Vous aimerez peut-être aussi
- Usmle Surgery Mcqs PDFDocument2 pagesUsmle Surgery Mcqs PDFGhadeer Ebraheem75% (4)
- One Hundred YearsDocument18 pagesOne Hundred YearsolziichPas encore d'évaluation
- English Time 3Document79 pagesEnglish Time 3Ghadeer Ebraheem100% (2)
- HIV and HIV CounsellingDocument12 pagesHIV and HIV CounsellingGhadeer EbraheemPas encore d'évaluation
- GcsDocument1 pageGcsGhadeer EbraheemPas encore d'évaluation
- ATLS DRDocument45 pagesATLS DRNeNeei HenNiePas encore d'évaluation
- Myotomes of The Upper LimbDocument2 pagesMyotomes of The Upper LimbGhadeer Ebraheem0% (1)
- Leach and Lily Stanley - Last Updated On: Edit This Article View RevisionsDocument7 pagesLeach and Lily Stanley - Last Updated On: Edit This Article View RevisionsGhadeer EbraheemPas encore d'évaluation
- PalsDocument12 pagesPalsGhadeer EbraheemPas encore d'évaluation
- Antibody Tests Reveal Red Blood Cell AntibodiesDocument2 pagesAntibody Tests Reveal Red Blood Cell AntibodiesGhadeer EbraheemPas encore d'évaluation
- Mansmed Surgery QbankDocument7 pagesMansmed Surgery QbankGhadeer EbraheemPas encore d'évaluation
- Acid Base PhysiologyDocument4 pagesAcid Base PhysiologyGhadeer EbraheemPas encore d'évaluation
- Medical Therapies for Antibody DeficienciesDocument5 pagesMedical Therapies for Antibody DeficienciesGhadeer EbraheemPas encore d'évaluation
- Leach and Lily Stanley - Last Updated On: Edit This Article View RevisionsDocument7 pagesLeach and Lily Stanley - Last Updated On: Edit This Article View RevisionsGhadeer EbraheemPas encore d'évaluation
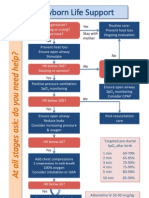
- Arc Neonatal FlowchartDocument1 pageArc Neonatal FlowchartChander KantaPas encore d'évaluation
- Inflamatory Bowel Disease: Dr. Samir IsmailDocument82 pagesInflamatory Bowel Disease: Dr. Samir IsmailGhadeer EbraheemPas encore d'évaluation
- Neuro ExaminationDocument82 pagesNeuro ExaminationGhadeer Ebraheem100% (1)
- Vasc Med 1998 Powell 21 8Document9 pagesVasc Med 1998 Powell 21 8Ghadeer EbraheemPas encore d'évaluation
- Drugs Causing HirsutismDocument1 pageDrugs Causing HirsutismGhadeer EbraheemPas encore d'évaluation
- RicketsDocument7 pagesRicketsGhadeer EbraheemPas encore d'évaluation
- 5 - Health Care System Awad Etc 2009Document11 pages5 - Health Care System Awad Etc 2009Ghadeer EbraheemPas encore d'évaluation
- Drugs Causing HirsutismDocument1 pageDrugs Causing HirsutismGhadeer EbraheemPas encore d'évaluation
- Nephrotic SyndromeDocument1 pageNephrotic SyndromeGhadeer EbraheemPas encore d'évaluation
- Anatomy 2 MnemonicsDocument46 pagesAnatomy 2 MnemonicsGhadeer EbraheemPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- En Booklet PDFDocument113 pagesEn Booklet PDFRoyal CurePas encore d'évaluation
- CPT PCM NHSNDocument307 pagesCPT PCM NHSNYrvon RafaPas encore d'évaluation
- Aggravating Factors Precipitating Factors Predisposing FactorsDocument4 pagesAggravating Factors Precipitating Factors Predisposing FactorsJann ericka JaoPas encore d'évaluation
- Diagnostic Endocrinology Blood Steroid Concentrations in Neutered Male and Female HabbitsDocument4 pagesDiagnostic Endocrinology Blood Steroid Concentrations in Neutered Male and Female HabbitsThatiana SanchesPas encore d'évaluation
- Risk Factors For Pelvic Surgery: Y.E. Erata B. Kilic S. Güçlü U. Saygili T. UsluDocument5 pagesRisk Factors For Pelvic Surgery: Y.E. Erata B. Kilic S. Güçlü U. Saygili T. UsluGleiciane AguiarPas encore d'évaluation
- Changing A Urinary Diversion Ostomy ApplianceDocument3 pagesChanging A Urinary Diversion Ostomy Appliancemyer pasandalanPas encore d'évaluation
- Rubin - Ovarian Cancer 2ed PDFDocument207 pagesRubin - Ovarian Cancer 2ed PDFfdroooPas encore d'évaluation
- Scanning Systems, Ultrasonic, Cardiac Intravascular: Scope of This Product ComparisonDocument75 pagesScanning Systems, Ultrasonic, Cardiac Intravascular: Scope of This Product Comparisonkevin. mitnickPas encore d'évaluation
- Maternal Perception of Fetal Movements and Real-Time Ultrasound FindingsDocument6 pagesMaternal Perception of Fetal Movements and Real-Time Ultrasound FindingsDarian AngPas encore d'évaluation
- Family Welfare Programme in IndiaDocument25 pagesFamily Welfare Programme in IndiaTirumalesha DadigePas encore d'évaluation
- Endocrinology, Diabetes, and Metabolism - American Board of Internal Medicine - ABIMDocument3 pagesEndocrinology, Diabetes, and Metabolism - American Board of Internal Medicine - ABIMabimorgPas encore d'évaluation
- Surgical TechniqueDocument6 pagesSurgical TechniqueDavid PalomequePas encore d'évaluation
- Introduction To Endocrinology For Clinical StudentsDocument9 pagesIntroduction To Endocrinology For Clinical StudentsOhwovoriole ToketemuPas encore d'évaluation
- Twin to twin transfusion syndrome الدكتور ماهر معايطةDocument7 pagesTwin to twin transfusion syndrome الدكتور ماهر معايطةjordanmedicsPas encore d'évaluation
- Informatics Quiz 1 NAME: - DATE: - I. Multiple Choice. Choose The Best Answer. Encircle The Letter of The Correct AnswerDocument2 pagesInformatics Quiz 1 NAME: - DATE: - I. Multiple Choice. Choose The Best Answer. Encircle The Letter of The Correct Answerlouie roderosPas encore d'évaluation
- Dianosis Dan Resusitasi Pada Pasien Syok Perdarahan &Document31 pagesDianosis Dan Resusitasi Pada Pasien Syok Perdarahan &Strata PertiwiPas encore d'évaluation
- BrachytherapyDocument10 pagesBrachytherapyapi-279886264Pas encore d'évaluation
- Philippine Airlines Vs NLRCDocument5 pagesPhilippine Airlines Vs NLRCAntonio kwalalumporPas encore d'évaluation
- DRUG STUDY TITLEDocument2 pagesDRUG STUDY TITLEpretty_mary100% (4)
- Ateneo de Davao University Graduate SchoolDocument10 pagesAteneo de Davao University Graduate SchoolDennis Nabor Muñoz, RN,RMPas encore d'évaluation
- Koch AO Manual Chapter 2 2005Document45 pagesKoch AO Manual Chapter 2 2005Juan Guillermo RamirezPas encore d'évaluation
- ACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Document15 pagesACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Reza ZulkarnainPas encore d'évaluation
- Role of Multi Detector (MDCT)Document52 pagesRole of Multi Detector (MDCT)ramon100% (5)
- Case AnalysisDocument3 pagesCase AnalysisDebi Bahinting Ouano-RotaPas encore d'évaluation
- G.augustin - Acute Abdomen During Pregnancy - 2014Document584 pagesG.augustin - Acute Abdomen During Pregnancy - 2014Constantin BudinPas encore d'évaluation
- Pelvic Planes Dimensions and ContractionTITLEDocument12 pagesPelvic Planes Dimensions and ContractionTITLEDavid Eka PrasetyaPas encore d'évaluation
- A New Look at The Safety of Breastfeeding During Pregnancy - KellyMomDocument11 pagesA New Look at The Safety of Breastfeeding During Pregnancy - KellyMomdoggydogPas encore d'évaluation
- Natural Family Planning MethodDocument36 pagesNatural Family Planning MethodJhuf FerrarenPas encore d'évaluation
- Daftar PustakaDocument4 pagesDaftar PustakaBilly Aditya PratamaPas encore d'évaluation
- One of These Days Reaction PaperDocument2 pagesOne of These Days Reaction PapercreamyfrappePas encore d'évaluation