack of these abilities would likely be enhanced.
6. Cookingjnutrition classes are beneficial in that they teach clients eor-
reet management and preparation of foods, nutritional values, and
appropriate portions. They also can make clients more comfortable
around food since most bulimics have an obsession with food.
7. Beauty classes eould be formed to teach clients to foeus on their ap-
pearance and ways to improve it. They also may improve body image.
These classes ean include techniques in applying makeup, hair dress-
ing, sewing, and fashion design. Area professionals and students in
these fields can be invited to give volunteer demonstrations to clients
and staff.
176 CHAPTER 8
In addition to this procedure, Azrin and Wesolowski (1975) successfully
treated a brain-injured female who vomited by using simple correction and
positive practice. When the client vomited, she was required to clean up the
mess by mopping the floor and washing her clothes (simple correction) and
then practice the correct way to vomit by running three times to the toilet
from where the vomiting occurred (positive practice).
OBESITY
Obesity is a problem in most populations; however, Black, Jeffries, Blu-
mer, Wellner, and Walker (1969) and Wesolowski and Burke (1988) identified
overeating as a characteristic common to head-injured adolescents. Rotatori
and Fox (1980) developed a weight reduction program for moderately retarded
adolescents. We have found the content ofthis program suitable for persons
with brain injury. The program has four components: parentjspouse involve-
ment, staff involvement, reinforcement, and maintenance.
Parent/Spouse Involvement
Prior to initiating the program, parents and spouse attend a meeting with
staff. They are trained in behavioral weight reduction techniques and famil-
iarized with recording forms to be completed by the overweight person. The
parents' and spouse's roles during the program include providing directions
and feedback in conducting the techniques and administering reinforcement
for weight loss.
Staff Involvement
Clients meet with a staff member three tim es a week during the 14-week
treatment phase. The meetings are designed to provide instruction in behav-
ioral weight reduetion teehniques and in procedures for completing homework
assignments (e.g., a food diary and weight reduetion reeords). Behavioral ap-
proaehes include manipulation of emotional responses (Hall, 1972), food eue
elimination (Stuart, 1969), ehanging eating behavior (Stuart & Davis, 1972),
using exereise to burn unneeded ealories, and developing alternative aetivities
to eating (Ferguson, 1975). Two proeedures are introdueed each week.
Manipulation of emotional responses eonsists of having the clients ver-
balize the undesirable eonsequenees of overeating. When one is tempted to
overeat, one might say, for example, "My friends will eall me Fatty." They
PROCEDURES FOR HEAL TH AND MEDICAL PROBLEMS 177
are also taught to verbalize pleasant consequences when they are successful
in not overeating-'Tm going to look great." Food cue elimination involves
specifying one place to eat meals and snacks, leaving some food behind on
the plate, and taking only one helping. Changing the act of consuming food
includes eating more slowly than before, chewing food completely, and putting
utensils on the table between taking bites. Developing of alternative activities
to eating involves encouraging clients to engage in pleasant activities that
compete with eating, such as going for walks, listening to records, or working
on a craft project. They also are expected to burn unneeded calories by en-
gaging in a lO-minute exercise period twice a day.
A number of instructional modalities are employed to facilitate under-
standing of the behavioral procedures during the intervention. First, the be-
havioral procedures are verbaIly described along with a simple rationale. The
teacher then models the procedure. This demonstration is foIlowed by having
clients imitate the procedure in simulated situations. Comments are given on
their practice trials. Additional feedback is provided by a staff member who
observes during meals. Parents and spouse are required to write regular pro-
gress notes on the person's use ofthe techniques to increase implementation
in the horne. The notes are foIlowed up with bimonthly phone caIls to parents
and spouse by staff members to discuss in detail the progress of the client in
attaining mastery ofthe techniques as weIl as implementation concerns. These
progress notes and phone caIls serve as reliability checks to assess program
implementation in the horne.
Reinforcement
During the intervention phase, aIl clients receive facility and horne re-
inforcement at the end of the school/work week for weight loss. Clients have
to lose one pound or more between sessions to receive reinforcement for
weight loss. The horne reinforcement is an activity desired by the person, e.g.,
bowling with dad. Facility reinforcement is a group activity usuaIly chosen
by the majority of persons (e.g., attending a dance on Friday night).
In addition, clients rate their performance daily on the techniques they
have been using on a behavior checklist. Based on their ratings, clients receive
a grade that depends on the total rating each person has earned for employing
the techniques. The particular rate earned is then exchanged for an envelope
that contains self-reinforcement guidelines. The self-reinforcement guidelines
are divided into two areas: activity reward and a self-administered positive
statement.
Maintenance
The maintenance training phase begins immediately foIlowing the 14-
week treatment period and lasts for at least 5 weeks. During this phase, aIl
178 CHAPTER 8
clients attend meetings. The maintenance meetings include a videotape pre-
sentation, which reviews the behavioral techniques presented during the in-
tervention phase and a review of self-monitoring forms. Horne and facility
reinforcement conditions are continued during this phase.
DIABETES
We have encountered two clients who manipulated staff by raising or
lowering their blood sugar levels through diet changes and exercise. In both
cases, individualized point systems were used where keeping blood sugar levels
(levels were measured each moming) within a certain range was reinforced
with points and backed up by activities and tangible reinforcers. This resulted
in blood sugar levels being kept within the desired range.
SUMMARY
Assistive Devices
1. Following TBI, many survivors are required to use assistive devices.
On occasion, clients refuse to use these devices or become overly
dependent on them.
2. Commonly used assistive devices for TBI survivors include wheel-
chairs, walkers, quad canes, straight canes, heImets, and leg and arm
braces.
3. Consequence management techniques such as point systems, level
systems, behavior contracts, and the Premack Principle can be used
to both increase use of and decrease overdependence on assistive
devices.
4. Antecedent control techniques can be effective in increasing use of
assistive devices particularly with those clients who have memory
deficits.
Operant Seizures
5. Operant seizures are seizures that are maintained because clients
receive positive or negative reinforcement for them.
6. Extinction is a procedure in which reinforcement of a previously
reinforced behavior is discontinued. Extinction can be an effective
procedure for decreasing the frequency of operant seizures when
administered consistently.
PROCEDURES FOR HEALTH AND MEDICAL PROBLEMS 179
7. When using motivational techniques to decrease operant seizures,
reinforcement is provided for a decrease or absence of seizures.
8. When reinforcement is provided for behaviors incompatible with
seizures, a schedule of differential reinforcement of incompatible
behaviors is in effect.
Hypachandria
9. Hypochondriacal statements are maintained by positive and negative
reinforcement contingencies. With positive reinforcement, the client
receives attention for demonstrating pain behaviors or verbalizations
regarding pain. With negative reinforcement, unpleasant activities
or events are withdrawn or avoided because of statements of pain.
10. Differential reinforcement of other behaviors and incompatible be-
haviors is used to reinforce the nonoccurrence of or behaviors in-
compatible with the target behavior.
11. It is recommended that extinction and reinforcement procedures be
combined when attempting to decrease both operant seizures and
hypochondriacal statements.
Bulimia and Weight Lass
12. Bulimia is a condition particularly prevalent among young females
and is characterized by the binge-purge phenomenon. That is, the
person consumes large quantities of food and subsequently vomits.
13. Treatment of bulimia consists of seven components: (a) reinforce-
ment of weight gain, (b) self-monitoring of binge-purge behaviors,
(c) stimulus control of environmental cues, (d) staff monitoring of
binge-purge behaviors, (e) social skills training, (f) cooking/nutrition
classes, and (g) beauty classes focusing on appearance.
14. Obesity is a common problem among all populations. Recently,
however, researchers have found overeating to be a frequent char-
acteristic of adolescent TBI survivors.
15. A program for weight reduction includes four components: parent
or spouse involvement, staff involvement, reinforcement, and
maintenance.
9
The Role of the Family
Therapists should incJude the family members in planning rehabilitation.
Family members' concerns and expectations must be addressed for long-term
success (Livingston & Brooks, 1988). The brain-injured individual is a member
of an interdependent system (thc family) and changes in any member affect
that system (Guth, Lasseter, & Harward, 1988a). Many family members at-
tempt to deal with injury or disability by either increasing the rigidity of
existing roles or creating new roles for members. These changes in patterns
of interaction, role definitions, and allocations of resources can either promote
or interfere with successful family functioning.
Many survivors ofhead injury return horne to their families even though
this may not be the most appropriate placement. The scarcity of community
placement opportunities and the limitation offinancial resources force many
families to care for the injured survivor in their horne. Family members'
ability to manage stress and their knowledge of and adjustment to long-term
disability will impact the survivor's care as weil as the lives of other family
members. It is crucial that the rehabilitation team recognize these variables
and their long-term effect when designing a comprehensive treatment program
for the brain-injured survivor and his or her family.
This chapter reviews common characteristics offamilies affected by TBI,
discusses the stages of adjustment that families often undergo, and highlights
special issues that often arise. Its intent is to provide suggestions that can be
applied by practicing professionals in their work with brain-injured individuals
and their families.
FAMILY REACTIONS TO HEAD INJURY
Families react differently to the devastating reality of head injury. The
family's reaction is influenced by many variables, some of which are the
181
182 CHAPTER 9
characteristics of the injured individual, family dynamics, the nature and
severity of the injury, and the availability of resources.
The Injured Individual
Characteristics ofthe injured individual that influence the family mem-
bers' reaction to disability include the age of the person and his or her role
within the family. For example, ifthe individual were considered successful
and relied on for support, his or her injury would disrupt the family differently
than if that person were unemployed and dependent.
Family Dynamics
Family dynamics refers to the flexibility and range of roles of family
members. Family members with rigidly defined roles may be greatly affected
by disability. For example, if the wife previously assumed responsibility for
the housework and child care, a long hospital stay could create a gap in how
the family previously operated. Families with flexible roles, however, may be
better able to make adjustments to maintain successful functioning after injury.
If the family has a strong network of extended family and friends, the
probability of the family surviving the crisis and regaining equilibrium is
increased. It may require outside assistance in obtaining support to ensure
continued functioning if these natural supports are lacking.
Head injuries often occur in families that are poody equipped to absorb
the impact. Many individuals who become traumatically brain injured are
considered "risk takers" and their families are considered dysfunctional.
Problem-solving abilities may be poor or ineffective, and the injury may be
enough to destroy the family as a working unit.
Severity oi Injury
The severity of the injury often affects family members' reaction to it.
Families ofvictims with severe injuries expenence high levels ofstress during
the acute phase ofrecovery. Contact with hospitals and medical equipment
can be frightening. This combined with concern for the person's survival can
be overwhelming.
The types and severity of residual deficits over the course of recovery
also will influence the family's adjustment to the disability. Awareness ofthe
permanence of some disabilities plays a critical role in family members' ability
to assist the injured individual. Physical disabilities require greater levels of
physical assistance; however, cognitive and behavioral deficits may be the
most difficult for family members to manage over time. The severity of injury
THE ROLE OF THE FAMILY 183
and the nature ofthe deficits, therefore, have an impact on the family's reaction
to TBI. Table 9.1 describes common family responses and interventions during
the course of rehabilitation.
Stages
Families aficted by injury or chronic disease of one of its members go
through stages similar to the individual grieving process described by Kubler-
Ross (Brown & McCormick, 1988). Family members typically respond to
injury with shock, panic, despair, denial, and finally acceptance.
Crisis intervention techniques should be used such as listening (which
provides opportunities for ventilation of feelings), assistance with problem-
TABLE 9.1. Family Responses and Sampie Intervention Techniquesfor the Course
of Rehabilitation
Rehabilitation stage
Injury to stabilization
Return to conseiousness
Transfer to rehabilitation
Transfer to postacute
rehabilitation
Discharge horne
Family response
Shock, panie, despair, denial
Anxiety, endless waiting,
claims of unsubstantiated
improvement, continued
denial
Mixed emotions (hopejfear),
overinvolvement,
hypercritieism of rehab andj
or staff, anger. Beginning of
extended disabilities
Mixed emotions (renewed
hopejfear) possible
depression, overinvolvement
or possible disengagement,
disenchantment. Beginning
acceptance and adjustment
Reality, shock, renewed or
inereased stress, role
ehanges, acceptance,
adjustment
Intervention
Crisis intervention (active
listening, ventilation, ease
work, problem-solving,
allowing hope)
Edueation, beginning
involvement in patient
care, expression of fear
and validation offeelings
Establishing trust in rehab
team, education in TB!,
involvement in treatment
planning, establishing
outside support systems,
assessment offamily
functioning
Family assessment,
integration into family
training, family therapy,
solidify extern al support
Support, respite, therapy
184 CHAPTER 9
solving, and provision of resource information. Basic information regarding
the performance of medical equipment will be helpful in alleviating anxiety.
Family members usually expect total recovery when the survivor is about
to be released from the hospital and fall into despair and denial when this
does not occur. TBI education as weIl as involving family members in the
daily routines of the dient should be offered. Most family members will express
fears regarding long-term prognosis.
Family members process information and move through grief stages at
different rates. While fallacies about total recovery can make the decision-
making process ineffective, confrontation can precipitate further despair. Ex-
perienced, professional judgement must be used in determining timing of
confronting family members' denial.
TRANSFER TO POSTACUTE SETTINGS
When the survivor is transferred from the hospital to a residential re-
habilitation center, many family members experience mixed feelings. They
are hopeful that the transfer is indicative of progress, yet they fear the new
setting, new staff, and the knowledge that the family member cannot return
horne at this point. Family members are often dissatisfied with the rate of
progress and may express their concerns through criticism of staff. This crit-
icism may be heard as the dient moves to postacute services. The rehabilitation
professional should assist family members in gaining confidence in the treat-
ment team at this point. This will establish a relationship between family and
treatment team members that will be critical for discharge planning. Recog-
nition by the treatment team of these issues may indicate the need to initiate
a formal family assessment and education.
SPECIAL ISSUES, ROLES, AND PLA YERS
Emotion
The feelings associated with a family member suffering a brain injury
can cause dysfunctional patterns ofbehavior. It is natural for family members
to experience shock, despair, helplessness, guilt, and anger. These emotions
can be useful and productive. They become dysfunctional only when they
evolve into behavior patterns that threaten other family members' functioning.
For example, anger, if channeled into effective advocacy for the injured family
member, can be a motivational force to obtain services. It becomes dysfunc-
tional ifit is carried into situations where others are blamed for events outside
THE ROLE OF THE FAMILY 185
their control such as causing the original accident. Oenial can be considered
functional if it helps family members maintain hope and continued func-
tioning during crisis. Oenial becomes dysfunctional when it interferes with
the family member's participation in rehabilitation. Sadness and grief are
functional ifthey allow family members to work through the mourning process
for the deficits of the injured survivor. These feelings become dysfunctional
ifthey persist, block family decision-making, and lead to the neglect offamily
responsibilities and activities.
Preexisting Issues
Areas of limited functioning prior to the injury may impact upon some
family members' ability to adjust to disability. These issues might include a
history of substance abuse or physical or sexual abuse. When these preexisting
difficulties exist, the therapist must consider their impact on family members'
ability to work with the rehabilitation team. Returning the injured member
to the family may not be a realistic goal.
Maladaptive Rales
Ouring a lengthy stay at horne, family members may promote dependence
in the client. They may inadvertently sabotage the goal of rehabilitation, i.e.,
to function independently. It is the responsibility ofthe treatment team mem-
bers to assist family members in the assumption of new roles that will foster
the survivor's continued recovery.
Marital Issues
The spouse of an individual with brain injury has special concerns. It
can be particularly devastating to a marital relationship to have an individual
receive an injury resulting in long-term behavioral, cognitive, and physical
changes. The partner one married is simply no longer there. He or she has
been replaced by astranger. The divorce rate in this situation is high and
often spouses will find themselves assuming the role of caretakers when once
they were partners. Feelings of anger, resentment, sexual frustration, and
depression are common (Zeigler, 1987). Even in minor head injury or post-
concussion syndrome, the individual may have lifelong episodes ofheadaches,
dizziness, and irritability. The survivor's ability to return to employment is
often compromised. These variables combine to instigate a role change be-
tween the marital partners. For example, if the survivor was the "breadwinner,"
the spouse may have to ass urne that responsibility. For some couples, ad-
justment is a reasonable expectation; however, other couples are unable to
186 CHAPTER 9
make the necessary changes. Marital counseling is often indicated and should
be conducted by a therapist who not only understands marital and sexual
issues but also has a knowledge of TBI and its long-term implications.
Young Adults
If a young adult is the victim of TBI, some family members become
locked into caretaker roles. Guilt feelings or fear of recurrent TBI may prevent
independence. Family members may find themselves in the position ofbeing
unable to "let go." In a follow-up study of young adults placed at family
members' hornes versus supervised situations, Burke, Wesolowski, and Guth
(1988) found that individuals returning horne had lower levels of independence
and vocational produCtivity than persons placed in supervised settings (group
hornes). It was hypothesized that family members "provide for" rather than
"work with" or challenge the injured individual. In cases where aggression is
present, family members may change their behavior to avoid outbursts, which
prevents them from dealing with the aggression. In rehabilitation centers,
family members may be overly concerned for the safety ofthe TBI survivor.
This may translate into hesitancy in agreeing to initiate more risky vocational
and recreational endeavors.
Siblings
Siblings of survivors have many of the same reactions to TBI as parents.
Yet, these individuals frequently do not receive counseling or training in what
to expect. In addition, parental attention is focused on the injured individual.
This often results in feelings of neglect by siblings. Truancy, difficulty with
authority, and potential for substance abuse are considered likely c.onsequences
for the siblings ofbrain-injured survivors. It is imperative that the treatment
team provide parents with information concerning the effect of TBI on the
survivor's siblings.
Children
In the situation where the TBI survivor is a parent, the children often
experience difficulties. In some cases, the children may take on the role of
caretaker for the parent. In many cases, they are relied on by the other parent
for assistance, causing the brain-injured survivor to become resentful of the
children's abilities (as compared with his or her own). The children may
experience resentment, particularly surrounding behavioral difficulties of the
survivor. As with siblings, the children may feel neglected by the survivor and
by the other parent. Preteaching family members regarding early warning
THE ROLE OF THE FAMILY 187
signs is imperative for effective intervention. Follow-up sessions dealing with
these issues (even after discharge ) should be established. Family members also
should be instructed to direct a portion ofthe family's time to the children's
preferred activities.
When the brain-injured survivor is a young child, family services become
pivotal in the rehabilitation process. Indeed, it has become customary to speak
of"head-injured families" as well as head-injured individuals. Because ofthe
crucial role of the family in the lives and development of children, attention
to family needs and to the family's role in the child's rehabilitation is a nec-
essary condition for successful rehabilitative outcome.
Growth/Development
A child's behavioral and attitudinal development are directly linked to
the family (McKinley & Hickox, 1988). This observation has important im-
plications for recovery following brain injury and for rehabilitation planning.
The treatment plan must be based, in part, on the assumption that gains
achieved in a rehabilitation setting (particularly behavioral gains) are unlikely
to generalize to a horne in which the family is poorly oriented to the child's
functioning and good behavior management practices (Burke, Wesolowski,
Buyer, & Zawlocki, 1990). Planning is complicated by the natural tendency
of parents to be protective of vulnerable children. It is natural for parents to
be overprotective following brain injury, but this jeopardizes the normal de-
velopmental process of independence. Furthermore, the responsibility as-
sumed by most parents to protect their children from harm easily produces
guilt when the child is injured (Waaland & Kreutzer, 1988). This occurs even
if the parents were in no way responsible for the accident. This often unac-
knowledged guilt can interfere with the parents' interaction with rehabilita-
tion staff.
Primary Caregivers
Because of their caregiving role, parents play an important part in re-
habilitation assessment and treatment. In pediatric assessment, the staffmust
acknowledge and make effective use of family members' knowledge of the
child's functioning. In treatment, most parents can assurne, with the appro-
priate training, a caregiver role. Playing this role, however, requires careful
guidance from therapists on the treatment team.
While family members experience similar reactions to head injuries with
children as they do with adults, there are differences. For example, respon-
sibilities for child care produce profound guilt which may be greater than that
experienced with families where an adult is injured. In addition, when children
188 CHAPTER 9
are injured, assuming a nurturing, protective role is less disruptive to family
members' routines than with older adolescents or adults.
Discharge
Family members with injured children generally experience adjustment
similar to those with adults. The discharge horne for children, however, can
be particularly distressing. The early weeks following discharge is the time
when family members attempt to re-create a comfortable routine; however,
this is when parents have to face their new realities: demanding physical care
and behavioral and cognitive changes in their injured child. Conflicts may
emerge between parents over roles and limits for the child. For parents who
do not have access to respite services, stress may lead to anger toward the
disabled child. The negative effects of disability on family members may, in
fact, intensify as the child develops into puberty. It is often when the child
reaches adolescence that families feel the most desperate need for assistance.
With successful assessment and treatment, family members can adjust
to the reality of long-term disability, thus becoming effective partners with
rehabilitation teams in recovery. The following section will describe available
methods of assessment as aprecursor to services that should be provided to
families.
ASSESSMENT
With the survivor's stabilization and transfer to arehabilitation facility,
family members are better able to participate in a structured, data-collecting
process.
Goals
The purpose of a comprehensive family assessment is to identify
1. All family members and their level of involvement
2. Family members' interaction patterns
3. The level of family members' knowledge of TBI
4. The types and availability of support and resources
5. Sources of stress to family members including financial, maladaptive
behavior patterns, and other dependents in the horne setting
THE ROLE OF THE FAMILY 189
Methods
There are three different suggested methods of assessment: structured
interviews, questionnaires (self-report inventories), and observation. Bishop
and Miller (1988) review specific tools developed for family assessment. They
also discuss what is measured, the instrument's validity, and the interrela-
tionship among different assessment instruments.
Interview
A structured interview serves several purposes. Frequently, it is the initial
contact between members of the rehabilitation team and family members.
The initial interview can formulate trust in the rehabilitation team and uncover
parts of the family history that were previously unknown. The use of checklists
or standard questions ensures that the same data are gathered ac ross different
family members being treated by the rehabilitation program. This allows for
longitudinal evaluation across dient or family groups and comparison offam-
ily members' progress.
Se!fReport
Questionnaires are usually used in conjunction with structured interviews.
Using questionnaires allows for repeated administration to monitor progress
within the family over time. They also ensure consistency across families for
program evaluation. When administered early in rehabilitation, questionnaires
can give a family member concrete tasks to perform-another useful inter-
vention in assisting family members in dealing with stress. The timing of
administration can be critical, for if administered too soon after the injury,
the questionnaire can be viewed as "just one more form." Family members
should understand the purpose of questionnaires to facilitate open, honest
answers. There should be adequate time and a comfortable setting provided
with minimal distractions.
Structured Observation
Observation is considered the most effective method of assessing family
interaction. Observation can take place either in the natural horne setting or
in an artificial, laboratory environment. There are advantages and disadvan-
tages to both. Observation in the natural horne setting evokes more "nor-
malized" family interactions; however, tasks are difficult to standardize across
different families. In addition, family members may be on their "best behavior"
when visitors are present and, therefore, may not exhibit dysfunctional or
190 CHAPTER 9
ineffective interaction patterns. This can be minimized by scheduling multiple
observation sessions at varying times during the day.
In laboratories, tasks similar to those in the ho me can be given to family
members. This not only provides data across family members, but also allows
observers to improve skills through repeated observation of the same tasks.
The laboratory environment, however, may create artificiality in family in-
teractions. The tasks assigned may or may not be applicable to every family
member. We recommended, therefore, that families perform certain applicable
tasks from a standardized test. For example, it would not be useful to require
a physical therapy activity of a family member whose brain-injured survivor
experiences only cognitive or behavioral deficits. It would be useful, however,
to observe family members setting limits with this person. The laboratory
setting may increase stress in some family members. This can be useful for
the therapist in data collection as family members may exhibit familiar be-
havior rather than "best behavior." It is ideal to observe the family both in
the laboratory and in natural home settings.
The purpose of an assessment is to obtain the information to develop
interventions and make comparisons of the effects of treatment with prein-
tervention levels. Frequently, assessment relies only on the interview process.
This has limitations including the inability to validate subjective viewpoints
of the interviewer. Determining lines of communication, assessing problem-
solving abilities, and verifying roles within family members will assist the
evaluator to identify the best intervention.
FAMILY SERVICES: INTERVENTION/INTEGRATION
Primary services are those that need to be provided by rehabilitation
programs, and secondary services are those that rehabilitation programs must
have access to for appropriate referral. The primary services consist of edu-
cation, family training, therapeutic home visits, and advocacy. The secondary
services include family therapy and marriage or sexual counseling.
Assumptions
Services to family members are predicated on three assumptions. First,
family members differ in their premorbid functioning and dynamics. Second,
some families have more external resources. Third, family members require
different interventions at different stages of adjustment. All of the above as-
sumptions underline the importance of an effective assessment process for
family members of brain-injured survivors. With the knowledge of family
roles, patterns of communicating and interrelating, and the availability of
THE ROLE OF THE F AMIL Y 191
support, the rehabilitation team can assist the family in adjusting to new
endeavors.
Education
Education of family members is the most effective tool that can be used
to help family members adjust to their new circumstances. The education
process begins at the time of injury and continues beyond discharge. Infor-
mation should be nonthreatening and should provide reassurance and allay
anxiety caused by new and unfamiliar settings. Through supplying infor-
mation, the therapist can establish relationships between the rehabilitation
team and family members. Many family members will find it difficult to
absorb all of the information that is presented to them. It is always preferable
to provide written supplements such as handouts and artic1es with all oral
presentations. Family members should be encouraged not only to digest in-
formation provided by the treatment team but also to seek additional artic1es,
books, or pamphlets on their own. They also should be encouraged to ask
questions regarding all information. Therapists should ensure that adequate
time is provided to answer questions. Time taken in the early stages may
prevent incorrect perceptions or assumptions and facilitate support by the
family members in the later stages of rehabilitation. While this is particularly
true in the early or acute stages, it will carry over throughout the entire course
of rehabilitation.
Information on external resources or supports, such as the National Head
Injury Foundation or financial assistance, can alleviate some of the stress
when family members do not know where to turn for answers and assistance.
Suggestions for structuring resources such as holiday time saved at work or
juggling schedules to provide staggered visitation also can be helpful.
More thorough education regarding brain injury is generally given at the
later stages of rehabilitation. Distributing information regarding residual dis-
abilities can be important in fostering understanding, acceptance, and appro-
priate participation in the rehabilitation program by family members.
Group Education
Providing family education in groups has limited success. Individuals
come to sessions with specific agendas and have little patience with information
that they do not perceive as specifically applicable to their injured family
member. Attendance may be sporadic for a variety ofreasons (e.g., distance,
employment, or other family obligations). Invitations to attend formal staffing
or progress review meetings with treatment teams may encourage family
192 CHAPTER 9
members to participate in the specifics of the rehabilitation plan. This in-
volvement will keep family members abreast of treatment progress.
Audio/Video
Audiotapes or videotapes may be preferable to written information. Such
materials are available through the National Head Injury Foundation's ed-
ucation department and cover a wide variety of topics. Information on the
injured individual's functioning and progress can be obtained by videotaping
therapies and activities.
Information regarding the dient's abilities and disabilities will better en-
able the family members to support the rehabilitative process. Education can
also foster family utilization of community resources. Many rehabilitation
facilities have general TBI educational curricula intended for family members.
It is important to tailor the materials to the family member concerned. Early
in the recovery process, family members are often interested in receiving
general TBI information; however, in later stages of rehabilitation, they are
most concerned with information that applies specifically to their loved one.
Farnily Training
A variation of family education is family training, the difference being
that family training is a specific, skill-based, activity that will enable family
members to participate in the head-injured individual's rehabilitation. This
may indude implementing cognitive compensatory strategies or behavior
management programs. Each skill area is specific to the survivor and creates
what Quinn, Pierce, and Lyle (1988) described as "a lay therapist approach."
By transforming family members into "lay therapists," rehabilitation profes-
sionals gain the benefit ofhaving family members familiar with the programs
the dient is working on. Through this training, family members will be better
equipped to cooperate with the treatment team in the rehabilitation of the
dient.
Many brain-injured survivors will return horne following their rehabil-
itation, and family members will become the caretakers. Without family
training, treatment gains made at the rehabilitation facility will usually not
be maintained. Treatment strategies designed in a residential facility cannot
be expected to generalize to the horne environment; generalization must be
programmed.
Horne Visits
A therapeutic horne visit can be an integral part of TBI rehabilitation.
Horne visits can be counterproductive during a long course of rehabilitation
THE ROLE OF THE FAMILY 193
in that many treatment gains can be lost. When the horne visit is planned
and structured, training the family members and giving them homework as-
signments on treatment strategies, the horne visit becomes therapeutic. Ther-
apeutic horne visits can be an opportunity to promote generalization of skills.
In addition, therapists can assess the dient's functioning within the horne
environment.
Preparation
To plan the therapeutic horne visit, it is necessary to define its purpose.
This involves writing objectives to be accomplished and specifying the fre-
quency oftherapist contact with family members prior to and while the dient
is at horne. Prior to the actual visit, ahorne assessment should be made. The
areas assessed should indude safety issues, accessibility, level of supervision
in the horne environment, and safeguards for younger children or other
dependents.
Prior to the horne visit, the family members need to be trained in tech-
niques used at the rehabilitation facility. These may indude physical tech-
niques such as transfers or behavioral strategies designed to assist clients in
maintaining what they have learned. Family members must also be trained
in the documentation that is required by the treatment team. The request for
documentation should be kept short and should only indude information
that is needed by the rehabilitation team. A sam pie set of forms developed
by Guth et al. (l988a) is induded in Appendix E. The rehabilitation team
should preview with family members potential pitfalls and then problem-
solve and role-play strategies that may be helpful should those situations arise.
Evaluation
Following the horne visit, it is important to evaluate its success or failure.
This will help in planning the next therapeutic horne visit. As the dient ap-
proaches discharge, horne visits should become more frequent, with discharge
being characterized as a "trial placement."
A therapeutic horne visit also can lessen the impact of a cJient's final
return horne. Family members who were unable to participate in the reha-
bilitation process can be exposed to the dient, thus maximizing the probability
of acceptance.
Support
Families that have large social networks are better able to co pe with
stressful situations (Wesolowski, 1987). Many families perceive support groups
194 CHAPTER 9
(comprised of individuals with similar experiences) as a primary coping
mechanism. The National Head Injury Foundation has established anational
network of support groups to assist survivors, families, and friends in coping
with TBI. In some areas, "response teams" have been established. These teams
are comprised of volunteers who are available at area hospitals to meet with
families in the initial stages of treatment.
Because of the behavioral changes that many clients undergo, it is not
unusual for friends to stop seeing survivors over time. Family members,
therefore, often require support outside immediate friends or extended family.
The National Head Injury Foundation, church, and social organizations have
been suggested as viable long-term support options for families.
Professional Support
Professionals also must remain available for supportive counseling, crisis
intervention, or just continued contact with the family. While the stress of
dealing with TBI does level off, the need for assistance continues.
Respite Care
Many family members will need respite care while caring for the brain-
injured survivor. Professionals may make referrals or provide information
about respite care services that are available. Placing the survivor outside the
horne can enable family members to regroup and successfully continue caring
for a disabled individual at horne on a long-term basis.
Advocacy
Professionals need to be advocates for the family in the early stages and
work with the family in developing self-advocacy skills in later stages. Families
may continue to require assistance with advocacy from either the rehabilitation
team or other organized groups to obtain needed services. These may include
community mental health centers, centers for the elderly, or public school
systems, none of which may be experienced in dealing with brain-injured
survivors.
Family Therapy
For some family members, family therapy may be indicated. In situations
where family dynamics and roles were ineffective or maladaptive prior to the
injury, the injury can be devastating to the family unit. Even families with
good interaction patterns and adequate support prior to injury may find the
THE ROLE OF THE FAMILY 195
adjustment overwhelming and seek guidance. Traditional therapy goals are
applicable (e.g., increased communication, mobilization of support).
Clients often are placed a long distance from horne during some point
in their rehabilitation. This may preclude family therapy at the facility; how-
ever, families can be referred to therapists in their community. This not only
initiates the family therapy process, but also identifies a support system fol-
lowing discharge. Therapists need to be available on a long-term basis as
survivors will move in and out of crisis over long periods of time.
Support versus Therapy
It is important to differentiate between therapy and support. Rosenthai
and Young (1988) distinguish between supportive counseling and family
therapy by describing counseling as an assistive method to help families deal
with feelings ofloss and helplessness. Therapy is described as a process designed
to bring about a change in family functioning. Family members may require
supportive counseling throughout the recovery process and may not require
family therapy. On the other hand, family members requiring family therapy
will need professionals in that field with a knowledge of TBI. Solomon and
Scherzer (1991) present 31 guidelines for family therapists.
Intimacy
Brain-injured survivors often experience long-term "personality changes."
This has special implications for marital and sexual relationships. Even in
mild head injury, previous patterns of relating are often replaced, and the
new patterns may be unappealing to the spouse. In most cases, brain injury
results in reduced sexual drive (Zencius, Wesolowski, Burke, & Rough, 1990).
These changes in sexuality along with behavioral and cognitive sequelae com-
bine to alter the character ofintimacy.
A sex therapist may be weIl qualified to assist the couple with the physical
changes that have occurred as a result of TBI. The "personality changes,"
however, are often the most disruptive. Traditional marital therapists may or
may not have the experience with TBI necessary to address all of the com-
plicating variables. Careful selection of a therapist is imperative. While many
TBI rehabilitation programs will not employ sex therapists on their staff, the
case manager, nurse, or social worker should know qualified individuals in
this specialty who will accept TBI referrals. The relatively high rate of divorce
among brain-injured survivors and reports of marital dissatisfaction warrant
ongoing treatment and research.
196 CHAPTER 9
SUMMARY
Family Reactions to Head Injury
1. The family's reaction to head injury is influenced by characteristics
of the injured individual (current and premorbid), the pretrauma
characteristics ofthe family, and the nature and severity ofthe injury.
2. Stress and anxiety can result not only from the injury but also from
unfamiliar medical settings.
3. Families go through stages like the grieving process: shock, panic,
despair, and denial.
4. Professionals should engage in crisis intervention at this time.
Special Issues, Roles, and Players
5. The emotions displayed after head injury can be functional or dys-
functional depending on how they are used.
6. Members of the family may assurne maladaptive roles in that they
may promote dependency.
7. Spouses often find themselves in the role of caretaker which puts a
strain on marriage.
8. It is often better to place young adults in group hornes rather than
at horne where they may be made more dependent.
9. Siblings of clients are often neglected by parents and should be ed-
ucated about brain injury.
10. Children of clients may end up in the role of a caregiver.
11. Injured children may be overprotected.
12. Discharge can be traumatic for the family since this is when family
members realize the extent of the injured member's disability.
Assessment
13. Family assessment has five goals: to measure the level ofinvolvement,
identify roles, leam the level of adjustment, assess types of support,
and leam sources of stress.
14. There are three methods of family assessment: interview, question-
naires, and structured observation.
Family Services: Intervention/Integration
15. The development offamily services is based on three assumptions:
that families differ in premorbid abilities, that some families have
THE ROLE OF THE FAMILY 197
more resources, and that families require different interventions at
different stages of adjustment.
16. Families need education about TBI.
17. Families need to know about available resources.
18. Horne visits by clients should be therapeutic in that the family is
prepared for what to expect and trained to deal with any situation.
19. Horne visits should be an extension of the therapy given at the re-
habilitation facility.
20. Respite care is often needed by families to give them a chance to
"regroup. "
21. Professionals should continue contact with the family to provide
counseling and therapy when needed.
APPENDIXA
Performance Analysis
DOt1AIN: _________ _
ENVIRONt1ENT: _________ _
SUBENVIRONt1ENT: ________ _
SUBENV I RONt1ENT CLiENT
TASK ANALYSIS
INVENTORY BARRIER
OBJECTIVE
+/-
Activity:
SkilJs:
+/-
Activity:
Skills:
+/-
Activity:
Skills:
+/-
Activity:
Skills:
+/-
Activity:
Skills:
+/-
Activity:
Skills:
+/-
Activity
SkilJs: +/-
199
APPENDIX B
Practitioner Forms for Memory
1 ................................................ Blank Dally Schedule Form
:&. Weekly Schedule Form
.............................................. .Monthly Calendar
40 .............................................. JndlvlduaI loal .:heet
50 .............................................. Dally tournai and loal .:heet
............................................... .A llnment .:heet
, .............................................. .Notebook entry form
8 .............................................. .Memory checklist (one task)
9 ............................................... Memory checklist (multiple
ta.:k)
10 ............................................. Selimedlcatlon form
:1:1 ............................................. New people met form
201
202
APPENDIX B
________________ __
DATE ___________ _
7-B:00AM
B-9 :00AM
9-10 :ooAM
10-11 :00...,..
ll-12:ooN
12-1 :OOPM
I-2:00PM
2-3:OOPM
3-4 :OOPM
4-:5 :0OPM
5-6 :OOPM
6-7 :OOPM
7-B :ooPM
B-9 :ooPM
9-10 :OOPM
10-1 1
SCHEDUlED
ACl IV IIV VES /00
V N
y N
'( N
V N
V N
V N
V N
V N
'( N
'( N
'( N
V N
V N
V N
V N
'( N
ACTUAl
ACI IYITY
BEHAVIOR ___________________________________________________________ _
_______________________________________________________ ___
P.T ____________________________________________________________ _
O.T . _____________________________________________________________ _
________________________________________________________________ _
PRACTITIONER FORMS FOR MEMORY 203
TIME SUN MON TUES WEDN THUR FRI SAT
7:00am
B:OOllm
9:00am
IO:OOllm
I 1: 00am
12:00N
1:00pm
2:00pm
3:00pm
4:00pm
5-00pm
6:00pm
7:00pm
B:OOpm
9:00pm
204
APPENDIX B
MONTHL Y CALENDAR
MONTH OF: _______ _
Sundoy Mondoy Tuesdoy Wednesdoy Thursdoy Fridoy Soturdoy
I I I
C C I I
I I I I I I I
I I I I I I I
I I I I I I I
I I I I I I I
C- I r-- I r- I r-
WRITE DATE IN LOWER RIGHT HAND CORNER FOR EACH BOX.
NOTES:
1.} __________________ _
2J __________________ _
3J __________________ _
4J __________________ _
5J __________________ _
6.) __________________ _
7J
BJ, __________________ _
9.), __________________ _
10.) __________________ _
PRACTITIONER FORMS FOR MEMORY 205
NAME: __________ DATE: ___________ _
LIST TOUR SHORT TERM GOALS (TO OBTAIN WITHIN A WEEK)
1.) ____________________ _
2.> ____________________ _
3.)--------------------
4.> ____________________ _
5.>-------------------
6.> ___________________ _
7.> ____________________ _
.> ____________________ _
9.> ___________________ _
10.> ____________________ _
WHAT ARE TOUR LONG TERM GOALS? (LONGER THAN A WEEK)
1.)- -------------_____ _
2.> ____________________ _
3.>-------------------
4.> ___________________ _
5.>-------------------
6.) __________ _________ _
7.) ____________________ _
.> ___________________ _
9.> _ _________________ _
10.) _______ _____________ _
11.) ___________________ _
12.> ____________________ _
13.) __________________ _
14.> ____________________ _
15.>-----__________ _____ _
206
APPENDIX B
JOURNAL & GOAL REVIEW
TODATS DATE AND DAT: __________________ -'
L) What did you do today to meet youe goals? (eefee to goal sheet).
a->' ______________________ _
b-> _____________________ _
c-> _______________________ _
dJ ____________________ _
e-> _______________________ _
2.) Name one good thing you did today .
3.) What did you do this moening ?
4.) What did you do this afteenoon ?
5-> What could have you done to make today bettee ?
6.) What is on youe schedule foe tomoccow ?
7.) Name five people you inteeacted with today .
8.) List any appointments oe special events foe tomoeeow.
9-> Name two othee people in this geoup.
10.) What is on youe schedule foe this evening ?
PRACTITIONER FORMS FOR MEMORY
ASSIGNMENT SHEET
DATF.
ASS'--" __ .-
()UF: DATF.
207
COMPLETED
TES NO
0 D
0 D
0 D
0 D
SPECIAL INSTRUCTIONS: _________________ _
SPECIAL MATERIALS: __________________ _
208
APPENDIX B
DAILY NOTEBOOK ENTRIES
DATE MESSAGEIENTRT PERSON/PLACE COMMENTS
PRACTITIONER FORMS FOR MEMORY
TASK ________________________ __
STEPS
TRIALS ------';?
Date
209
210 APPENDIX B
DAllV TASKS CHECKLIST
TIME TASK CHECK-OFF
Comments
PRACTITIONER FORMS FOR MEMORY
211
SELF-MEDICATION CHECKLIST
MedicatioD _________ _ Dosage ________ ___
Medication _________ _ Dosage __________ ___
Medication _________ _ Dosage __________ ___
Medication _________ _
Dosage __________ ___
Date &
time Mon Tues Wedn Thur Fri Sat Sun comments
EMERGENCY NUMBERS
SPECIAL INSTRUCTIONS ___________________________________ __
212
APPENDIX B
PiOPLi I"Vi MiT FORM
-
.. ,. ..... N,. ..... W'it:h IWh,.t: dn t:ha" dn ? of
APPENDIXC
TBI Education Curriculum
TRAINING METHODOLOGY
Small Group Training
Training should occur in small groups (e.g., four to five dients). Small group
training offers several advantages. Group training can be a more efficient
instructional procedure compared to one-on-one training (how much material
is learned per unit of time). Group training offers an alternative teaching
strategy where one-on-one instruction is neither feasible nor efficient and
results in more dient-to-dient social interactions.
Instructional Method
Characteristics ofan individualized system ofinstruction should be used.
Individualized systems of instruction allow dients to proceed at their own
rates through units of course material with help from study guides. An ad-
ditional aspect of personalized systems of instruction is a unit perfection re-
quirement (e.g., before dients can move to the next unit they must master
the proceeding unit, demonstrated by a mastery quiz) (Keller, 1968).
Interspersal Training
This refers to reintroducing course material that was previously trained
with new course material (i.e., while learning new course material, course
material from the previous units is interspersed among the new material).
Maintenance of skills and information has been demonstrated in the past
through using this interspersal training technique (Neef et al., 1978). The use
of interspersal training is necessary with brain-injured dients due to the char-
acteristic memory deficits exhibited by the majority of brain-injured dients.
213
214
APPENDIX C
Instructional Units
We recommend training the brain-injured dient by progressing through
six distinct units. These six units are listed below and are sequenced in the
order in which training should occur. Apretest precedes training sessions and
a posttest follows completion of the last instructional unit. Programmed into
all six instructional units is information interspersed from previous units into
current instructional units. Thus, while dients are leaming about psychological
deficits they also review information on demographics and anatomy of
the brain.
Session 1
On the first day of dass, all dients begin with a written pretest. The
instructor hands out two forms of the pretest, distributing them in a random
fashion. Thus, if a dient receives test format "A" on the pretest, then this
dient would receive test format "B" on the posttest.
Sessions 2 and 3 (Unit #1)
These two sessions introduce dients to the demographies of TBI. The
frequency of TBI is higher among males, and injuries are frequently related
to alcohol abuse; the most common cause of TBI is automobile accidents.
Clients are asked to explain the conditions of their accident or cause of TBI.
Session 4 (Uni! #2)
This session outlines types of injury to the brain that can result from
accidents. Also, a review ofthe anatomy ofthe brain is briefly covered. Clients
are provided with maps of the brain for labeling parts and lobes. Clients are
also asked to identify what part of their brain was injured.
Sessions 5 and 6 (Uni! #3)
These two sessions outline resulting physical deficits from TBI. Some
examples of physical deficits outlined are as folIows: ambulatory balance dif-
ficulties, vision and taste inadequacies, alcohol intolerance, and seizure dis-
order. Clients are encouraged to list any physical deficits they may have ex-
perienced after their injuries.
TBI EDUCATION CURRICULUM 215
Sessions 7 and 8 (Uni! #4)
Psychological deficits are reviewed in these two sessions. Common psy-
chological deficits among TBI survivors are outlined. These include decreased
anger control and sexual disinhibition, feelings of loneliness, depression, and
apathy. Clients are asked to list psychological deficits within themselves.
Sessions 9 and 10 (Uni! #5)
Common cognitive deficits resulting from TBI are covered in this unit.
Some of the deficits covered include decreased attention and retrieving in-
formation and inability to store information in the memory. Clients are en-
couraged to list any cognitive changes in themselves since their injury.
Sessions 11 and 12 (Unit #6)
These two sessions review executive functions (i.e., the higher processes
ofthe brain that allow us to plan and to execute these plans). Specific infor-
mation reviewed is: goal formation, self-monitoring, self-initiation, problem-
solving, and organizing. Once again, clients are asked to identify deficits they
have regarding this area.
Session 13 (Uni! #7)
This entire session is used to review information covered in the six in-
structional units. Clients may independently read and answer workbook
questions or questions may be answered by the instructor.
Session 14 (Uni! #8)
The last session is used to administer the posttest. As previously men-
tioned, the posttest should differ from the pretest.
PRETEST
1. Traumatic brain injury refers to: (Circle one)
A. Trauma to the head that results in only psychological and physical
problems
B. Trauma to the head that results in physical, psychological, and
cognitive problems
216 APPENDIX C
C. A wound to the head which always leads to social problems
D. Trauma to the head that results in language and mathematics
deficits only
2. What other terms have been used to describe traumatic brain injury?
List two.
3. Overall, most people are injured in what season? (Circle one)
A. Spring
B. Summer
C. Fall
D. Winter
4. There are 13,500 persons surviving what severity of injury each year?
(Circle one)
A. Severe brain injury
B. Moderate brain injury
C. Mild brain injury
5. True or false: More men are injured each year than women.
6. Falls are reported to be the cause for: (Circle one)
A. The majority of head injuries
B. The second most common cause of head injury
C. The third most common cause of head injury
D. The fourth most common cause of head injury
7. Black people are more likely to have a head injury than white people
because ofpoor educational background. (Circle one)
A. True
B. False
C. Only in winter months
8. The hall mark of a closed head injury is: (Circle one)
A. An automobile accident
B. The head being struck by a heavy object
C. Violent and unnatural movement of the brain
D. Movement of the head and striking a stationary object
9. See Illustration 1 (label all pictures).
10. Damage to the frontal lobes results in: (Circle one)
A. Memory deficits
B. Taste and smell difficulties
C. Inability to plan
D. Sight difficulties
11. Damage to temporal lobes often leads to which problem?
A. Hearing difficulties
B. Problems retrieving stored information
C. Psychological problems leading to psychosis
D. Problems socializing with others
TBI EDUCA TI ON CURRICULUM
217
Label the following diagrams using the following terms: contu-
sion, coup' concussion, contra coup' concussion, and normal.
218
APPENDIX C
12. See Illustration 2 (label two lobes ofthe brain).
13. Circle the correct definition oflong-term or distant memory.
A. Recall of events that happened "s" seconds ago
B. Recall of events that happened several hours ago
C. Recall of events that happened days to years ago
D. Recall of events that happened over "s" years ago
14. True or false: Things are easier to remember ifthey are tied to our
emotions or senses.
1. ____ _
3. ____ _
Medulla
(lower bram)
Lobes of the Brain
2. ___ _
Cerebellum
TB! EDUCA nON CURRICULUM 219
15. True or false: Memory problems usually disappear after one to two
years of therapy.
16. Which is not a physical deficit that some head-injured people have?
(Circle one)
A. Problems walking
B. Difficulty speaking
C. Reoccurring halitosis
D. Poor balance
17. Which ofthe following refers to cognitive deficits? (Circle one)
A. Psychological imbalance
B. Continual chest pain
C. Attention and problem-solving deficits
D. Social and psychological deficits
18. Which is a psychological deficit some head-injured people have?
(Circle one)
A. Psychological shutdown
B. Neurological instability
C. Impulsivity
D. Gastrointestinal problems
19. Which type of head injury is characterized by a coma length of an
hour to several hours? (Circle one)
A. Catastrophic head injury
B. Severe head injury
C. Mild head injury
D. Moderate head injury
20. What type of head injury is characterized by a coma that lasts for
days? (Circle one)
A. Catastrophic head injury
B. Severe head injury
C. Mild head injury
D. Moderate head injury
21. Recovery from a head injury: (Circle one)
A. Never really occurs
B. Occurs only when the individual is aware ofthe injury
C. Occurs within one to ten years
D. Varies according to the individual
22. Which is the best indicator of long-term recovery? (Circle one)
A. Age and personality type
B. Income and education
C. Family support and community support
D. Age at injury and job experience
220
APPENDIX C
Homework Assignment Form 1
Completed by Group Leader: _______ _
Leader Oient
Date
Due Date
Action Required: ____________________ _
With Whom: ___________________ _
Where: _________________________ ___
When: ___________________________________ _
Task Analysis:
Step 1: ____________________________________ _
Step 2: ______________________ _
Step 3: _______________________ _
Completed by Client:
Action completed with whom and where: ___________ _
Outcome: _____________________________ ___
Whatworked: __________________________________ __
What didn't work: _________________________________ _
Future plan: __________________________________ _
Homework Assignment Form 2
Group Title
Assignment:
Date Due Date
Action(s): _________________________________ _
With whom: ___________________________ ___
Where: ________________________________ ___
Outcome:
Whatworked: ________________________ __
TBI EDUCATION CURRICULUM 221
What didn't work: __________________ _
Future plan: _____________________ _
PRETEST ANSWER KEY
1. B
2. Head injury, brain injury, open head injury, closed head injury
3. B
4. A
5. True
6. B
7. False
8. A or C
9. Upper left -+ coup concussion; upper right -+ contusion; lower left -+
normal; and lower right -+ contra coup concussion
10. C
11. B
12. 1 = Frontal, 2 = Parietal, 3 = Temporal, 4 = Occipital
13. C
14. True
15. True
16. C
17. C
18. C
19. D
20. B
21. D
22. C
APPENDIXD
Social Skills Curriculum
Name' ____________________ ___
1.) Following Instructions
2.) Accepting Criticism
3.) Accepting -NO
4.) Solving Problems
5.) Giving Feeclback
6.) Complimenting Tourself
7 -> Requesting Permission
6-> Expressing Appreciation
9.) Giving Compliments
10.) Being Assertive
1 L) Accepting Compliments
12.) Asking for Help
13.) Reporting Whereabouts
14.) Acknowteclge a Guest
15.) Disagree Appropriately
16-> Introclucing Tourself
1 7 J Departing Ski11s
16.) Conversation Ski11s
19J Volunteering to Help
20.) Interrupting Appropriately
pre/
223
224
APPENDIX D
TASK ANALYSiS FOR INDIVIDUAL SOCIAL SKILLS
NAMi ____________________ __
U FOLLOWING INSTRUCTIONS
a.) Maintain eye contact
b.) Acknowledge request
c,) Follow instructions (do task etc')
d.) Check back when completed
2.) ACCEPTING CRITICISM (ROUTINE)
a.) Maintain eye contact
b.) Acknowledge criticism (say ok)
c.) Don't argue, pout or threaten
d.) It you disagree, let them finish
speaking & then discuss in calm voice
3) ACCEPTING NO FOR AN ANSWER
a.) Maintain eye contact
b,) Acknowledge NO
c.) Don't argue,whine, pout or swear
d,) If you don't understand why
calmly ask tor a reason
4,) SOLVING PROBLEMS RATIONALLY
a.) Wait tor appropriate time to express
grievance (after class, work, etc.l.
b.) Maintain eye contact
c.) State your problem without yelling
d.) Begin with a positive suggestion
e.) Offer a solution or solutions
5.) GIVING POSITIVE & CORRECTIVE FEEDBACK
a,) Begin with a smile, joke or nice greeting
b.) Tell the person exact1y what he has done.
Describe in non threatening way
c.) Describe the appropriate waY
d.) Tell person why to use the appropriate way
e,) Ask the person if they understand
f.) Thank the person for listening
111111111111
-
=
-
-
-
-
SOCIAL SKILLS CURRICULUM
6) COMPLIMENTING YOURSELF
a,) Express appreciation tor belonging to
a group, activity, etc,
b,) Don't brag
c,) Don't make negative statements
7) REQUESTING PERMISSION
a) Ask permission, don't demand
b,) Ask the appropriate person who
can grant you permission
c,) Say "Thank you" regardless
8) EXPRESSING APPRECIA TlON TO OTHERS
a) When people help you or offer to help
you say "Thankyou"
b.) Maintain eye contact
g) EXTENDING COMPLIMENTS
a,) Greet the person ('A'ith smile, handshake
b) Compliment others tor something they
did well, a skill, job, etc
10) BEING ASSERTIVE APPROPRIATELY
a,) Remain ca Im, don't argue or raise voice
b,) State your grievance in clear fashion
c) Wait to discuss grievance or request in
a situation alone,
d.) Use "I" statements
e) Express "Thanks" for listening
I U ACCEPTING COMPLIMENTS
a.)Maintain eye contact
b) Express appreciation (thank you)
c) Don 't deny the compliment
12) ASKING FOR HELP
a) Approach person & say "Excuse me"
b) Ask person for a favor or help
c.) Specify what you need help 'A'ith
d.) Say "Thank you" regardless or their
response
225
-
I
----
-
-
-
226
13.) REPORTlNG YOUR WHEREABOUTS
a.) Request permission
b.) When given permission, state where
you are & when you Will be back
c.) Return on time
d.) If late, request additional permission
14.) ACKNOWLEDGE A GUEST
a.) Stop what your are doing, stand up
b.)Greet the guest
c.) Open the door for others when you can
d.) Keep eye contact & good voice level
15.) DISAGREE APPROPRIATELY
a.) Ask to speak to person, remain calm
b.) State disagreement, in specific & "I" terms
c.) Keep eye contact & pleasant voice
d.) Offer possible solutions
e.) If solutions are not accepted, remain calm
and discuss issue With another individual
16.) INTRODUCING YOURSELF
a.) Look at person and smile
b.) Say "Hello, my name is ......
c.) Invite them to come in, talk, etc.
d) Follow-up With "May I help you", etc.
17.) DEPARTURE SKILLS
a.) Say "It was nice to meet or see you"
b) Walk guest to door, shake hands
18.) CONVERSATION SKILLS
a.) Respond when spoken to by others
b) Maintain eye contact & smile
c.) Give complete answers not yes/no
19.) VOLUNTEERING TO HELP
a.) Ask person "Can I help you"
b.) Help person With task, problem, etc.
c.) Inform them it was your pleasure to help
20.) INTERRUPTING APPROPRIATELY
a.) Say "Excuse me" before talking
b.) Wait for a response before talking
c.) Say "Im sorry for interrupting but ......
d.) Provide information
e.) Say "Thank you for listening"
APPENDIX D
I I I I I I
I I I I
I I I I
I I I J
I I I I
-
APPENDIX E
Horne Trip Observation Scale
To facilitate therapeutic horne trips, it is imperative to specify desired behaviors
to be observed and measured during the dient's therapeutic horne visit. The
attached observation scale is meant to be tailored to each dient prior to his
or her trip horne. Skills or areas of assessment should be behaviorally specific
and detailed under each functional area (identified on instrument as A, B, or
C). Family members should be instructed in the observation ofthe behaviors
prior to the dient's trip horne and questions answered upon his or her leaving
the horne. Specific techniques should be thoroughly taught to accompanying
family members prior to their departure from the rehabilitation facility. This
may involve preteaching long distance via telephone, modeling and coaching
upon the family's arrival at the facility, and follow-up upon the dient's return.
227
228 APPENDIX E
OBSERVATION SCALE
Name: ______________________________________________ ___
Date: ________________________________________________ _
To provide the best possible treatment, it is essential for us to know how your
family member uses the skiHs he or she learned at in his or her
horne environment. Please compare functioning to the last time you spent a
significant amount of time with hirn or her.
How to rate:
Much worse 1
Not as weH as before 2
Same 3
Improved 4
Much improved 5
Please circle the correct answer:
1. Daily Living Skills
a. 2 3 4 5
b. 2 3 4 5
c. 2 3 4 5
Other 2 3 4 5
2. Beha vior /Psychosocial
a. 2 3 4 5
b. 2 3 4 5
c. 2 3 4 5
Other 2 3 4 5
3. Medical
a. 2 3 4 5
b. 2 3 4 5
c. 2 3 4 5
4. Communication/Socialization
a. 2 3 4 5
b. 2 3 4 5
c. 2 3 4 5
Other 2 3 4 5
5. Vocational
a. 2 3 4 5
b. 2 3 4 5
c. 2 3 4 5
Other 2 3 4 5
HOME TRIP OBSERVATION SCALE 229
6. Physical
a. 2 3 4 5
b. 2 3 4 5
c. 2 3 4 5
Other 2 3 4 5
7. Cognitive
a. 2 3 4 5
b. 2 3 4 5
c. 2 3 4 5
Other 2 3 4 5
Other Observations:
The length of the visit: ______ ,days
Filled out by: _____________________ _
Relationship to dient: __________________ _
References
Ayllon, T., & Azrin, N. (1968). The token economy: A motivatirmal system/or therapy and re-
habilitation. New York: Appleton-Century-Crofts.
Azrin, N. H. (1967). Pain and aggression. Psychology Today. }, 27-33.
Azrin, N. H. (1970). Punishment of elicited aggression. Journal 0/ the Experimental Analysis or
Behavior, 14,7-10.
Azrin, N. H., & Wesolowski, M. D. (1975). Eliminating habitual vomiting in a brain injured
adult by positive practice and self-correction. Journal of Behavior Therapy and E>::perimental
Psychiatry, 6, 145-148.
Bakay, L., & Glasauer, F. E. (1980). Head in jury. Boston: Little, Brown, and Company.
Benton, A. L. (1979). Behavioral consequences of closed head injury. In G. L. Odem (Ed.),
Central nervous system trauma status report (pp. 220-231). Bethesda: National Institute of
Neurological and Communicative Disorders and Stroke.
Ben-Yishay, Y. (Ed.). (1981). Working approach es to remediation 0/ cognitive deficits in brain
damaged persons (Rehabilitation monograph No. 62). New York: New York University
Medical Center, Institute of Rehabilitation Medicine.
Ben-Yishay, Y., & Diller, L. (1983). Cognitive remediation. In M. Rosenthai, E. Griffith, M.
Bond, & D. Miller (Eds.), Rehahilitation o/the head injured adult (pp. 367-380). Philadelphia:
Davis.
Bishop, D. S., & Miller, I. M. (1988). Traumatic brain injury: Empirical family assessment tech-
niques. Journal o/Head Trauma Rehabilitation, 3, 16-30.
Black, P., Jeffries, J., Blumer, D., Wellner, A., & Walker, A. (1969). The post-traumatic syndrome
in children. In A. Walker, E. Caveness, & M. Critchley (Eds.), The late effects o!head injllry.
New Y ork: Raven Press.
Blackerby, W. F. (1987). Disruption or sexuality /ollowing a head injury. Framingham, Mass.:
National Head Injury Foundation.
Blackerby, W. F. (1988). Head injury rehabilitation: Sexuality after TBI. In W. H. Burke, M.
Wesolowski, & W. F. Blackerby (Eds.), The HDI professional series on trallmatic brain
injurv. Houston: HDI Publishers.
Boiler, F., & Frank, E. (1982). Sexual dys/unction in neurological disorders: Diagnosis, management,
and rehabilitation. New Y ork: Raven Press.
Brooks, D. N., & McKinlay, W. (1983). Personality and behavior change after severe blunt head
injury, a relative's view. Journal 0/ Neurology, Neurosurgery, and Psychiatry, 46, 336-344.
Brown, B., & McCorrnick, T. (1988). Family coping following traumatic brain injury. Family
Relations, 37, 12-16.
231
232 REFERENCES
Burke, W. H., & Lewis, F. D. (1986). Management of maladaptive social behavior of a brain
injured adult. International Journal of Rehabilitation Research, 9, 335-342.
Burke, W., & Wesolowski, M. D. (1988). Applied behavior analysis in head in jury rehabilitation.
Houston: HDl Publishers.
Burke, W., Wesolowski, M. D., & Guth, M. (1988). Comprehensive head injury rehabilitation:
An outcome evaluation. Brain Injury, 2,313-322.
Burke, W.,Wesolowski, M. D., Buyer, D., & Zawlocki, R. (1990). The rehabilitation ofadolescents
with traumatic brain injury: Outcome and follow-up. Brain Injury, 4, 371-378.
Burke, W. H., Zencius, A. H., Wesolowski, M. D., & Doubleday, F. (1991). Improving executive
function disorders in brain injured c1ients. Brain Injury, 5, 241-252.
Camp, 8., & Bash, M. (1981). Think aloud. Champaign, III.: Research Press.
Cartlidge, N., & Shaw, D. A. (1981). Head in jury. Philadelphia: Saunders.
Cooper, J., Heron, T., & Heward, W. (1987). Applied behavior analysis. Columbus, Ohio: Merrill.
Corrigan, J. D., Amett, J. A., Houch, L. J., & Jackson, R. D. (1985). Reality orientation for brain
injured patients: Group treatment and monitoring ofrecovery. Archives ofPhysical Medicine
and Rehabilitation, 66, 626-630.
Craighead, W. E., Kazdin, A. E., & Mahoney, M. (1981). Behavior modification: Principles,
issues, and applications. Boston: Houghton Milin.
Craine, J. F., & Gudeman, H. E. (Eds.) (1981). The rehabilitation ofbrainfunction: Principles,
procedures, and techniques of Neurotraining. Springfield, IL: CharIes C. Thomas.
Crossen, 8. (1987). Treatment of interpersonal deficits for head-trauma patients in inpatient
rehabilitation settings. The Clinical Neuropsychologist, 4, 335-352.
Diller, L. (1976). Model for cognitive retraining in rehabilitation. The Clinical Psychologist, 29,
13-15.
Diller, L., & Gordon, W. (1981). Interventions for cognitive deficits in brain injured adults.
Journal of Consulting and Clinical Psychology, 49, 822-834.
Dougherty, P., & Radomski, M. (1987). Memory notebook training: Section three. Cognitive
rehabilitation workbook. Rockville, MD: Aspen Publishers.
Ducharme, S. (1987). Sexuality and physical disability. In B. Caplan (Ed.), Rehabilitation psychology
desk reference (pp. 419-435). Rockville, Md.: Aspen.
Faglioni, P., Spinnler, H., & Vignolo, L. (1969). Contrasting behavior of right and left hemisphere
damaged patients in a discriminative and a semantic task of auditory recognition. Cortex,
5,366-389.
Ferguson, J. M. (1975). Learning to eat: Behavior modificationfor weight control. Palo Alto: Bull.
Fisher, J. M. (1985). Cognitive and behavioral consequences of c10sed head injury. Seminars in
Neurology, 5, 3.
Foreyt, J. P., & Kondo, A. T. (1985). Eating disorders. In P. H. Bornstein & A. E. Kazdin (Eds.),
Handbook of clinical behavior therapy with children. Homewood, III.: Dorsey Press.
Foxx, R. M., Marchard-Martella, N. c., Martella, R. c., Braunling-McMorrow, D., & McMorrow,
M. J. (1988). Teaching a problem solving strategy to c10sed head injured adults. Behavioral
Residential Treatment, 3, 193-208.
Glitsky, E. L., & Schacter, D. L. (1988). Remediation of organic memory disorders: Current
status and future prospects. Journal of Head Trauma Rehabilitation, 1, 54-63.
Guare, R., Dawson, M., & Warren, S. O. (1988). Managing attention deficits. Houston: HDI
Publishers.
Guare, R., Samson, M., Guth, M., Warren, S., & Burke, W. (1988). Developing the TBI reha-
bilitation plan. Houston: HDI Publishers.
Guth, M. L., Lasseter, S. A., & Harward, M. (1988a). The role ofthe family in TBI rehabilitation.
Houston: HDI Publishers.
REFERENCES
233
Guth, M. L., Wesolowski, M. D., & Burke, W. H. (1988b). Increasing self-awareness. Houston:
HDI Publishers.
Hacaen, H., & Ajuriaguerra, J. (1964). Lefi handedness, manual dexterity, and cerebra I dominance.
New York: Grune & Stratton.
Hall, S. M. (1972). Self-control and therapist control on the behavioral treatment of overweight
women. Behaviour Research and Therapy, 10, 59-68.
Harris, J. (1980). Memory aids people use: Two interview studies. Memory and Cognition, 8, 31-
38.
Hawkins, R. P., & Dobes, R. W. (1977). Behavioral definitions in applied behavior analysis:
Explicit or implicit? In B. Etzel, J. LeBianc, & D. Bear (Eds.), New developments in hehavioral
research. Hillsdale, N.J.: Erlbaum.
Heilman, K. M., & Valenstein, E. (1979). Clinical neuropsychology. London: Oxford University
Press.
Hopewell, A., Burke, W., Wesolowski, M., & Zawlocki, R. (1990). Behaviorallearning therapies
for the traumatically brain injured patient. In R. L. Wood & l. Fussey (Eds.), Cognitive
rehabilitation in perspective. London: Taylor & Francis.
Horton, A. M. (1979). Behavioral neuropsychology: A clinical case study. Clinical Neuropsychology,
1.20-23.
Horton, A. M. (1981). Behavioral neuropsychology in schools. School Psychology Review, 10,
367-372.
Horton, A. M., & Wedding, D. (1984). Clinical and behavioral neuropsychology. New York:
Praeger.
Jennett, B., & Teasedale, G. (1981). Management oJhead injuries. Philadelphia: Davis.
Jennett, B., Snoek, J., Bond, M. R., & Brooks, N. (1981). Disability after severe head injury:
Observations on the use ofthe Glasgow Outcome Scale. Journal oJNeurology, Neurosurgery,
and Psychiatry, 44, 285-293.
Keller, F. S. (1968). Good-bye teacher. Journal oJ Applied Behavior Analysis, 1,79-89.
Kosteljanetz, M., Jensen, T. S., Norgard, B., Lunde, l., Jensen, P. B., & Jensen, S. G. (1981).
Sexual and hypothalamic dysfunction in the postconcussional syndrome. Acta Neurologica
Scandinavica, 63, 169-180.
Levin, H. S., Benton, A. L., & Grossman, R. G. (1982). Neurobehavioral consequences oJ closed
head in jury. London: Oxford University Press.
Lewis, F., Burke, W., & Carrillo, R. (1987). Model for rehabilitation of brain injured adults in
the post-acute setting. Journal oJ Applied Rehabilitation Counseling, 18, 39-45.
Lezak, M. D. (1978). Living with the characterologically aitered brain-injured patient. Journal oJ
Clinical Psychology, 39, 592-598.
Lezak, M. D. (1983). Neuropsychological assessment (2nd ed.). London: Oxford University Press.
Livingston, M., & Brooks, D. (1988). The burden on families of the brain injured: A review.
Journal oJ Head Trauma Rehabilitation, 3, 6-15.
Luria, A. R. (1966). Higher corticalfunctions in man. New York: Basic Books.
Luria, A. R. (1969). The mind or a mnemonist. New York: Basic Books.
Luria, A. R. (1973). The working brain. New York: Basic Books.
McFall, R. M. (1982). A review of reformation ofthe concept of social skills. Behavioral Assessment,
4, 1-33.
Mack, J. L. (1986). Clinical assessment of disorders of attention and memory. Journal oJHead
Trauma Rehabilitation, 1, 22-34.
McKinley, W., & Hickox, A. (1988). Family response to childhood traumatic brain injury. Journal
oJHead Trauma Rehabilitation, 3, 64-72.
234
REFERENCES
Malkmus, D., Booth, B. J., & Kodimer, L. (1980). Rehabilitation oJ the head injured adult:
Comprehensive cognitive management. Downey, Calif.: Professional Stalf Association of
Rancho Los Amigos Hospital.
Meichenbaum, D., & Goodman, J. (1971). Training impulsive children to talk to themselves: A
means of developing self-control. Abnormal Psychology, 77, 115-126.
MilIer, B. L., Cummings, J. S., Mclntyre, H., & Ebers, G. M. (1986). Hypersexuality or altered
sexual preference following brain injury. Journal oJ Neurology, Neurosurgery, and Psychiatry,
49, 873-876.
Morris, R. J. (1985). Behavior modijication with exceptional children: Principles and practices.
Glenview, 111.: Scott, Foresman.
National Head Injury Foundation. (1992). The silent epidemic. Framingham, Mass.
National Institute ofNeurologicai and Communicative Disorders and Stroke. (1976). In N. Cart-
lidge & D. Shaw, Head injury. Philadelphia: Saunders.
Neef, N., Iwata, B., & Page, T. (1978). Public transportation training: In vivo versus c1assroom
instruction. Journal oJ Applied Behavior Analysis, 11, 331-344.
Posner, M. T., & Rafal, R. D. (1987). Cognitive theories of attention and the rehabilitation of
attentional deficits. In Meir, A. Benton, & L. Diller (Eds.), Neuropsychological rehabilitation
(pp. 182-202). Edinburgh: Churchill Livingstone.
Premack, D. (1959). Toward empirical behaviorallaws: I. Positive reinforcement. Psychological
Bulletin, 66, 219-233.
Prigatano, G. P., & Others (1986). Neuropsychological rehabilitation after brain injury. Baltimore:
The Johns Hopkins University Press.
Quinn, S., Pierce, I. P., & Lyle, D. M. (1988). Relatives as play-therapists for the severely head
injured. Brain Injury, 3, 139-149.
Rosenthai, M., & Young, T. (1988). Elfective family intervention after traumatic brain injury:
Theory and practice. Journal oJ Head Trauma Rehabilitation, 3, 42-50.
Rotatori, A. F., & Fox, R. (1980). The elfectiveness of a behavioral weight reduction for moderately
retarded adolescents. Behavior Therapy, 11, 410-416.
Satz, P., & Fletcher, J. M. (1981). Emergent trends in neuropsychology: An overview. JournaloJ
Consulting and Ctinical Psychology, 49, 851-865.
Sidman, M. (1960). Tactics oJscientijic research. New York: Basic Books.
Solomon, c., & Scherzer, P. (1991). Some guidelines for family therapists working with the trau-
matically brain injured and their families. Brain In jury, 5, 253-266.
Struss, D., & Benson, D. (1984). Neuropsychological studies ofthe frontal Lobes. Psychological
Bulletin, 95, 328.
Stuart, R. B. (1969). Behavioral control of overeating. Behaviour Research and Therapy. 5, 357-
365.
Stuart, R. B., & Davis, B. (1972). Stim chance in a Jat world: Behavioral control oJ obesity.
Champaign, IlI.: Research Press.
Suinn, R. M. (1975). Anxiety management training for general anxiety. In R. Suinn & R. Weigel
(Eds.), The innovative therapy: Creative and clinical contributions. New York: Harper &
Row.
Suinn, R. M., & Richardson, F. (1971). Anxiety management training: A non-specific behavior
therapy program for anxiety control. Behavior Therapy, 4, 498.
Szekeres, B. F., Ylvisaker, M., & Cohen, S. B. (1987). A framework for cognitive rehabilitation.
In M. Yilvisaker & E. M. Gobble (Eds.), Community reentry Jor head injured adults. Boston:
College Hili Press.
Tawney, J., & Gast, D. (1984). Single subject research in special education. Columbus, Ohio:
Charles E. Merrill.
REFERENCES
235
Teasedale, G., & Jennett, B. (1974). Assessment of coma and impaired consciousness: A practical
scale. Lancet. 2. 81-84.
Thompson, L. (1974). The patient with severe head injury and his family. Scandinavian Journal
olRehabilitation Medicine, 6, 180-183.
Tuerk, K., Fish, 1., & Ransohoff, J. (1975). Head injury. In S. Arieti (Ed.), American handbook
ofpsychiatry (2nd ed.). New York: Basic Books.
Turner, 1., Green, G., & Braunling-McMorrow, D. (1990). Differential reinforcement oflow rate
responding (DRL) to reduce dysfunctional social behaviors in a brain injured man. Behavioral
Residential Treatment, 5, 15-27.
Valentich, M., & Gripton, J. (1986). Facilitating the sexual integration ofthe head-injured person
in the community. Sexuality and Disability, 7, 28-42.
Voganthaler, D. (1987). An overview of head injury: Its consequences and rehabilitation. Brain
Injury, 1,113-127.
Waaland. F., & Kreutzer, J. (1988). Family response to childhood traumatic brain injury. Journal
ofllead Trauma Rehabilitation, J, 51-63.
Wesolowski, M. D. (1987). Differences in the social networks of rehabilitation clients versus non-
c1ients. Rehahilitation Counseling Bulletin, Jl, 17-27.
Wesolowski, M. D., & Burke, W. H. (1988). Behavior management techniques. In P. M. Deutsch
& K. Fralish (Eds.), Innovations in head in jury rehabilitation. New York: Matthew Bender.
Wesolowski. M. D., & Deichmann. J. (1980). Physiological activity and attitudes toward disabled
persons. Rehabilitation COllnseling Bulletin, 23, 218-226.
Wesolowski, M. D., & Zawlocki, R. J. (1985). Stereotyped movement disorders. In P. Bornstein
& A. Kazdin (Eds.), llandhook o/clinical behavior therapy with childrell. Homewood, 111.:
Dorsey Press.
Wesolowski, M. D., & Zencius, A. H. (1992). Treatment of aggression in a brain injured adolescent.
Behavioral Residential Treatment. 7, 205-2 10.
Wesolowski, M. D .. & Zencius, A. H. (1993). Effects offeedback and behavior contracts on head
trauma persons inappropriate sexual behavior. Behavior Therapy.
Wesolowski, M. D., Zencius, A. H., & Burke, W. (1988). Developing motivation in head-injured
person.\. Houston: HDI Pub1ishers.
Williams, R. D .. & Gentry. W. D. (1977). Behavioral approach es to medicaltreatment. Cambridge,
Mass.: Ballinger.
Wood, R. (1988). Management ofbehavior disorders in a day treatment setting. Journal ofHead
Trauma Rehabilitation, J, 53-61.
Zahara, D., & Cuvo, A. (1984). Behavioral applications to the rehabilitation of traumatically
brain injured patients. Clinical Psycho!ogy Review, 4, 477-481.
Zeigler, E. (1987). Spouses of persons who are brain injured: Overlooked victims. Journal of
Rehabilitation, 45, 50-53.
Zencius, A. H., & Wesolowski, M. D. (1989). Control ofseizures in the treatment of a elient with
a brain injurv. Paper presented at the Eighth Annual National Head Injury Foundation
Symposium, Chicago.
Zencius, A. H., & Wesolowski, M. D. (1990). Using stress management to decrease inappropriate
behavior in a brain injured adult. Behavioral Residentia! Treatment, 5, 6 I -64.
Zencius, A. H., & Wesolowski, M. D. (1991). Reducing verbal aggression in adults with brain
injury. Behaviora! Residentia! Treatment, 6, 155-164.
Zencius, A., Wesolowski, M. D., Burke, W. H., & McQuade, P. (1989). Antecedent control in
the treatment of brain-injured c1ients. Brain Injury, J, 199-205.
Zencius, A. H., Wesolowski, M. D., & Burke, W. H. (1989). Comparing motivational systems
with two non-compliant head injured adolescents. Brain Injury, J, 67-71.
236
REFERENCES
Zencius, A., Wesolowski, M. D., & Burke, W. H. (1990a). A comparison offour memory strategies
with traumatically brain-injured adults. Brain Injury, 4, 33-38.
Zencius, A., Wesolowski, M. D., & Burke, W. H. (l990b). The use ofa visual cue to decrease
profanity in a brain-injured adult. Behavioral Residential Treatment, 3, 143-147.
Zencius, A. H., Wesolowski, M. D., Burke, W. H., & Hough, S. (l990c). Managing hypersexual
disorders in brain-injured clients. Brain Injury, 4, 175-181.
Zencius, A., Wesolowski, M. D., & Burke, W. H. (1991). Memory checklist: A method ofteaching
functional skills to brain damaged adults. Behavioral Residential Treatment, 6, 1-10.
Zencius, A., Wesolowski, M. D., Krankowski, T., & Burke, W. H. (1991). Memory notebook
training. Brain Injury, 5, 321-326.
Zencius, A. H., Wesolowski, M. D., & Lane, I. (1991). Assessing and treating noncompliance in
head injured persons. Brain Injury, 5, 288-295.
Index
A-B-A-B designs, 23; see also Reversal
designs
Acronym formation, 81
Advocacy, 194
Aggression, 132-140
causes of, 132
treatment of, 134-140
Alarms, as cuing devices, 105
AIternating treatments design, 27; see also
Multielement designs
Antecedents, 11, 21
control of, 99, 105, 129, 168
Anosognosia, 106-110; see also Denial, Self-
awareness
Applied behavior analysis, 11-30; see also
Behavior analysis
Assessments
c1inical, 35, 138
horne, 188
situational, 39
See also Situational evaluation
Assistive devices, 167-169
Association, 84
Attendance, 124, 130
Attention deficits, 99-105
Baseline, 16, 24
Behavior analysis, 11-30; see also Applied
behavior analysis
Behavior contracts, 128, 147, 173; see also
Contracts
Behavioral deficits, 12
Behavioral excesses, 12
Behavioral medicine, 167
Behavioral neuropsychology, 5-7
Bulimia, 174; see also Vomiting; Weight loss
Checklists, 86, 88, 102, 103, 115, 158
daily chores, 88
memory checklists, 89
planning checklists, 115
self-monitoring, 103
Children, 186
Chunking, 82
Coaching, 66
Cognitive deficits, 79-120
Cognitive retraining, 80-86
Coincidental teaching, 58
Community meeting, 56
Compensatory strategies, 86-96
Compliance, 121-131; see also
Noncompliance
Consequences, 11,21,99,104,109,122
management of, 122, 135, 168
natural, 109
Contingencies, II
Contracts, 128, 147, 171, 173, 175; see also
Behavior contracts
Cooking assessment, 42
Cuing devices, 92, 105
Daily routine, 51, 52, 69
Denial, 105-1 10; see also Anosognosia, Self-
awareness
Diabetes, 178
Differential reinforcement of incompatible
behavior (DRI), 171, 174
237
238
Differential reinforcement oflow rates of
responding (DRL), \35
Differential reinforcement of other behavior
(DRO), 171, 174
Discharge, 188
Duration, 16
by occurrence, 16
total, 16
Education, 191, 215
Emotion, 184
Empirical evaluation, 23
Environmental design, 132
Environmental restructuring, 95, 100, 132
Environment performance analysis, 98, 199
Epidemiology, I
Executive functions, 1\3-114
Experimental designs, 23-27
Extinction, 133, 170, 172, 173, 174, 177; see
also Planned ignoring
Family
dynamics, 182
role of, 181-196
services, 190
therapy, 194
Feedback, 67, 104, 113, 117, 136, 143, 144,
147, 152, 154, 159
contingent, 154
scheduled, 144, 154
videotaped, 104, 109, 136
Row sheets, 112
Frequency, 16,20
Functional analysis, 21, 99
Generalization, 12
Gestural prompt, 19
Graphing behavior, 19
Growth/Development, 187
Group training, 60, 96, 106, 107, 108, 110,
112,114,117,125,151,158,216
current event, 112, 117
dating skil1s, 140
goal and journal, 108
orientation, 96
personal adjustment, 107
planning, 114
point systems, 125
problem solving, 110
psychotherapy, 158
routines, 60
Group training (Cont.)
social skilIs, 15 I
TBI education, 106,216
Guiding observation, 64
Horne trip observation scale, 227
Horne visits, 192
Hypochondriacal statements, 173
Impulsivity, 158-163
Incidental teaching, 57
Incompatible behavior, 13
Integration, 108, 190
INDEX
Interpersonal skil1s training, 149-158; see
also Social skil1s training
Interspersal training, 107,216
Intervention, 12
Intimacy, 195
Latency, 17
Laundry assessment, 43
Maintenance ofbehavior, 107, 177
Maps, \30
Marital issues, 185
Memory checklists, 86, 89
Memory loss, 79
Memory notebook training, 88-92
Memory practitioner forms, 20 I
Modeling, 19,65,71,87,89,112,116,143,
147, 152
Momentary time sampling, 17
Motivational systems, 152, 171; see also
Point systems; Token economy
Multielement designs, 27; see also
Alternating treatments design
Multiple baseline designs, 24-26
across behavior, 25
across setti ngs, 25
across clients, 26
Natural environment, 32
Negative reinforcement, 121, 122, 132
Neuropsychology, 5-7; see also Behavioral
neuropsychology
Neurotraining, 4
Noncompliance, 121-131
Obesity, 176
Operant behavior, 169
Operant seizures, 169
INDEX
Operational definition, 13-15; see also
Response definition; Topography
Orientation problems, 96-99
group treatment of, 96
individual treatment of, 97
Overlearning, 104
Pain
as a cause of aggression, 133
complaints of, 173
See also Hypochondriacal statements
Partial interval recording, 18
Personalized system ofinstruction, 107,215;
see also Self-paced instruction
Physical prompting, 19
Pictures, 131
Planned ignoring, 170, 172, 173, 177; see
also Extinction
Planned teaching, 57
Planning skins, 113-117
Point systems, 123, 125, 152, 171
group point systems, 125
individualized point systems, 123
See also Motivational systems; Token
economy
Positive reinforcement, 121. 122, 132
Preexisting issues, 185
Premack principle, 122
Preteaching, 157, 162
Problem solving, 110-113
Profanity and swearing, 94; see also Verbal
abuse
Prompts, number of, 19
Psychotherapy, 158
Punctuality, 94; see also Compliance;
Unauthorized breaks
Redirection, 66, 138
Rehabilitation plan, 31-48
Reinforcement, 72, 133, 173, 175, 177; see
also Negative reinforcement; Positive
reinforcement
Relaxation techniques, 139; see also Stress
management training
Respite care, 194
Response cost, 123, 135
Response definition, 13-15; see also
Operational definition; Topography
Reversal designs, 23; see also A-B-A-B
design
Rhyme formation, 85
Seizures, 169; see also Operant seizures
Self-awareness, 105-110; see also
Anosognosia; Denial
Seif-monitoring, 102, 146, 160, 175
Self-paced instruction, 215; see also
Personalized system of instruction
Self-recording, 160
Self-talk, 102
Severity of injury, 182
Sexual behavior, 140-147
Shopping assessment, 44
Siblings, 186
Situational evaluation, 39; see also
Situational assessments
Social skills curriculum, 223
Social skins training, 151, 175; see also
Interpersonal skins training
Spouse, 176, 185
Staff involvement, 176
Stafftraining,63-76
Stimulus control, 145
Stress management training, 139; see also
Relaxation techniques
Target behavior, 12, 13
TBI education, 106, 215
239
Token economy, 152; see also Motivational
systems, Point systems
Topography, 13-15
Trials to criterion, 18
Tutorial process, 63
Unauthorized breaks from vocational sites,
94; see also Punctuality
Verbal abuse, 94, 135; see also Profanity and
swearing
Verbal prompting, 19
Verbal rehearsal, 80
Visual cue, 92
Visual imagery, 93
Vomiting, 174; see also Bulimia
Weight loss, 174; see also Bulimia; Vomiting
Whole interval recording, 18
Written rehearsal, 80
Y oung adults, 186
Vous aimerez peut-être aussi
- Neuropsychological Rehabilitation: Principles and ApplicationsD'EverandNeuropsychological Rehabilitation: Principles and ApplicationsJamuna RajeswaranÉvaluation : 5 sur 5 étoiles5/5 (1)
- George P. Prigatano-Principles of Neuropsychological Rehabilitation PDFDocument375 pagesGeorge P. Prigatano-Principles of Neuropsychological Rehabilitation PDFTlaloc Gonzalez100% (7)
- Cognitive Rehabilitation of Memory: A Clinical-Neuropsychological IntroductionD'EverandCognitive Rehabilitation of Memory: A Clinical-Neuropsychological IntroductionPas encore d'évaluation
- The The Practice of Clinical Neuropsychology Studies On Neuropsychology Development and CognitionDocument392 pagesThe The Practice of Clinical Neuropsychology Studies On Neuropsychology Development and CognitionJelena Jovanovic100% (6)
- Topics in Behavioral Neurology and Neuropsychology: With Key ReferencesD'EverandTopics in Behavioral Neurology and Neuropsychology: With Key ReferencesPas encore d'évaluation
- (Critical Issues in Neuropsychology) Louise Margaret Smith, Hamish P. D. Godfrey (auth.)-Family Support Programs and Rehabilitation_ A Cognitive-Behavioral Approach to Traumatic Brain Injury-Springer .pdfDocument227 pages(Critical Issues in Neuropsychology) Louise Margaret Smith, Hamish P. D. Godfrey (auth.)-Family Support Programs and Rehabilitation_ A Cognitive-Behavioral Approach to Traumatic Brain Injury-Springer .pdfDebora Berger100% (1)
- Neuropsychiatric Guide to Modern Everyday PsychiatD'EverandNeuropsychiatric Guide to Modern Everyday PsychiatPas encore d'évaluation
- Neuropsychological RehabilitationDocument26 pagesNeuropsychological RehabilitationMaría Belén FaríasPas encore d'évaluation
- Bottom Up: An Integrated Neurological and Cognitive Behavioural Book Which Addresses the Key Principles of Neuropsychotherapy. Five Important Emotional Parts of the Brain with Skills Training.D'EverandBottom Up: An Integrated Neurological and Cognitive Behavioural Book Which Addresses the Key Principles of Neuropsychotherapy. Five Important Emotional Parts of the Brain with Skills Training.Pas encore d'évaluation
- Practitioner's Guide To Clinical Neuropsychology (PDFDrive)Document398 pagesPractitioner's Guide To Clinical Neuropsychology (PDFDrive)Miguel AlvarezPas encore d'évaluation
- Neuropsychological Evaluation of the Older Adult: A Clinician's GuidebookD'EverandNeuropsychological Evaluation of the Older Adult: A Clinician's GuidebookÉvaluation : 3 sur 5 étoiles3/5 (1)
- Functional Movement Disorder: Kathrin Lafaver Carine W. Maurer Timothy R. Nicholson David L. Perez EditorsDocument455 pagesFunctional Movement Disorder: Kathrin Lafaver Carine W. Maurer Timothy R. Nicholson David L. Perez Editors李世民100% (3)
- Neurosurgical Neuropsychology: The Practical Application of Neuropsychology in the Neurosurgical PracticeD'EverandNeurosurgical Neuropsychology: The Practical Application of Neuropsychology in the Neurosurgical PracticeCaleb M. PearsonPas encore d'évaluation
- Neuropsychological RehabilitationDocument18 pagesNeuropsychological RehabilitationAliPas encore d'évaluation
- International Handbook of Neuropsychological Rehabilitation PDFDocument376 pagesInternational Handbook of Neuropsychological Rehabilitation PDFTlaloc Gonzalez100% (2)
- Neuropsychology Study Guide & Board Review (2014)Document666 pagesNeuropsychology Study Guide & Board Review (2014)pachozal100% (6)
- Cognitive Rehabilitation Manual PDFDocument24 pagesCognitive Rehabilitation Manual PDFShreya Sharma100% (2)
- (Critical Issues in Neuropsychology) Theresa Incagnoli (Auth.), Gerald Goldstein, Theresa M. Incagnoli (Eds.) - Contemporary Approaches To Neuropsychological Assessment-Springer US (1997)Document425 pages(Critical Issues in Neuropsychology) Theresa Incagnoli (Auth.), Gerald Goldstein, Theresa M. Incagnoli (Eds.) - Contemporary Approaches To Neuropsychological Assessment-Springer US (1997)dpf050100% (1)
- Child Neuropsychology PDFDocument348 pagesChild Neuropsychology PDFHugo Hernandez100% (6)
- Encycl in Neuro PsyDocument2 813 pagesEncycl in Neuro PsyAnonymous haOGKg8JUV100% (3)
- Neuropsychology A Twentieth-Century ScienceDocument32 pagesNeuropsychology A Twentieth-Century ScienceIcaro100% (1)
- Thomas D. Parsons (Auth.) - Clinical Neuropsychology and Technology - What's New and How We Can Use It (2016, Springer International Publishing)Document198 pagesThomas D. Parsons (Auth.) - Clinical Neuropsychology and Technology - What's New and How We Can Use It (2016, Springer International Publishing)Ever Josue Alvarenga100% (2)
- NeuroDocument329 pagesNeuroNicol Mariana V. Fernández100% (2)
- Clinical Neuropsychology - P. Snyder, Et. AlDocument782 pagesClinical Neuropsychology - P. Snyder, Et. AlAlexandra Balan100% (11)
- Dementia in Clinical PracticeDocument250 pagesDementia in Clinical Practicekatty100% (1)
- Interview and Testing: The Data Collection Phase of Neuropsychological EvaluationsDocument43 pagesInterview and Testing: The Data Collection Phase of Neuropsychological EvaluationsJessyMH100% (4)
- Neuropsychological Neurology The Neurocognitive Impairments of Neurological Disorders PDFDocument244 pagesNeuropsychological Neurology The Neurocognitive Impairments of Neurological Disorders PDFIKFR Unpad100% (3)
- Practical Psychology in Medical RehabilitationDocument591 pagesPractical Psychology in Medical RehabilitationHîrjoabă Ioan100% (1)
- Clinician S Guide To Neuropsychological AssessmentDocument538 pagesClinician S Guide To Neuropsychological Assessmentmulix8880% (5)
- (American Academy of Clinical Neuropsychology Oxford Workshop) Glenn E. Smith, Mark W. Bondi - Mild Cognitive Impairment and Dementia_ Definitions, Diagnosis, and Treatment-Oxford University Press (20 (1).pdfDocument416 pages(American Academy of Clinical Neuropsychology Oxford Workshop) Glenn E. Smith, Mark W. Bondi - Mild Cognitive Impairment and Dementia_ Definitions, Diagnosis, and Treatment-Oxford University Press (20 (1).pdfNicole CamachoPas encore d'évaluation
- Antolin M. Llorente-Principles of Neuropsychological Assessment With Hispanics - 2007Document252 pagesAntolin M. Llorente-Principles of Neuropsychological Assessment With Hispanics - 2007Anneliese FuentesPas encore d'évaluation
- (Handbook of Behavioral Neurobiology 2) Harold Goodglass, Edith Kaplan (Auth.), Michael S. Gazzaniga (Eds.) - Neuropsychology-Springer US (1979)Document569 pages(Handbook of Behavioral Neurobiology 2) Harold Goodglass, Edith Kaplan (Auth.), Michael S. Gazzaniga (Eds.) - Neuropsychology-Springer US (1979)Lic Paola PrémoloPas encore d'évaluation
- Pediatric Neuropsychology Case Studies PDFDocument358 pagesPediatric Neuropsychology Case Studies PDFGabriela Hernandez100% (1)
- Movement Disorders RehabilitationDocument193 pagesMovement Disorders RehabilitationJacob DoughertyPas encore d'évaluation
- A Neuropsychological AnalysisDocument193 pagesA Neuropsychological AnalysisSARA RUEDA JIMENEZ100% (1)
- Neural - Plasticity - and - Disorders - of - The - Nervous - System 2006 PDFDocument405 pagesNeural - Plasticity - and - Disorders - of - The - Nervous - System 2006 PDFMatei TeodorescuPas encore d'évaluation
- Rehabilitation For TBI PDFDocument383 pagesRehabilitation For TBI PDFJerry Kurnia WahyudiPas encore d'évaluation
- MB - CM.SL.2018. Enciclopedia de Neuropsicología ClínicaDocument3 848 pagesMB - CM.SL.2018. Enciclopedia de Neuropsicología ClínicaAlejandro Guzman100% (5)
- Neurologic Differential Diagnosis - A Case-Based Approach (PDFDrive)Document1 678 pagesNeurologic Differential Diagnosis - A Case-Based Approach (PDFDrive)veerrajuPas encore d'évaluation
- History of Neuropsychology PDFDocument365 pagesHistory of Neuropsychology PDFAna Rita Serra71% (7)
- 2015 Book PainEmotionAndCognitionDocument246 pages2015 Book PainEmotionAndCognitionYEILING LORENA GUERRERO GRANADOS100% (1)
- 3 Neuropsychiatric Symptoms of Cognitive Impairment and DementiaDocument375 pages3 Neuropsychiatric Symptoms of Cognitive Impairment and Dementiajuby30Pas encore d'évaluation
- Cognitive Rehabilitation For Attention Deficts Following StrokeDocument58 pagesCognitive Rehabilitation For Attention Deficts Following StrokeHardeep Singh BaliPas encore d'évaluation
- NeuroscienceDocument234 pagesNeuroscienceDrAvik Chakraborty100% (1)
- Lezak. Neuropsychological Assessment (5th Edition)Document1 576 pagesLezak. Neuropsychological Assessment (5th Edition)Anneliese Fuentes95% (107)
- Introduction To NeuropsychologyDocument15 pagesIntroduction To NeuropsychologyPsychology Department Ilahia Arts CollegePas encore d'évaluation
- Cognitive Impairment in Schizophrenia (2013) PDFDocument345 pagesCognitive Impairment in Schizophrenia (2013) PDFSdN100% (1)
- A Process Approach To Neuropsychological Assessment (Kaplan, 1988)Document42 pagesA Process Approach To Neuropsychological Assessment (Kaplan, 1988)MairaLabraPas encore d'évaluation
- Intraoperative Neurophysiological Monitoring 2011Document415 pagesIntraoperative Neurophysiological Monitoring 2011dr.darchPas encore d'évaluation
- Frontal LobesDocument275 pagesFrontal LobesSilvia Eugenia100% (7)
- Cognitive Remediation For Brain Injury and - Marvin H PoddDocument173 pagesCognitive Remediation For Brain Injury and - Marvin H PoddGheorghe Șarcani100% (1)
- Clinical Neurophysiology of The Vestibular System (001-057) PDFDocument57 pagesClinical Neurophysiology of The Vestibular System (001-057) PDFAriel CarterPas encore d'évaluation
- Cognitive Rehabilitation For Memory Deficits Following StrokeDocument23 pagesCognitive Rehabilitation For Memory Deficits Following StrokeHardeep Singh BaliPas encore d'évaluation
- Neuropsychological AssesmentDocument5 pagesNeuropsychological AssesmentodiliajessicanpviaPas encore d'évaluation
- Arthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDFDocument569 pagesArthur MacNeill Horton Jr. EdD ABPP ABPN, Lawrence C. Hartlage PHD ABPP ABPN - Handbook of Forensic Neuropsychology-Springer Publishing Company (2003) PDF'Minerva AlejandraPas encore d'évaluation
- Assessment Issues in Child NeuropsychologyDocument395 pagesAssessment Issues in Child NeuropsychologyLilith100% (2)
- The Neuropsychiatry of EpilepsyDocument361 pagesThe Neuropsychiatry of Epilepsypablo_zabala100% (3)
- @MBS MedicalBooksStore 2018 The PDFDocument1 061 pages@MBS MedicalBooksStore 2018 The PDFDhiya Muthiah Gaffari100% (6)
- Geriatric NeuropsychDocument480 pagesGeriatric NeuropsychSergio García100% (2)
- Textbook of Traumatic Brain Injury 2 Edition 228x300 PDFDocument687 pagesTextbook of Traumatic Brain Injury 2 Edition 228x300 PDFAnonymous q1NLY8R100% (5)
- CV Michael Naughton 2019Document2 pagesCV Michael Naughton 2019api-380850234Pas encore d'évaluation
- Memoire On Edgar Allan PoeDocument16 pagesMemoire On Edgar Allan PoeFarhaa AbdiPas encore d'évaluation
- Workshop 02.1: Restart Controls: ANSYS Mechanical Basic Structural NonlinearitiesDocument16 pagesWorkshop 02.1: Restart Controls: ANSYS Mechanical Basic Structural NonlinearitiesSahil Jawa100% (1)
- Los Documentos de La Dictadura Que Entregó Estados Unidos (Parte 2)Document375 pagesLos Documentos de La Dictadura Que Entregó Estados Unidos (Parte 2)Todo NoticiasPas encore d'évaluation
- Trigonometry Primer Problem Set Solns PDFDocument80 pagesTrigonometry Primer Problem Set Solns PDFderenz30Pas encore d'évaluation
- The Personal Law of The Mahommedans, According To All The Schools (1880) Ali, Syed Ameer, 1849-1928Document454 pagesThe Personal Law of The Mahommedans, According To All The Schools (1880) Ali, Syed Ameer, 1849-1928David BaileyPas encore d'évaluation
- Data Science Online Workshop Data Science vs. Data AnalyticsDocument1 pageData Science Online Workshop Data Science vs. Data AnalyticsGaurav VarshneyPas encore d'évaluation
- DBA Daily StatusDocument9 pagesDBA Daily StatuspankajPas encore d'évaluation
- New VibesDocument12 pagesNew VibesSangeeta S. Bhagwat90% (20)
- Assignment 1 Front Sheet: Qualification BTEC Level 5 HND Diploma in Computing Unit Number and Title Submission DateDocument18 pagesAssignment 1 Front Sheet: Qualification BTEC Level 5 HND Diploma in Computing Unit Number and Title Submission DatecuongPas encore d'évaluation
- DSLP CalculationDocument7 pagesDSLP Calculationravi shankar100% (1)
- Easter in RomaniaDocument5 pagesEaster in RomaniaDragos IonutPas encore d'évaluation
- Roofing Shingles in KeralaDocument13 pagesRoofing Shingles in KeralaCertainteed Roofing tilesPas encore d'évaluation
- Spring94 Exam - Civ ProDocument4 pagesSpring94 Exam - Civ ProGenUp SportsPas encore d'évaluation
- THE LAW OF - John Searl Solution PDFDocument50 pagesTHE LAW OF - John Searl Solution PDFerehov1100% (1)
- Motivational Speech About Our Dreams and AmbitionsDocument2 pagesMotivational Speech About Our Dreams and AmbitionsÇhärlöttë Çhrístíñë Dë ÇöldëPas encore d'évaluation
- Mathematics Grade 5 Quarter 2: Answer KeyDocument4 pagesMathematics Grade 5 Quarter 2: Answer KeyApril Jean Cahoy100% (2)
- SpellsDocument86 pagesSpellsGypsy580% (5)
- 4 Major Advantages of Japanese Education SystemDocument3 pages4 Major Advantages of Japanese Education SystemIsa HafizaPas encore d'évaluation
- Multiple Linear RegressionDocument26 pagesMultiple Linear RegressionMarlene G Padigos100% (2)
- Ad1 MCQDocument11 pagesAd1 MCQYashwanth Srinivasa100% (1)
- The Gower Handbook of Project Management: Part 1: ProjectsDocument2 pagesThe Gower Handbook of Project Management: Part 1: ProjectschineduPas encore d'évaluation
- CLASS 12 PracticalDocument10 pagesCLASS 12 PracticalWORLD HISTORYPas encore d'évaluation
- Key Performance IndicatorsDocument15 pagesKey Performance IndicatorsAbdul HafeezPas encore d'évaluation
- Mathematics Trial SPM 2015 P2 Bahagian BDocument2 pagesMathematics Trial SPM 2015 P2 Bahagian BPauling ChiaPas encore d'évaluation
- Intrauterine Growth RestrictionDocument5 pagesIntrauterine Growth RestrictionColleen MercadoPas encore d'évaluation
- A Study On Investors Perception Towards Sharemarket in Sharekhan LTDDocument9 pagesA Study On Investors Perception Towards Sharemarket in Sharekhan LTDEditor IJTSRDPas encore d'évaluation
- Sucesos de Las Islas Filipinas PPT Content - Carlos 1Document2 pagesSucesos de Las Islas Filipinas PPT Content - Carlos 1A Mi YaPas encore d'évaluation
- Ar 2003Document187 pagesAr 2003Alberto ArrietaPas encore d'évaluation
- CSEC Eng A Summary ExerciseDocument1 pageCSEC Eng A Summary ExerciseArisha NicholsPas encore d'évaluation
- The Compound Effect by Darren Hardy - Book Summary: Jumpstart Your Income, Your Life, Your SuccessD'EverandThe Compound Effect by Darren Hardy - Book Summary: Jumpstart Your Income, Your Life, Your SuccessÉvaluation : 5 sur 5 étoiles5/5 (456)
- Summary of 12 Rules for Life: An Antidote to ChaosD'EverandSummary of 12 Rules for Life: An Antidote to ChaosÉvaluation : 4.5 sur 5 étoiles4.5/5 (294)
- Can't Hurt Me by David Goggins - Book Summary: Master Your Mind and Defy the OddsD'EverandCan't Hurt Me by David Goggins - Book Summary: Master Your Mind and Defy the OddsÉvaluation : 4.5 sur 5 étoiles4.5/5 (386)
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesD'EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesÉvaluation : 5 sur 5 étoiles5/5 (1636)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Summary of The Anxious Generation by Jonathan Haidt: How the Great Rewiring of Childhood Is Causing an Epidemic of Mental IllnessD'EverandSummary of The Anxious Generation by Jonathan Haidt: How the Great Rewiring of Childhood Is Causing an Epidemic of Mental IllnessPas encore d'évaluation
- Book Summary of Ego Is The Enemy by Ryan HolidayD'EverandBook Summary of Ego Is The Enemy by Ryan HolidayÉvaluation : 4.5 sur 5 étoiles4.5/5 (388)
- The One Thing: The Surprisingly Simple Truth Behind Extraordinary ResultsD'EverandThe One Thing: The Surprisingly Simple Truth Behind Extraordinary ResultsÉvaluation : 4.5 sur 5 étoiles4.5/5 (709)
- Summary of The New Menopause by Mary Claire Haver MD: Navigating Your Path Through Hormonal Change with Purpose, Power, and FactsD'EverandSummary of The New Menopause by Mary Claire Haver MD: Navigating Your Path Through Hormonal Change with Purpose, Power, and FactsPas encore d'évaluation
- The War of Art by Steven Pressfield - Book Summary: Break Through The Blocks And Win Your Inner Creative BattlesD'EverandThe War of Art by Steven Pressfield - Book Summary: Break Through The Blocks And Win Your Inner Creative BattlesÉvaluation : 4.5 sur 5 étoiles4.5/5 (274)
- Summary of The Algebra of Wealth by Scott Galloway: A Simple Formula for Financial SecurityD'EverandSummary of The Algebra of Wealth by Scott Galloway: A Simple Formula for Financial SecurityPas encore d'évaluation
- How To Win Friends and Influence People by Dale Carnegie - Book SummaryD'EverandHow To Win Friends and Influence People by Dale Carnegie - Book SummaryÉvaluation : 5 sur 5 étoiles5/5 (557)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessD'EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (328)
- The Whole-Brain Child by Daniel J. Siegel, M.D., and Tina Payne Bryson, PhD. - Book Summary: 12 Revolutionary Strategies to Nurture Your Child’s Developing MindD'EverandThe Whole-Brain Child by Daniel J. Siegel, M.D., and Tina Payne Bryson, PhD. - Book Summary: 12 Revolutionary Strategies to Nurture Your Child’s Developing MindÉvaluation : 4.5 sur 5 étoiles4.5/5 (57)
- Make It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningD'EverandMake It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningÉvaluation : 4.5 sur 5 étoiles4.5/5 (55)
- Summary of The Galveston Diet by Mary Claire Haver MD: The Doctor-Developed, Patient-Proven Plan to Burn Fat and Tame Your Hormonal SymptomsD'EverandSummary of The Galveston Diet by Mary Claire Haver MD: The Doctor-Developed, Patient-Proven Plan to Burn Fat and Tame Your Hormonal SymptomsPas encore d'évaluation
- Blink by Malcolm Gladwell - Book Summary: The Power of Thinking Without ThinkingD'EverandBlink by Malcolm Gladwell - Book Summary: The Power of Thinking Without ThinkingÉvaluation : 4.5 sur 5 étoiles4.5/5 (114)
- Steal Like an Artist by Austin Kleon - Book Summary: 10 Things Nobody Told You About Being CreativeD'EverandSteal Like an Artist by Austin Kleon - Book Summary: 10 Things Nobody Told You About Being CreativeÉvaluation : 4.5 sur 5 étoiles4.5/5 (128)
- Summary of "Measure What Matters" by John Doerr: How Google, Bono, and the Gates Foundation Rock the World with OKRs — Finish Entire Book in 15 MinutesD'EverandSummary of "Measure What Matters" by John Doerr: How Google, Bono, and the Gates Foundation Rock the World with OKRs — Finish Entire Book in 15 MinutesÉvaluation : 4.5 sur 5 étoiles4.5/5 (62)
- Summary of The Algebra of Wealth: A Simple Formula for Financial SecurityD'EverandSummary of The Algebra of Wealth: A Simple Formula for Financial SecurityÉvaluation : 4 sur 5 étoiles4/5 (1)
- Summary of Miracle Morning Millionaires: What the Wealthy Do Before 8AM That Will Make You Rich by Hal Elrod and David OsbornD'EverandSummary of Miracle Morning Millionaires: What the Wealthy Do Before 8AM That Will Make You Rich by Hal Elrod and David OsbornÉvaluation : 5 sur 5 étoiles5/5 (201)
- Summary of Million Dollar Weekend by Noah Kagan and Tahl Raz: The Surprisingly Simple Way to Launch a 7-Figure Business in 48 HoursD'EverandSummary of Million Dollar Weekend by Noah Kagan and Tahl Raz: The Surprisingly Simple Way to Launch a 7-Figure Business in 48 HoursPas encore d'évaluation
- Summary of Atomic Habits by James ClearD'EverandSummary of Atomic Habits by James ClearÉvaluation : 5 sur 5 étoiles5/5 (169)
- Designing Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeD'EverandDesigning Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (62)
- Extreme Ownership by Jocko Willink and Leif Babin - Book Summary: How U.S. Navy SEALS Lead And WinD'EverandExtreme Ownership by Jocko Willink and Leif Babin - Book Summary: How U.S. Navy SEALS Lead And WinÉvaluation : 4.5 sur 5 étoiles4.5/5 (75)
- SUMMARY: So Good They Can't Ignore You (UNOFFICIAL SUMMARY: Lesson from Cal Newport)D'EverandSUMMARY: So Good They Can't Ignore You (UNOFFICIAL SUMMARY: Lesson from Cal Newport)Évaluation : 4.5 sur 5 étoiles4.5/5 (14)
- The 5 Second Rule by Mel Robbins - Book Summary: Transform Your Life, Work, and Confidence with Everyday CourageD'EverandThe 5 Second Rule by Mel Robbins - Book Summary: Transform Your Life, Work, and Confidence with Everyday CourageÉvaluation : 4.5 sur 5 étoiles4.5/5 (329)
- Essentialism by Greg McKeown - Book Summary: The Disciplined Pursuit of LessD'EverandEssentialism by Greg McKeown - Book Summary: The Disciplined Pursuit of LessÉvaluation : 4.5 sur 5 étoiles4.5/5 (188)