Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NDocument2 pagesJFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NDocument2 pagesJFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NMuhammad Adzan AkbarPas encore d'évaluation
- JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NDocument2 pagesJFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument54 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NDocument1 pageJFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NMuhammad Adzan AkbarPas encore d'évaluation
- JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NDocument1 pageJFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NDocument1 pageJFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, N JFKJJGGJJJ, NMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument81 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument27 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GDocument27 pagesKJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, G KJFDKGF, GMuhammad Adzan AkbarPas encore d'évaluation
- Synthesis of Oxazolidinone Phosphonate Derivatives, Part II: Jae-Min Hwang, Sung-Ho Yeom, and Kang-Yeoun JungDocument6 pagesSynthesis of Oxazolidinone Phosphonate Derivatives, Part II: Jae-Min Hwang, Sung-Ho Yeom, and Kang-Yeoun JungMuhammad Adzan AkbarPas encore d'évaluation
- Kamus CompDocument8 pagesKamus CompMuhammad Adzan AkbarPas encore d'évaluation
- ARTICLE Sleep Tips: 7 Steps To Better SleepDocument9 pagesARTICLE Sleep Tips: 7 Steps To Better SleepMuhammad Adzan AkbarPas encore d'évaluation
- Doctor'S Role, Function and DutyDocument6 pagesDoctor'S Role, Function and DutyMuhammad Adzan AkbarPas encore d'évaluation
- Literature SearchingDocument19 pagesLiterature SearchingMuhammad Adzan AkbarPas encore d'évaluation
- Type 2 Diabetes in Childhood and Adolescence Is At-: Pediatric Allergy: Principles and PracticeDocument1 pageType 2 Diabetes in Childhood and Adolescence Is At-: Pediatric Allergy: Principles and PracticeMuhammad Adzan AkbarPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Cable For Solar Power SystemDocument1 pageCable For Solar Power SystemEnspartan 63Pas encore d'évaluation
- Rijwana Hussein Final EssayDocument18 pagesRijwana Hussein Final EssayhusseinrijwanaPas encore d'évaluation
- Pengaruh Kelas Lereng Dan Tutupan Lahan Terhadap Solum Tanah, Kedalaman Efektif Akar Dan PH TanahDocument10 pagesPengaruh Kelas Lereng Dan Tutupan Lahan Terhadap Solum Tanah, Kedalaman Efektif Akar Dan PH TanahAPRI YANSYAHPas encore d'évaluation
- Signed PAN: Erwin Panofsky's (1892-1968) "The History of Art As A Humanistic Discipline" (Princeton, 1938)Document94 pagesSigned PAN: Erwin Panofsky's (1892-1968) "The History of Art As A Humanistic Discipline" (Princeton, 1938)Adrian Anton MarinPas encore d'évaluation
- RPS Bahasa Inggris Untuk Fisika 2020 TranslateDocument4 pagesRPS Bahasa Inggris Untuk Fisika 2020 TranslateIndah SaputriPas encore d'évaluation
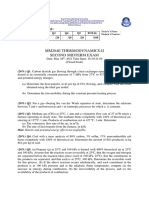
- Mm204E Thermodynamics-Ii Second Midterm Exam: Q1 Q2 Q3 Q4 Q5 Total /20 /20 /20 /20 /20 /100Document2 pagesMm204E Thermodynamics-Ii Second Midterm Exam: Q1 Q2 Q3 Q4 Q5 Total /20 /20 /20 /20 /20 /100Ali DoğruPas encore d'évaluation
- Test Bank For Economic Development The Pearson Series in Economics 11th Edition Michael P TodaroDocument24 pagesTest Bank For Economic Development The Pearson Series in Economics 11th Edition Michael P TodaroRebeccaRodriguezcqgf100% (49)
- Identification of The Best Model and Parameters For T-Y-X Equilibrium Data of Ethanol-Water MixtureDocument7 pagesIdentification of The Best Model and Parameters For T-Y-X Equilibrium Data of Ethanol-Water MixtureMeghana SPas encore d'évaluation
- Title Page (Research 2)Document10 pagesTitle Page (Research 2)sagunsophiarozzPas encore d'évaluation
- IAL Mathematics Formula BookDocument34 pagesIAL Mathematics Formula BookHaleef Mk0% (1)
- Soc (Cad 1)Document34 pagesSoc (Cad 1)ASIST MechPas encore d'évaluation
- Breeding Objectives, Selection Criteria and Breeding System of Indigenous Goat Types in Bale Zone, Oromia, EthiopiaDocument10 pagesBreeding Objectives, Selection Criteria and Breeding System of Indigenous Goat Types in Bale Zone, Oromia, EthiopiareinpolyPas encore d'évaluation
- Philosophical Foundations of Curriculum DevelopmentDocument34 pagesPhilosophical Foundations of Curriculum DevelopmentAdeeb AhmadPas encore d'évaluation
- Popular Horoscopes and The "Barnum Effect" PDFDocument12 pagesPopular Horoscopes and The "Barnum Effect" PDFYilbert Oswaldo Jimenez CanoPas encore d'évaluation
- Effects of Noise PollutionDocument2 pagesEffects of Noise PollutionMishal FatimaPas encore d'évaluation
- Name - Date - Class - Density NotesDocument2 pagesName - Date - Class - Density NotesBranchley LefrancPas encore d'évaluation
- FormulaShell SAE 10W 40 Motor Oil DatasheetDocument3 pagesFormulaShell SAE 10W 40 Motor Oil DatasheetAnonymous YjoCCKPas encore d'évaluation
- Xglo & Lightsystem Indoor/Outdoor Loosetube, Dca - Emea: Ordering InformationDocument2 pagesXglo & Lightsystem Indoor/Outdoor Loosetube, Dca - Emea: Ordering InformationDemetri M. ScythePas encore d'évaluation
- Earth Subsystem: BiosphereDocument17 pagesEarth Subsystem: BiosphereRhiza Mae LaxPas encore d'évaluation
- Literacy Planning Sheet Year Group: Reception Stimulus: Jolly Phonics Day Skill Learning Objective Main Teaching Focused Task(s) Key Skill 1Document2 pagesLiteracy Planning Sheet Year Group: Reception Stimulus: Jolly Phonics Day Skill Learning Objective Main Teaching Focused Task(s) Key Skill 1Engy HassanPas encore d'évaluation
- Appendix A 2Document7 pagesAppendix A 2MUNKIN QUINTEROPas encore d'évaluation
- DSP AssignmentDocument16 pagesDSP AssignmentPunitha ShanmugamPas encore d'évaluation
- NotesverifDocument4 pagesNotesverifSabitri SanyalPas encore d'évaluation
- Local Knowledge, Global GoalsDocument48 pagesLocal Knowledge, Global Goalsecossich123100% (1)
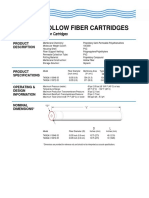
- Targa Ii Hollow Fiber Cartridges: 10-Inch Water Ultrafiltration CartridgesDocument2 pagesTarga Ii Hollow Fiber Cartridges: 10-Inch Water Ultrafiltration CartridgesChristianus RudyantoPas encore d'évaluation
- Technologies and Decision Support Systems To Aid Solid-WasteDocument18 pagesTechnologies and Decision Support Systems To Aid Solid-WasteNelson RiañoPas encore d'évaluation
- Malaysia VBI Full ReportDocument116 pagesMalaysia VBI Full ReportHasoPas encore d'évaluation
- Mechanical Engineering Department University of Engineering and Technology, LahoreDocument22 pagesMechanical Engineering Department University of Engineering and Technology, LahoreSyed MunawarPas encore d'évaluation
- 10) Assessment On Performance and Challenges of EthiopianDocument11 pages10) Assessment On Performance and Challenges of EthiopianyaregalPas encore d'évaluation
- Department of Education: Republic of The PhilippinesDocument36 pagesDepartment of Education: Republic of The PhilippinesKristine Rose CADUTDUTPas encore d'évaluation