Académique Documents
Professionnel Documents
Culture Documents
1 s2.0 S0022391310601473 Main PDF
Transféré par
Claudio Sumonte Hernandez0 évaluation0% ont trouvé ce document utile (0 vote)
39 vues7 pagesThis study suggests that the placement of foundation restorations on teeth with short ferrule heights improves the fatigue performance of the definitive restorations. A critical tooth height existed at which the placement of a foundation restoration resulted in no significant difference in the load fatigue performance.
Description originale:
Titre original
1-s2.0-S0022391310601473-main.pdf
Copyright
© © All Rights Reserved
Formats disponibles
PDF, TXT ou lisez en ligne sur Scribd
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentThis study suggests that the placement of foundation restorations on teeth with short ferrule heights improves the fatigue performance of the definitive restorations. A critical tooth height existed at which the placement of a foundation restoration resulted in no significant difference in the load fatigue performance.
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
0 évaluation0% ont trouvé ce document utile (0 vote)
39 vues7 pages1 s2.0 S0022391310601473 Main PDF
Transféré par
Claudio Sumonte HernandezThis study suggests that the placement of foundation restorations on teeth with short ferrule heights improves the fatigue performance of the definitive restorations. A critical tooth height existed at which the placement of a foundation restoration resulted in no significant difference in the load fatigue performance.
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
Vous êtes sur la page 1sur 7
The Journal of Prosthetic Dentistry
319 November 2010
Uy et al Uy et al
Clinical Implications
This in vitro study suggests that the placement of foundation
restorations on teeth with short ferrule heights improves the fatigue
performance of the definitive restorations.
Statement of problem. In badly damaged teeth and teeth with short clinical crown heights, the placement of founda-
tion restorations has been advocated to permit the development of retention and resistance form. However, there is little
information on the effect of these foundation restorations on the clinical performance of the definitive restoration.
Purpose. The purpose of this study was to evaluate the load fatigue performance of teeth restored with posts and
cores, with varying tooth heights, and to compare them with similar groups having no posts and cores. A secondary
purpose was to determine whether a critical tooth height existed at which the placement of a foundation restoration
resulted in no significant difference in the load fatigue performance.
Material and methods. Three test groups (n=10) with prepared tooth heights of 2, 3, and 4 mm were tested. These
were compared with another 3 groups with similar tooth heights that were restored with prefabricated titanium posts
and core heights of 4, 3, and 2 mm, respectively. Cast complete crowns were then fabricated and cemented with zinc
phosphate cement. A fatigue load of 58.8 N was applied at an angle of 135 degrees to the long axis of each crown-
tooth specimen. The number of cycles to preliminary failure was determined. Significant differences in cycles to pre-
liminary failure were assessed with 1-way ANOVA, followed by Tukey HSD tests (=.05).
Results. The group with the greatest preparation height (4 mm) and a 2-mm post-retained foundation had the high-
est number of cycles to preliminary failure (437,701), while the group with the shortest preparation height and no
foundation had the lowest number of cycles (53,806). The Tukey HSD multiple comparison tests showed that for all
3 tooth heights, groups with foundation restorations had a significantly higher number of cycles to preliminary failure
than those without foundation restorations.
Conclusions. For a given tooth height, teeth restored with foundation restorations had a significantly better load
fatigue performance than those with no foundation restoration. (J Prosthet Dent 2010;104:318-324)
The effect of tooth and foundation
restoration heights on the load fatigue
performance of cast crowns
Joanne N. Uy, DMD, MDS,
a
Jennifer C. L. Neo, BDS, MS,
b
and
Swee Heng Chan, Dip Industrial Eng, Adv Dip Eng Mgt
c
Faculty of Dentistry, National University of Singapore
This study was supported by a National University of Singapore research grant (R-224-000-026-112).
a
Assistant Professor, Department of Restorative Dentistry.
b
Associate Professor and Head, Department of Restorative Dentistry.
c
Laboratory Technologist.
The success of a cast restoration
depends largely on adequate reten-
tion and resistance.
1,2
Retention form
is defined as the feature of a tooth
preparation that resists dislodgement
of the crown in a vertical direction or
along the path of placement, while
resistance form is defined as the fea-
tures of a tooth preparation that en-
hance the stability of a restoration
and resist dislodgement along an axis
other than the path of placement.
3
Although initial studies focused on
the retention form of tooth prepara-
tions,
4,5
most of the recent literature
has focused extensively on the signifi-
cance and clinical relevance of resis-
tance form.
Several factors have been pro-
posed to enhance the resistance form
of a crown. These include placement
of interproximal grooves and box-
es,
6,7
inclined planes on the occlusal
surface of a crown preparation, and
placement of an occlusal isthmus.
8
However, a recent study by Proussaefs
et al
9
on the effects of different aux-
iliary preparation features related to
the resistance form of crowns showed
that auxiliary features pose no advan-
tage in enhancing resistance form.
The total occlusal convergence (TOC)
of a preparation is another factor that
affects resistance form.
10,11
Recent
studies have determined that instead
of the recommended TOC of 2 to 6
degrees,
1,12,13
dental students, general
practice residents, general dentists,
and prosthodontists created mean
TOC angles that ranged from 12.2 to
27 degrees.
14-18
A third factor affecting
resistance form is the occlusocervical
(OC) dimension.
19
Studies investigat-
ing the effect of occlusal height on
resistance form are limited. Maxwell
et al
20
tested the resistance of crowns
with occlusal preparation heights of
1, 2, 3, and 5 mm with a 6-degree
taper. The crowns were loaded at a
45-degree angle to catastrophic fail-
ure. The authors concluded that 3
mm was the minimal OC dimension
required to provide adequate resis-
tance to crowns. In a review by Good-
acre et al
21
on the principles of tooth
preparation, 3 mm was proposed as
the minimal OC dimension for anteri-
or teeth and premolars, and 4 mm for
molars. These values were determined
based on calculations of critical con-
vergence angles.
Adequate retention and resistance
form must be incorporated into the
design of the tooth preparation. In
most circumstances, however, teeth
in need of complete coverage restora-
tions have lost substantial tooth struc-
ture. In these situations, a foundation
restoration is indicated to permit de-
velopment of retention and resistance
form.
22
These foundation restorations
replace coronal tooth structure that
was lost as a result of caries, previ-
ous restorations, or tooth fracture.
Shillingburg et al
1
also suggested the
placement of a core reconstruction or
foundation restoration when one half
or more of the coronal tooth structure
is missing. For endodontically treated
teeth, a core alone may be placed if
adequate tooth structure remains.
23
For endodontically treated teeth with
moderate to severe tooth structure
loss, a cast post-and-core restoration
may be placed prior to the definitive
restoration.
24
Posts and cores can transfer occlu-
sal forces intraradicularly, with resul-
tant predisposition to vertical fracture
of the root.
25,26
In 1961, Rosen
27
pro-
posed the concept of an extracoronal
brace to prevent tooth fracture. The
term ferrule effect was used to de-
scribe this 360-degree ring of cast
metal, and extension of the defini-
tive restoration at least 2 mm apical
to the junction of the core and re-
maining tooth structure was recom-
mended.
28
Over the years, numerous
studies have investigated the ferrule
effect.
28-31
These studies demon-
strated that to maximize the ferrule
effect, the clinician should retain as
much tooth structure as possible. A
minimum of 1.5-2 mm of intact tooth
structure above the crown margin has
been proposed as a guideline. If the
tooth to be restored is severely dam-
aged, surgical crown lengthening
32
or orthodontic extrusion
33
should be
considered to establish a ferrule.
Few studies have evaluated the ef-
fect of different ferrule heights on en-
hancing resistance form.
34-38
Pereira et
al
36
compared the fracture strengths
of endodontically treated teeth us-
ing prefabricated stainless steel posts,
composite resin cores, and varying
ferrule heights. The authors mea-
sured fracture resistance on teeth
with 0-mm, 1-mm, 2-mm, and 3-mm
ferrule heights and found that an in-
creased amount of coronal dentin
significantly increased the fracture re-
sistance. Another study by de Oliveira
et al
37
tested teeth with similar ferrule
heights. The teeth were restored with
carbon fiber posts, composite resin
cores, and cast crowns. The authors
found no significant difference in
fracture resistance, and hypothesized
that minimal differences in the elas-
tic moduli of the carbon fiber post
and dentin resulted in the forces be-
ing distributed similarly along the
length of the post, regardless of the
ferrule height. Al-Wahadni and Gut-
teridge
38
also investigated the fracture
resistance of teeth restored with cast
posts and partial cores supported by
different ferrule heights. The authors
concluded that a 3-mm ferrule height
had a significantly higher resistance
to fracture compared to control teeth
with a 0-mm ferrule, whereas greater
ferrule heights did not produce statis-
tically significant improvements.
The purpose of this study was to
evaluate the load fatigue performance
of teeth restored with posts and cores,
with varying tooth heights. These
were compared with similar groups
having no posts and cores. The null
hypothesis was that the load fatigue
performance of teeth restored with
posts and cores would not be differ-
ent from those without posts and
cores. The secondary purpose was
to determine whether a critical tooth
height existed at which the placement
of a foundation restoration resulted
in no significant difference in the load
fatigue performance. The secondary
null hypothesis was that the place-
ment of a foundation restoration for
any given tooth height would result in
no difference in load fatigue perfor-
mance when compared to no founda-
tion restoration.
MATERIAL AND METHODS
Human first and second premo-
lars, extracted for orthodontic reasons,
were used in this study. The criteria for
selection were the presence of a single
canal, absence of cracks or fractures, no
evidence of caries or restorations, and
no previous endodontic treatment. The
teeth were stored in 0.5% chloramine-T
solution (Chloramine T; Merck KGaA,
Darmstadt, Germany) for 1 week, fol-
lowed by storage in distilled water.
The buccopalatal dimensions of
the teeth were measured using an
electronic vernier caliper (Absolute
The Journal of Prosthetic Dentistry
319 November 2010
Uy et al Uy et al
Clinical Implications
This in vitro study suggests that the placement of foundation
restorations on teeth with short ferrule heights improves the fatigue
performance of the definitive restorations.
Statement of problem. In badly damaged teeth and teeth with short clinical crown heights, the placement of founda-
tion restorations has been advocated to permit the development of retention and resistance form. However, there is little
information on the effect of these foundation restorations on the clinical performance of the definitive restoration.
Purpose. The purpose of this study was to evaluate the load fatigue performance of teeth restored with posts and
cores, with varying tooth heights, and to compare them with similar groups having no posts and cores. A secondary
purpose was to determine whether a critical tooth height existed at which the placement of a foundation restoration
resulted in no significant difference in the load fatigue performance.
Material and methods. Three test groups (n=10) with prepared tooth heights of 2, 3, and 4 mm were tested. These
were compared with another 3 groups with similar tooth heights that were restored with prefabricated titanium posts
and core heights of 4, 3, and 2 mm, respectively. Cast complete crowns were then fabricated and cemented with zinc
phosphate cement. A fatigue load of 58.8 N was applied at an angle of 135 degrees to the long axis of each crown-
tooth specimen. The number of cycles to preliminary failure was determined. Significant differences in cycles to pre-
liminary failure were assessed with 1-way ANOVA, followed by Tukey HSD tests (=.05).
Results. The group with the greatest preparation height (4 mm) and a 2-mm post-retained foundation had the high-
est number of cycles to preliminary failure (437,701), while the group with the shortest preparation height and no
foundation had the lowest number of cycles (53,806). The Tukey HSD multiple comparison tests showed that for all
3 tooth heights, groups with foundation restorations had a significantly higher number of cycles to preliminary failure
than those without foundation restorations.
Conclusions. For a given tooth height, teeth restored with foundation restorations had a significantly better load
fatigue performance than those with no foundation restoration. (J Prosthet Dent 2010;104:318-324)
The effect of tooth and foundation
restoration heights on the load fatigue
performance of cast crowns
Joanne N. Uy, DMD, MDS,
a
Jennifer C. L. Neo, BDS, MS,
b
and
Swee Heng Chan, Dip Industrial Eng, Adv Dip Eng Mgt
c
Faculty of Dentistry, National University of Singapore
This study was supported by a National University of Singapore research grant (R-224-000-026-112).
a
Assistant Professor, Department of Restorative Dentistry.
b
Associate Professor and Head, Department of Restorative Dentistry.
c
Laboratory Technologist.
The success of a cast restoration
depends largely on adequate reten-
tion and resistance.
1,2
Retention form
is defined as the feature of a tooth
preparation that resists dislodgement
of the crown in a vertical direction or
along the path of placement, while
resistance form is defined as the fea-
tures of a tooth preparation that en-
hance the stability of a restoration
and resist dislodgement along an axis
other than the path of placement.
3
Although initial studies focused on
the retention form of tooth prepara-
tions,
4,5
most of the recent literature
has focused extensively on the signifi-
cance and clinical relevance of resis-
tance form.
Several factors have been pro-
posed to enhance the resistance form
of a crown. These include placement
of interproximal grooves and box-
es,
6,7
inclined planes on the occlusal
surface of a crown preparation, and
placement of an occlusal isthmus.
8
However, a recent study by Proussaefs
et al
9
on the effects of different aux-
iliary preparation features related to
the resistance form of crowns showed
that auxiliary features pose no advan-
tage in enhancing resistance form.
The total occlusal convergence (TOC)
of a preparation is another factor that
affects resistance form.
10,11
Recent
studies have determined that instead
of the recommended TOC of 2 to 6
degrees,
1,12,13
dental students, general
practice residents, general dentists,
and prosthodontists created mean
TOC angles that ranged from 12.2 to
27 degrees.
14-18
A third factor affecting
resistance form is the occlusocervical
(OC) dimension.
19
Studies investigat-
ing the effect of occlusal height on
resistance form are limited. Maxwell
et al
20
tested the resistance of crowns
with occlusal preparation heights of
1, 2, 3, and 5 mm with a 6-degree
taper. The crowns were loaded at a
45-degree angle to catastrophic fail-
ure. The authors concluded that 3
mm was the minimal OC dimension
required to provide adequate resis-
tance to crowns. In a review by Good-
acre et al
21
on the principles of tooth
preparation, 3 mm was proposed as
the minimal OC dimension for anteri-
or teeth and premolars, and 4 mm for
molars. These values were determined
based on calculations of critical con-
vergence angles.
Adequate retention and resistance
form must be incorporated into the
design of the tooth preparation. In
most circumstances, however, teeth
in need of complete coverage restora-
tions have lost substantial tooth struc-
ture. In these situations, a foundation
restoration is indicated to permit de-
velopment of retention and resistance
form.
22
These foundation restorations
replace coronal tooth structure that
was lost as a result of caries, previ-
ous restorations, or tooth fracture.
Shillingburg et al
1
also suggested the
placement of a core reconstruction or
foundation restoration when one half
or more of the coronal tooth structure
is missing. For endodontically treated
teeth, a core alone may be placed if
adequate tooth structure remains.
23
For endodontically treated teeth with
moderate to severe tooth structure
loss, a cast post-and-core restoration
may be placed prior to the definitive
restoration.
24
Posts and cores can transfer occlu-
sal forces intraradicularly, with resul-
tant predisposition to vertical fracture
of the root.
25,26
In 1961, Rosen
27
pro-
posed the concept of an extracoronal
brace to prevent tooth fracture. The
term ferrule effect was used to de-
scribe this 360-degree ring of cast
metal, and extension of the defini-
tive restoration at least 2 mm apical
to the junction of the core and re-
maining tooth structure was recom-
mended.
28
Over the years, numerous
studies have investigated the ferrule
effect.
28-31
These studies demon-
strated that to maximize the ferrule
effect, the clinician should retain as
much tooth structure as possible. A
minimum of 1.5-2 mm of intact tooth
structure above the crown margin has
been proposed as a guideline. If the
tooth to be restored is severely dam-
aged, surgical crown lengthening
32
or orthodontic extrusion
33
should be
considered to establish a ferrule.
Few studies have evaluated the ef-
fect of different ferrule heights on en-
hancing resistance form.
34-38
Pereira et
al
36
compared the fracture strengths
of endodontically treated teeth us-
ing prefabricated stainless steel posts,
composite resin cores, and varying
ferrule heights. The authors mea-
sured fracture resistance on teeth
with 0-mm, 1-mm, 2-mm, and 3-mm
ferrule heights and found that an in-
creased amount of coronal dentin
significantly increased the fracture re-
sistance. Another study by de Oliveira
et al
37
tested teeth with similar ferrule
heights. The teeth were restored with
carbon fiber posts, composite resin
cores, and cast crowns. The authors
found no significant difference in
fracture resistance, and hypothesized
that minimal differences in the elas-
tic moduli of the carbon fiber post
and dentin resulted in the forces be-
ing distributed similarly along the
length of the post, regardless of the
ferrule height. Al-Wahadni and Gut-
teridge
38
also investigated the fracture
resistance of teeth restored with cast
posts and partial cores supported by
different ferrule heights. The authors
concluded that a 3-mm ferrule height
had a significantly higher resistance
to fracture compared to control teeth
with a 0-mm ferrule, whereas greater
ferrule heights did not produce statis-
tically significant improvements.
The purpose of this study was to
evaluate the load fatigue performance
of teeth restored with posts and cores,
with varying tooth heights. These
were compared with similar groups
having no posts and cores. The null
hypothesis was that the load fatigue
performance of teeth restored with
posts and cores would not be differ-
ent from those without posts and
cores. The secondary purpose was
to determine whether a critical tooth
height existed at which the placement
of a foundation restoration resulted
in no significant difference in the load
fatigue performance. The secondary
null hypothesis was that the place-
ment of a foundation restoration for
any given tooth height would result in
no difference in load fatigue perfor-
mance when compared to no founda-
tion restoration.
MATERIAL AND METHODS
Human first and second premo-
lars, extracted for orthodontic reasons,
were used in this study. The criteria for
selection were the presence of a single
canal, absence of cracks or fractures, no
evidence of caries or restorations, and
no previous endodontic treatment. The
teeth were stored in 0.5% chloramine-T
solution (Chloramine T; Merck KGaA,
Darmstadt, Germany) for 1 week, fol-
lowed by storage in distilled water.
The buccopalatal dimensions of
the teeth were measured using an
electronic vernier caliper (Absolute
320 Volume 104 Issue 5
The Journal of Prosthetic Dentistry
321 November 2010
Uy et al Uy et al
Digimatic Caliper; Mitutoyo Corp,
Kanagawa, Japan) with an accuracy
of 0.02 mm and repeatability of
0.01 mm. Three measurements were
made at the greatest buccopalatal
width of the specimen, and the aver-
age was determined. The teeth were
then ranked according to decreasing
dimension. The ranked teeth were
divided into 6 groups as follows: the
first tooth was assigned to group A, the
second to group B, the third to group
C, the fourth to group D, the fifth to
group E, the sixth to group F, the sev-
enth to group F, the eighth to group
E, the ninth to group D, the tenth to
group C, the eleventh to group B, and
the twelfth to group A. This procedure
was repeated until each group had 10
teeth. Each group was then assigned to
1 of 6 test groups. A 1-way analysis of
variance (ANOVA) showed no signifi-
cant difference among the buccopala-
tal widths of the teeth in the 6 groups.
Endodontic treatment was per-
formed with a crown-down procedure
to a file size of 40 (K-Flex Files; Sybron
Endo, Orange, Calif ). After intermit-
tent rinsing with 1% sodium hypo-
chlorite solution (Miltons Solution;
Milton Pharmaceuticals, Carole Park,
Australia), root canal obturation was
done using the lateral condensation
technique with gutta-percha (Dent-
sply Asia, Wong Chuk Hang, Hong
Kong) and root canal sealer (Roth
Root Canal Cement; Roth Intl Ltd,
Chicago, Ill).
Brass cylinders were machined to
retain the specimens during testing.
The cemento-enamel junction (CEJ)
of each specimen was outlined with
a permanent marker. Then a mark
was made 3 mm below the CEJ at the
midpoint of the buccal and palatal
surfaces. These 2 marks were con-
nected with a circumferential line to
designate bone level. The specimen
was then mounted using acrylic resin
(GC Pattern Resin; GC Corp, Tokyo,
Japan) into the brass cylinder.
30,31
The
circumferential line designating the
bone level was positioned flush with
the top of the brass cylinder. Prior to
embedment, 2 notches were made on
the specimen root slightly below the
bone level line to enhance tooth re-
tention within the acrylic resin.
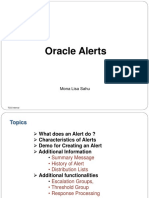
Six test groups were fabricated ac-
cording to the specifications shown
in Figure 1. As shown in this figure,
there were 2 general groups, 1 with-
out foundation restorations, and the
other with foundation restorations.
For the former, 3 tooth heights were
studied, 2, 3, and 4 mm above the
finish line. The group with foundation
restorations also had tooth heights of
2, 3, and 4 mm, but with correspond-
ing foundation heights of 4, 3, and
2 mm. The post length for these 3
groups remained constant at 8 mm.
The first group, 2TH, was prepared
to a tooth height of 2 mm. Two marks
were made 2 mm occlusal to the CEJ
at the midpoint of the buccal and
palatal surfaces. These marks were
connected with a circumferential line
that designated the tooth prepara-
tion height. Occlusal reduction to the
preparation height was accomplished
using a high-speed handpiece (KaVo
BELLAtorque Mini; KaVo Dental,
Charlotte, NC) and a fissure rotary cut-
ting instrument (NTI Diamond Instru-
ments, 856-016C; NTI Kahla-GmbH,
Thuringia, Germany). Each specimen
was then prepared with a buccopala-
tal convergence angle of 20 degrees,
using a tooth preparation guide.
39
The
mesial and distal walls were prepared
freehand using the same fissure rotary
cutting instrument, maintaining the
cutting instrument parallel to the long
axis of the tooth specimen. The direc-
tion of loading on the specimens was in
a buccopalatal direction; therefore, the
taper of the proximal surfaces was not
critical. Lastly, the preparations were
finished using a fine fissure rotary cut-
ting instrument (NTI Diamond Instru-
ments, 856-016F; NTI-Kahla GmbH).
Groups 3TH and 4TH were pre-
pared to a preparation height of 3
mm and 4 mm, respectively, using
a procedure similar to that used for
group 2TH. Group 2TH+4F was pre-
pared to a tooth height of 2 mm but
with a foundation height of 4 mm.
Tooth preparation was the same as
that for group 2TH. The post space
was then prepared using twist drills
(ParaPost Drills; Coltne/Whaledent
AG, Altsttten, Switzerland) to a de-
finitive diameter of 1.25 mm and a
depth of 8 mm from the prepared flat
surface. Titanium posts (ParaPost XP;
Coltne/Whaledent AG) were short-
ened to a length of 11 mm, allowing
3 mm of the post to extend above the
occlusal surface of the specimens.
1 Six test groups showing different tooth heights (TH) and
foundation heights (F) in millimeters.
The posts were then cemented with
zinc phosphate cement (HY-Bond Zinc
Phosphate Cement; Shofu, Inc, Kyoto,
Japan). Following setting of the post
cement, the occlusal surfaces of these
specimens were etched (All-Etch; Bisco
Inc, Schaumburg, Ill) and bonded (All-
Bond 2; Bisco, Inc) following the manu-
facturers directions. Base and catalyst
dual-polymerizing agents (Bis-Core; Bis-
co, Inc) were mixed into a uniform paste
and placed on the occlusal surface
of the specimens. Using preformed
crown molds (Frasaco Strip Crown
Forms; Frasaco GmbH, Tettnang, Ger-
many), the core was developed to 4
mm in height. After polymerization,
the core was prepared to maintain the
buccopalatal convergence angle of 20
degrees. Next, the occlusal height was
refined to achieve the desired prepa-
ration height of 6 mm (2-mm tooth
height plus 4-mm core height).
For group 3TH+3F, both tooth
and post space preparations were
similar to those of group 2TH+4F,
with the exception that the titanium
post (Parapost XP; Coltne/Whale-
dent AG) extended 2 mm above the
occlusal surface of the specimens.
The core was then developed to 3 mm
in height, resulting in a preparation
height of 6 mm (3-mm tooth height
plus 3-mm core height).
Again, for group 4TH+2F, both
tooth and post space prepara-
tions were similar to those of group
2TH+4F, with the exception that the
Parapost titanium post (Coltne/
Whaledent AG) extended 1 mm above
the occlusal surface of the specimens.
The core was then developed to 2 mm
in height, resulting in a preparation
height of 6 mm (4-mm tooth height
plus 2-mm core height).
Custom trays were fabricated
from acrylic resin (Shofu Tray Resin II;
Shofu, Inc). Impressions of each spec-
imen were made using a dual-phase
technique with light- and heavy-body
vinyl polysiloxane (Aquasil; Dentsply
DeTrey, Konstanz, Germany). Care
was taken to register part of the outer
surface of the machined brass cylin-
der. Type IV stone (Silky-Rock; Whip
Mix Corp, Louisville, Ky) was poured
into the impressions and allowed to
polymerize for 24 hours. Two coats of
die spacer (Trufit Die Spacer; George
Taub Products & Fusion Co, Jersey
City, NJ) and 1 coat of die hardener
(Stone Die and Plaster Hardener Res-
in; George Taub Products & Fusion
Co) were applied to each die. A cus-
tom waxing index
30,31
allowed fabrica-
tion of wax copings (Crowax; Renfert
GmbH, Hilzingen, Germany) on the
dies, which standardized the loca-
tion of a palatal notch 8 mm verti-
cally above the buccal finish line. This
notch located the point of applica-
tion of the fatigue load.
30,31
Upon re-
moval from the custom waxing index,
the wax pattern crown contours were
refined using x20 magnification (SZ-
FLR; Olympus Corp, Tokyo, Japan).
All of the wax patterns were in-
vested within 15 minutes of margin
refinement in a phosphate-bonded
investment (Cera-Fina; Whip Mix
Corp). The crowns were cast in a
noble alloy (Olympia; J. F. Jelenko &
Co, Armonk, NY). After divesting, the
crowns were inspected for fit under
x20 magnification (SZ-FLR; Olympus
Corp). Once fit had been ascertained,
the internal surfaces of the crowns
were airborne-particle abraded with
50-m aluminum oxide under 0.29
MPa. The crowns were cemented with
zinc phosphate cement (HY-Bond
Zinc Phosphate Cement; Shofu, Inc).
All teeth were pumiced prior to ce-
mentation, and the cement was mixed
according to the manufacturers in-
structions. Each crown was held in
place on the tooth for 10 minutes un-
der finger pressure.
Twenty-four hours after crown
cementation, a strain gauge (model
EA-05-050AH-120 LE; Vishay Micro-
Measurements, Raleigh, NC) was
placed on the palatal surface of the
crown-tooth interface. Prior to bond-
ing, the area was lightly buffed with
finishing discs (Sof-Lex; 3M ESPE,
St. Paul, Minn) and wiped with 95%
alcohol. The bonding surface of the
strain gauge was also cleaned with
alcohol. Bonding was achieved with
an adhesive (DP-460 Epoxy Adhe-
sive; 3M ESPE), ensuring that the
strain gauge grid was centered over
the crown-tooth interface. The strain
gauge cement was allowed to set for a
minimum of 24 hours before fatigue
testing. Following adhesive set, tray
adhesive (Caulk Tray Adhesive; Dent-
sply Caulk, Milford, Del) was painted
over the strain gauge to ensure water
exclusion.
The fatigue loading machine used
was similar in design to that used in
several studies at the University of
Washington, and has been described
previously.
30,31,39-41
To closely approxi-
mate in vivo loading conditions, each
specimen was subjected to a fatigue
load of 58.8 N on the loading notch
39
at a frequency of 75 cycles/min. The
load was applied at an angle of 135
degrees to the long axis of the tooth.
A positioning jig was used to hold
each specimen in this orientation dur-
ing testing.
39
Specimen failure or preliminary
failure was defined as the propaga-
tion of a crack in or around the luting
cement layer.
30,31
This was monitored
by the strain gauge on the specimen.
The strain monitoring and chart am-
plitude recording methodology have
been previously described.
39
When the
chart output demonstrated a signifi-
cant change, this verified preliminary
failure,
30,31,39-41
and the fatigue load-
ing machine was stopped. The upper
limit for testing was set at 500,000 cy-
cles. If a specimen reached this cycle
count without preliminary failure of
the cement, the test was stopped and
the cycles reported as 500,000.
The dependent variable recorded
was the number of load cycles re-
quired to induce preliminary failure.
This variable was subjected to 1-way
ANOVA to determine significant
differences among the test groups
(=.05). The Tukey Honestly Signifi-
cant Difference (HSD) multiple com-
parison test was used to determine
significant differences between the
individual groups. The data were ana-
lyzed using statistical software (SPSS
16.0; SPSS, Inc, Chicago, Ill).
320 Volume 104 Issue 5
The Journal of Prosthetic Dentistry
321 November 2010
Uy et al Uy et al
Digimatic Caliper; Mitutoyo Corp,
Kanagawa, Japan) with an accuracy
of 0.02 mm and repeatability of
0.01 mm. Three measurements were
made at the greatest buccopalatal
width of the specimen, and the aver-
age was determined. The teeth were
then ranked according to decreasing
dimension. The ranked teeth were
divided into 6 groups as follows: the
first tooth was assigned to group A, the
second to group B, the third to group
C, the fourth to group D, the fifth to
group E, the sixth to group F, the sev-
enth to group F, the eighth to group
E, the ninth to group D, the tenth to
group C, the eleventh to group B, and
the twelfth to group A. This procedure
was repeated until each group had 10
teeth. Each group was then assigned to
1 of 6 test groups. A 1-way analysis of
variance (ANOVA) showed no signifi-
cant difference among the buccopala-
tal widths of the teeth in the 6 groups.
Endodontic treatment was per-
formed with a crown-down procedure
to a file size of 40 (K-Flex Files; Sybron
Endo, Orange, Calif ). After intermit-
tent rinsing with 1% sodium hypo-
chlorite solution (Miltons Solution;
Milton Pharmaceuticals, Carole Park,
Australia), root canal obturation was
done using the lateral condensation
technique with gutta-percha (Dent-
sply Asia, Wong Chuk Hang, Hong
Kong) and root canal sealer (Roth
Root Canal Cement; Roth Intl Ltd,
Chicago, Ill).
Brass cylinders were machined to
retain the specimens during testing.
The cemento-enamel junction (CEJ)
of each specimen was outlined with
a permanent marker. Then a mark
was made 3 mm below the CEJ at the
midpoint of the buccal and palatal
surfaces. These 2 marks were con-
nected with a circumferential line to
designate bone level. The specimen
was then mounted using acrylic resin
(GC Pattern Resin; GC Corp, Tokyo,
Japan) into the brass cylinder.
30,31
The
circumferential line designating the
bone level was positioned flush with
the top of the brass cylinder. Prior to
embedment, 2 notches were made on
the specimen root slightly below the
bone level line to enhance tooth re-
tention within the acrylic resin.
Six test groups were fabricated ac-
cording to the specifications shown
in Figure 1. As shown in this figure,
there were 2 general groups, 1 with-
out foundation restorations, and the
other with foundation restorations.
For the former, 3 tooth heights were
studied, 2, 3, and 4 mm above the
finish line. The group with foundation
restorations also had tooth heights of
2, 3, and 4 mm, but with correspond-
ing foundation heights of 4, 3, and
2 mm. The post length for these 3
groups remained constant at 8 mm.
The first group, 2TH, was prepared
to a tooth height of 2 mm. Two marks
were made 2 mm occlusal to the CEJ
at the midpoint of the buccal and
palatal surfaces. These marks were
connected with a circumferential line
that designated the tooth prepara-
tion height. Occlusal reduction to the
preparation height was accomplished
using a high-speed handpiece (KaVo
BELLAtorque Mini; KaVo Dental,
Charlotte, NC) and a fissure rotary cut-
ting instrument (NTI Diamond Instru-
ments, 856-016C; NTI Kahla-GmbH,
Thuringia, Germany). Each specimen
was then prepared with a buccopala-
tal convergence angle of 20 degrees,
using a tooth preparation guide.
39
The
mesial and distal walls were prepared
freehand using the same fissure rotary
cutting instrument, maintaining the
cutting instrument parallel to the long
axis of the tooth specimen. The direc-
tion of loading on the specimens was in
a buccopalatal direction; therefore, the
taper of the proximal surfaces was not
critical. Lastly, the preparations were
finished using a fine fissure rotary cut-
ting instrument (NTI Diamond Instru-
ments, 856-016F; NTI-Kahla GmbH).
Groups 3TH and 4TH were pre-
pared to a preparation height of 3
mm and 4 mm, respectively, using
a procedure similar to that used for
group 2TH. Group 2TH+4F was pre-
pared to a tooth height of 2 mm but
with a foundation height of 4 mm.
Tooth preparation was the same as
that for group 2TH. The post space
was then prepared using twist drills
(ParaPost Drills; Coltne/Whaledent
AG, Altsttten, Switzerland) to a de-
finitive diameter of 1.25 mm and a
depth of 8 mm from the prepared flat
surface. Titanium posts (ParaPost XP;
Coltne/Whaledent AG) were short-
ened to a length of 11 mm, allowing
3 mm of the post to extend above the
occlusal surface of the specimens.
1 Six test groups showing different tooth heights (TH) and
foundation heights (F) in millimeters.
The posts were then cemented with
zinc phosphate cement (HY-Bond Zinc
Phosphate Cement; Shofu, Inc, Kyoto,
Japan). Following setting of the post
cement, the occlusal surfaces of these
specimens were etched (All-Etch; Bisco
Inc, Schaumburg, Ill) and bonded (All-
Bond 2; Bisco, Inc) following the manu-
facturers directions. Base and catalyst
dual-polymerizing agents (Bis-Core; Bis-
co, Inc) were mixed into a uniform paste
and placed on the occlusal surface
of the specimens. Using preformed
crown molds (Frasaco Strip Crown
Forms; Frasaco GmbH, Tettnang, Ger-
many), the core was developed to 4
mm in height. After polymerization,
the core was prepared to maintain the
buccopalatal convergence angle of 20
degrees. Next, the occlusal height was
refined to achieve the desired prepa-
ration height of 6 mm (2-mm tooth
height plus 4-mm core height).
For group 3TH+3F, both tooth
and post space preparations were
similar to those of group 2TH+4F,
with the exception that the titanium
post (Parapost XP; Coltne/Whale-
dent AG) extended 2 mm above the
occlusal surface of the specimens.
The core was then developed to 3 mm
in height, resulting in a preparation
height of 6 mm (3-mm tooth height
plus 3-mm core height).
Again, for group 4TH+2F, both
tooth and post space prepara-
tions were similar to those of group
2TH+4F, with the exception that the
Parapost titanium post (Coltne/
Whaledent AG) extended 1 mm above
the occlusal surface of the specimens.
The core was then developed to 2 mm
in height, resulting in a preparation
height of 6 mm (4-mm tooth height
plus 2-mm core height).
Custom trays were fabricated
from acrylic resin (Shofu Tray Resin II;
Shofu, Inc). Impressions of each spec-
imen were made using a dual-phase
technique with light- and heavy-body
vinyl polysiloxane (Aquasil; Dentsply
DeTrey, Konstanz, Germany). Care
was taken to register part of the outer
surface of the machined brass cylin-
der. Type IV stone (Silky-Rock; Whip
Mix Corp, Louisville, Ky) was poured
into the impressions and allowed to
polymerize for 24 hours. Two coats of
die spacer (Trufit Die Spacer; George
Taub Products & Fusion Co, Jersey
City, NJ) and 1 coat of die hardener
(Stone Die and Plaster Hardener Res-
in; George Taub Products & Fusion
Co) were applied to each die. A cus-
tom waxing index
30,31
allowed fabrica-
tion of wax copings (Crowax; Renfert
GmbH, Hilzingen, Germany) on the
dies, which standardized the loca-
tion of a palatal notch 8 mm verti-
cally above the buccal finish line. This
notch located the point of applica-
tion of the fatigue load.
30,31
Upon re-
moval from the custom waxing index,
the wax pattern crown contours were
refined using x20 magnification (SZ-
FLR; Olympus Corp, Tokyo, Japan).
All of the wax patterns were in-
vested within 15 minutes of margin
refinement in a phosphate-bonded
investment (Cera-Fina; Whip Mix
Corp). The crowns were cast in a
noble alloy (Olympia; J. F. Jelenko &
Co, Armonk, NY). After divesting, the
crowns were inspected for fit under
x20 magnification (SZ-FLR; Olympus
Corp). Once fit had been ascertained,
the internal surfaces of the crowns
were airborne-particle abraded with
50-m aluminum oxide under 0.29
MPa. The crowns were cemented with
zinc phosphate cement (HY-Bond
Zinc Phosphate Cement; Shofu, Inc).
All teeth were pumiced prior to ce-
mentation, and the cement was mixed
according to the manufacturers in-
structions. Each crown was held in
place on the tooth for 10 minutes un-
der finger pressure.
Twenty-four hours after crown
cementation, a strain gauge (model
EA-05-050AH-120 LE; Vishay Micro-
Measurements, Raleigh, NC) was
placed on the palatal surface of the
crown-tooth interface. Prior to bond-
ing, the area was lightly buffed with
finishing discs (Sof-Lex; 3M ESPE,
St. Paul, Minn) and wiped with 95%
alcohol. The bonding surface of the
strain gauge was also cleaned with
alcohol. Bonding was achieved with
an adhesive (DP-460 Epoxy Adhe-
sive; 3M ESPE), ensuring that the
strain gauge grid was centered over
the crown-tooth interface. The strain
gauge cement was allowed to set for a
minimum of 24 hours before fatigue
testing. Following adhesive set, tray
adhesive (Caulk Tray Adhesive; Dent-
sply Caulk, Milford, Del) was painted
over the strain gauge to ensure water
exclusion.
The fatigue loading machine used
was similar in design to that used in
several studies at the University of
Washington, and has been described
previously.
30,31,39-41
To closely approxi-
mate in vivo loading conditions, each
specimen was subjected to a fatigue
load of 58.8 N on the loading notch
39
at a frequency of 75 cycles/min. The
load was applied at an angle of 135
degrees to the long axis of the tooth.
A positioning jig was used to hold
each specimen in this orientation dur-
ing testing.
39
Specimen failure or preliminary
failure was defined as the propaga-
tion of a crack in or around the luting
cement layer.
30,31
This was monitored
by the strain gauge on the specimen.
The strain monitoring and chart am-
plitude recording methodology have
been previously described.
39
When the
chart output demonstrated a signifi-
cant change, this verified preliminary
failure,
30,31,39-41
and the fatigue load-
ing machine was stopped. The upper
limit for testing was set at 500,000 cy-
cles. If a specimen reached this cycle
count without preliminary failure of
the cement, the test was stopped and
the cycles reported as 500,000.
The dependent variable recorded
was the number of load cycles re-
quired to induce preliminary failure.
This variable was subjected to 1-way
ANOVA to determine significant
differences among the test groups
(=.05). The Tukey Honestly Signifi-
cant Difference (HSD) multiple com-
parison test was used to determine
significant differences between the
individual groups. The data were ana-
lyzed using statistical software (SPSS
16.0; SPSS, Inc, Chicago, Ill).
322 Volume 104 Issue 5
The Journal of Prosthetic Dentistry
323 November 2010
Uy et al Uy et al
RESULTS
Figure 2 shows the mean values and
standard deviations for all 6 groups.
Three specimens reached the upper
limit of 500,000 cycles; 2 specimens
belonged to group 4TH+2F, while 1
specimen belonged to group 3TH+3F.
The 1-way ANOVA showed significant
differences among the test groups
(P<.001, df=5, F=24.8). Group
4TH+2F had the highest number of cy-
cles to preliminary failure (437,701),
while group 2TH had the lowest num-
ber of cycles (53,806). The Tukey
HSD multiple comparison tests were
performed to compare groups with
and without foundation restorations.
As shown in Figure 2, the 2-mm tooth
height preparations with and with-
out foundation restorations (groups
2TH+4F and 2TH) were significantly
different (P<.001). This was also true
for both the 3-mm (groups 3TH+3F
and 3TH) and 4-mm (groups 4TH+2F
and 4TH) tooth height preparations
(P<.001).
DISCUSSION
The results of this study support re-
jection of the null hypothesis that the
load fatigue performance of teeth re-
stored with posts and cores would not
be different from the load fatigue per-
formance of those without posts and
cores. It was evident that placement
of foundation restorations resulted
in a higher number of cycles to pre-
liminary failure. This is in agreement
with the popular view that foundation
restorations permit development of
resistance and retention form.
22
The
results of this study also reinforce the
concepts that crown lengthening sur-
gery, elective root canal therapy, and
placement of foundation restorations
should improve the serviceability of
the fixed restorations in teeth that re-
quire cuspal coverage.
22-24,32,33
A study by Pereira et al
36
found
that fracture resistance increased with
increasing ferrule heights. Fracture re-
sistance was measured by static load-
ing of the specimens in a universal
testing machine. The authors tested
endodontically treated canines with
prefabricated stainless steel posts
and cores and cast crowns. Another
study by de Oliveira et al
37
had dif-
fering results. These investigators
also tested endodontically treated
canines with varying ferrule heights,
restored with prefabricated carbon fi-
ber posts and cores and cast crowns.
The authors hypothesized that mini-
mal differences in the elastic moduli
of carbon fiber posts and dentin re-
sulted in a more even distribution of
stress, thereby resulting in no signifi-
cant differences in the fracture resis-
tance. Neither study compared teeth
with and without foundation restora-
tions. In the present study, the load
fatigue performance was not signifi-
cantly increased with increasing fer-
rule heights, although the numbers
of cycles to preliminary failure were
progressively higher. This lack of sta-
tistical difference could be due to the
large standard deviations seen among
the groups (Fig. 2), owing to factors
such as tooth variability, and varying
locations of discontinuities in the ce-
ment layer.
39
The results of the current study
also support rejection of the second-
ary null hypothesis: that the place-
ment of a foundation restoration for
any given tooth height would result in
no difference in load fatigue perfor-
mance when compared to no founda-
tion restoration. In this study, there
was no critical tooth height at which
placement of a foundation restoration
resulted in no significant difference
in the load fatigue performance. This
study tested tooth heights of 2, 3, and
4 mm. Greater tooth heights were not
tested as they were deemed not to re-
quire foundation restorations.
For the current test series, 3 speci-
mens reached the upper limit of
500,000 cycles. Although the limit of
500,000 cycles was initially chosen as
an arbitrary number, it was deemed
appropriate as the majority of the
specimens failed within this limit.
Initially, the authors planned to
test groups of specimens with varying
core heights, but no posts. However,
2 Mean cycles to preliminary failure for test groups. Cement groups with dif-
ferent lowercase letters denote statistically significant differences (P<.05).
60
M
e
a
n
C
y
c
l
e
s
x
1
0
4
40
50
30
20
10
0
2TH 3TH 4TH 2TH+4F 3TH+3F 4TH+2F
a b c a b c
problems were encountered during
specimen preparation. The composite
cores dislodged from the teeth during
various stages of specimen prepara-
tion, resulting in a decision to exclude
these groups altogether. This is likely to
have an important clinical implication.
In badly damaged teeth and teeth with
short clinical crown heights, place-
ment of cores alone, without crown
lengthening surgery or elective root
canal therapy and post placement,
may result in a reduced success rate.
A study by Sahafi et al
35
tested the ef-
fect of different posts and a core on
the resistance to cyclic loading of cast
crowns. One of the groups tested in-
cluded teeth with core foundations of
3 mm, and no posts. The authors did
not report any problems during speci-
men preparation.
A limitation of this study is the
large standard deviation of the cycle
counts to preliminary failure. This
may be due to variations in the prepa-
ration of specimens. To minimize dif-
ferences, a single operator performed
all of the clinical and laboratory pro-
cedures for all specimens. Disconti-
nuities in the cement layer, such as
the presence of bubbles and lack of
wetting of the dentin and/or crown
surfaces, may also have contributed
to the large standard deviation. These
discontinuities affect the rate at
which fatigue failure occurs, thereby
resulting in variations in the number
of cycles to failure.
39
Furthermore, no
formal power analysis was performed
to determine adequate sample size.
In this study, each specimen was pre-
pared to a total occlusal convergence
of 20 degrees. As TOC has been pro-
posed to affect the resistance form of
crowns, it would be beneficial in the
future to investigate the effect of vary-
ing TOC angles on the load fatigue
performance of teeth restored with
and without foundation restorations.
CONCLUSIONS
Within the limitations of this in
vitro study, the following conclusions
were drawn:
1. For a given tooth height, teeth
restored with foundation restorations
had a significantly higher number
of cycles to preliminary failure than
those with no foundation restoration.
2. Comparing teeth of the same
height, with and without a founda-
tion restoration, there was no critical
tooth height for which there was no
significant difference in load fatigue
performance.
REFERENCES
1. Shillingburg HT, Hobo S, Whitsett LD, Ja-
cobi R, Brackett SE. Fundamentals of fixed
prosthodontics. 3
rd
ed. Chicago: Quintes-
sence; 1997. p. 120, 139-42, 151-2.
2. Potts RG, Shillingburg HT Jr, Duncanson
MG Jr. Retention and resistance of prepara-
tions for cast restorations. J Prosthet Dent
1980;43:303-8.
3. The glossary of prosthodontic terms. J
Prosthet Dent 2005;94:69.
4. Jrgensen KD. The relationship between re-
tention and convergence angle in cemented
veneer crowns. Acta Odontol Scand
1955;13:35-40.
5. Kaufman EG, Coehlo DH, Colin L. Factors
influencing the retention of cemented gold
castings. J Prosthet Dent 1961;11:487-502.
6. Reisbick MH, Shillingburg HT Jr. Effect of
preparation geometry on retention and
resistance of cast gold restorations. J Calif
Dent Assoc 1975;3:51-9.
7. Woolsey GD, Matich JA. The effect of axial
grooves on the resistance form of cast restora-
tions. J Am Dent Assoc 1978;97:978-80.
8. Zuckerman GR. Resistance form for the
complete veneer crown: principles of design
and analysis. Int J Prosthodont 1988;1:302-7.
9. Proussaefs P, Campagni W, Bernal G,
Goodacre C, Kim J. The effectiveness of
auxiliary features on a tooth preparation
with inadequate resistance form. J Prosthet
Dent 2004;91:33-41.
10.Weed RM, Baez RJ. A method for determin-
ing adequate resistance form of complete
cast crown preparations. J Prosthet Dent
1984;52:330-4.
11.Wiskott HW, Nicholls JI, Belser UC. The
relationship between abutment taper and
resistance of cemented crowns to dynamic
loading. Int J Prosthodont 1996;9:117-39.
12.Rosenstiel SF, Land MF, Fujimoto J. Con-
temporary fixed prosthodontics. 4
th
ed. St.
Louis: Elsevier; 2006. p. 209-57.
13.Johnston JF, Dykema RW, Goodacre CJ,
Phillips RW. Johnstons modern practice in
fixed prosthodontics. 4
th
ed. Philadelphia:
WB Saunders; 1986. p. 22-34.
14.Ohm E, Silness J. The convergence angle in
teeth prepared for artificial crowns. J Oral
Rehabil 1978;5:371-5.
15.Noonan JE Jr, Goldfogel MH. Convergence
of the axial walls of full veneer crown prepa-
rations in a dental school environment. J
Prosthet Dent 1991;66:706-8.
16.Nordlander J, Weir D, Stoffer W, Ochi
S. The taper of clinical preparations for
fixed prosthodontics. J Prosthet Dent
1988;60:148-51.
17.Leempoel PJ, Lemmens PL, Snoek PA, vant
Hof MA. The convergence angle of tooth
preparations for complete crowns. J Pros-
thet Dent 1987;58:414-6.
18.Mack PJ. A theoretical and clinical inves-
tigation into the taper achieved on crown
and inlay preparations. J Oral Rehabil
1980;7:255-65.
19.Wiskott HW, Nicholls JI, Belser UC. The
effect of tooth preparation height and
diameter on the resistance of complete
crowns to fatigue loading. Int J Prosthodont
1997;10:207-15.
20.Maxwell AW, Blank LW, Pelleu GB Jr. Effect
of crown preparation height on the reten-
tion and resistance of gold castings. Gen
Dent 1990;38:200-2.
21.Goodacre CJ, Campagni WV, Aquilino SA.
Tooth preparations for complete crowns:
an art form based on scientific principles. J
Prosthet Dent 2001;85:363-76.
22.Morgano SM, Brackett SE. Foundation
restorations in fixed prosthodontics: cur-
rent knowledge and future needs. J Prosthet
Dent 1999;82:643-57.
23.Nayyar A, Walton RE, Leonard LA. An
amalgam coronal-radicular dowel and core
technique for endodontically treated poste-
rior teeth. J Prosthet Dent 1980;43:511-5.
24.Bergman B, Lundquist P, Sjgren U,
Sundquist G. Restorative and endodontic
results after treatment with cast posts and
cores. J Prosthet Dent 1989;61:10-5.
25.Guzy GE, Nicholls JI. In vitro comparison
of intact endodontically treated teeth with
and without endo-post reinforcement. J
Prosthet Dent 1979;42:39-44.
26.Trope M, Maltz DO, Tronstad L. Resis-
tance to fracture of restored endodonti-
cally treated teeth. Endod Dent Traumatol
1985;1:108-11.
27.Rosen H. Operative procedures on mutilat-
ed endodontically treated teeth. J Prosthet
Dent 1961;11:973-86.
28. Sorensen JA, Engleman MJ. Ferrule design
and fracture resistance of endodontically treated
teeth. J Prosthet Dent 1990;63:529-36.
29.Isidor F, Brndum K, Ravnholt G. The
influence of post length and crown ferrule
length on the resistance to cyclic loading
of bovine teeth with prefabricated titanium
posts. Int J Prosthodont 1999;12:78-82.
30.Libman WJ, Nicholls JI. Load fatigue of
teeth restored with cast posts and cores
and complete crowns. Int J Prosthodont
1995;8:155-61.
31.Fan P, Nicholls JI, Kois JC. Load fatigue of
five restoration modalities in structurally
compromised premolars. Int J Prosthodont
1995;8:213-20.
32.Smukler H, Chaibi M. Periodontal and
dental considerations in clinical crown
extension: a rational basis for treat-
ment. Int J Periodontics Restorative Dent
1997;17:464-77.
33.Kocadereli I, Tasman F, Gner SB. Com-
bined endodontic-orthodontic and prosth-
odontic treatment of fractured teeth. Case
report. Aust Dent J 1998;43:28-31.
322 Volume 104 Issue 5
The Journal of Prosthetic Dentistry
323 November 2010
Uy et al Uy et al
RESULTS
Figure 2 shows the mean values and
standard deviations for all 6 groups.
Three specimens reached the upper
limit of 500,000 cycles; 2 specimens
belonged to group 4TH+2F, while 1
specimen belonged to group 3TH+3F.
The 1-way ANOVA showed significant
differences among the test groups
(P<.001, df=5, F=24.8). Group
4TH+2F had the highest number of cy-
cles to preliminary failure (437,701),
while group 2TH had the lowest num-
ber of cycles (53,806). The Tukey
HSD multiple comparison tests were
performed to compare groups with
and without foundation restorations.
As shown in Figure 2, the 2-mm tooth
height preparations with and with-
out foundation restorations (groups
2TH+4F and 2TH) were significantly
different (P<.001). This was also true
for both the 3-mm (groups 3TH+3F
and 3TH) and 4-mm (groups 4TH+2F
and 4TH) tooth height preparations
(P<.001).
DISCUSSION
The results of this study support re-
jection of the null hypothesis that the
load fatigue performance of teeth re-
stored with posts and cores would not
be different from the load fatigue per-
formance of those without posts and
cores. It was evident that placement
of foundation restorations resulted
in a higher number of cycles to pre-
liminary failure. This is in agreement
with the popular view that foundation
restorations permit development of
resistance and retention form.
22
The
results of this study also reinforce the
concepts that crown lengthening sur-
gery, elective root canal therapy, and
placement of foundation restorations
should improve the serviceability of
the fixed restorations in teeth that re-
quire cuspal coverage.
22-24,32,33
A study by Pereira et al
36
found
that fracture resistance increased with
increasing ferrule heights. Fracture re-
sistance was measured by static load-
ing of the specimens in a universal
testing machine. The authors tested
endodontically treated canines with
prefabricated stainless steel posts
and cores and cast crowns. Another
study by de Oliveira et al
37
had dif-
fering results. These investigators
also tested endodontically treated
canines with varying ferrule heights,
restored with prefabricated carbon fi-
ber posts and cores and cast crowns.
The authors hypothesized that mini-
mal differences in the elastic moduli
of carbon fiber posts and dentin re-
sulted in a more even distribution of
stress, thereby resulting in no signifi-
cant differences in the fracture resis-
tance. Neither study compared teeth
with and without foundation restora-
tions. In the present study, the load
fatigue performance was not signifi-
cantly increased with increasing fer-
rule heights, although the numbers
of cycles to preliminary failure were
progressively higher. This lack of sta-
tistical difference could be due to the
large standard deviations seen among
the groups (Fig. 2), owing to factors
such as tooth variability, and varying
locations of discontinuities in the ce-
ment layer.
39
The results of the current study
also support rejection of the second-
ary null hypothesis: that the place-
ment of a foundation restoration for
any given tooth height would result in
no difference in load fatigue perfor-
mance when compared to no founda-
tion restoration. In this study, there
was no critical tooth height at which
placement of a foundation restoration
resulted in no significant difference
in the load fatigue performance. This
study tested tooth heights of 2, 3, and
4 mm. Greater tooth heights were not
tested as they were deemed not to re-
quire foundation restorations.
For the current test series, 3 speci-
mens reached the upper limit of
500,000 cycles. Although the limit of
500,000 cycles was initially chosen as
an arbitrary number, it was deemed
appropriate as the majority of the
specimens failed within this limit.
Initially, the authors planned to
test groups of specimens with varying
core heights, but no posts. However,
2 Mean cycles to preliminary failure for test groups. Cement groups with dif-
ferent lowercase letters denote statistically significant differences (P<.05).
60
M
e
a
n
C
y
c
l
e
s
x
1
0
4
40
50
30
20
10
0
2TH 3TH 4TH 2TH+4F 3TH+3F 4TH+2F
a b c a b c
problems were encountered during
specimen preparation. The composite
cores dislodged from the teeth during
various stages of specimen prepara-
tion, resulting in a decision to exclude
these groups altogether. This is likely to
have an important clinical implication.
In badly damaged teeth and teeth with
short clinical crown heights, place-
ment of cores alone, without crown
lengthening surgery or elective root
canal therapy and post placement,
may result in a reduced success rate.
A study by Sahafi et al
35
tested the ef-
fect of different posts and a core on
the resistance to cyclic loading of cast
crowns. One of the groups tested in-
cluded teeth with core foundations of
3 mm, and no posts. The authors did
not report any problems during speci-
men preparation.
A limitation of this study is the
large standard deviation of the cycle
counts to preliminary failure. This
may be due to variations in the prepa-
ration of specimens. To minimize dif-
ferences, a single operator performed
all of the clinical and laboratory pro-
cedures for all specimens. Disconti-
nuities in the cement layer, such as
the presence of bubbles and lack of
wetting of the dentin and/or crown
surfaces, may also have contributed
to the large standard deviation. These
discontinuities affect the rate at
which fatigue failure occurs, thereby
resulting in variations in the number
of cycles to failure.
39
Furthermore, no
formal power analysis was performed
to determine adequate sample size.
In this study, each specimen was pre-
pared to a total occlusal convergence
of 20 degrees. As TOC has been pro-
posed to affect the resistance form of
crowns, it would be beneficial in the
future to investigate the effect of vary-
ing TOC angles on the load fatigue
performance of teeth restored with
and without foundation restorations.
CONCLUSIONS
Within the limitations of this in
vitro study, the following conclusions
were drawn:
1. For a given tooth height, teeth
restored with foundation restorations
had a significantly higher number
of cycles to preliminary failure than
those with no foundation restoration.
2. Comparing teeth of the same
height, with and without a founda-
tion restoration, there was no critical
tooth height for which there was no
significant difference in load fatigue
performance.
REFERENCES
1. Shillingburg HT, Hobo S, Whitsett LD, Ja-
cobi R, Brackett SE. Fundamentals of fixed
prosthodontics. 3
rd
ed. Chicago: Quintes-
sence; 1997. p. 120, 139-42, 151-2.
2. Potts RG, Shillingburg HT Jr, Duncanson
MG Jr. Retention and resistance of prepara-
tions for cast restorations. J Prosthet Dent
1980;43:303-8.
3. The glossary of prosthodontic terms. J
Prosthet Dent 2005;94:69.
4. Jrgensen KD. The relationship between re-
tention and convergence angle in cemented
veneer crowns. Acta Odontol Scand
1955;13:35-40.
5. Kaufman EG, Coehlo DH, Colin L. Factors
influencing the retention of cemented gold
castings. J Prosthet Dent 1961;11:487-502.
6. Reisbick MH, Shillingburg HT Jr. Effect of
preparation geometry on retention and
resistance of cast gold restorations. J Calif
Dent Assoc 1975;3:51-9.
7. Woolsey GD, Matich JA. The effect of axial
grooves on the resistance form of cast restora-
tions. J Am Dent Assoc 1978;97:978-80.
8. Zuckerman GR. Resistance form for the
complete veneer crown: principles of design
and analysis. Int J Prosthodont 1988;1:302-7.
9. Proussaefs P, Campagni W, Bernal G,
Goodacre C, Kim J. The effectiveness of
auxiliary features on a tooth preparation
with inadequate resistance form. J Prosthet
Dent 2004;91:33-41.
10.Weed RM, Baez RJ. A method for determin-
ing adequate resistance form of complete
cast crown preparations. J Prosthet Dent
1984;52:330-4.
11.Wiskott HW, Nicholls JI, Belser UC. The
relationship between abutment taper and
resistance of cemented crowns to dynamic
loading. Int J Prosthodont 1996;9:117-39.
12.Rosenstiel SF, Land MF, Fujimoto J. Con-
temporary fixed prosthodontics. 4
th
ed. St.
Louis: Elsevier; 2006. p. 209-57.
13.Johnston JF, Dykema RW, Goodacre CJ,
Phillips RW. Johnstons modern practice in
fixed prosthodontics. 4
th
ed. Philadelphia:
WB Saunders; 1986. p. 22-34.
14.Ohm E, Silness J. The convergence angle in
teeth prepared for artificial crowns. J Oral
Rehabil 1978;5:371-5.
15.Noonan JE Jr, Goldfogel MH. Convergence
of the axial walls of full veneer crown prepa-
rations in a dental school environment. J
Prosthet Dent 1991;66:706-8.
16.Nordlander J, Weir D, Stoffer W, Ochi
S. The taper of clinical preparations for
fixed prosthodontics. J Prosthet Dent
1988;60:148-51.
17.Leempoel PJ, Lemmens PL, Snoek PA, vant
Hof MA. The convergence angle of tooth
preparations for complete crowns. J Pros-
thet Dent 1987;58:414-6.
18.Mack PJ. A theoretical and clinical inves-
tigation into the taper achieved on crown
and inlay preparations. J Oral Rehabil
1980;7:255-65.
19.Wiskott HW, Nicholls JI, Belser UC. The
effect of tooth preparation height and
diameter on the resistance of complete
crowns to fatigue loading. Int J Prosthodont
1997;10:207-15.
20.Maxwell AW, Blank LW, Pelleu GB Jr. Effect
of crown preparation height on the reten-
tion and resistance of gold castings. Gen
Dent 1990;38:200-2.
21.Goodacre CJ, Campagni WV, Aquilino SA.
Tooth preparations for complete crowns:
an art form based on scientific principles. J
Prosthet Dent 2001;85:363-76.
22.Morgano SM, Brackett SE. Foundation
restorations in fixed prosthodontics: cur-
rent knowledge and future needs. J Prosthet
Dent 1999;82:643-57.
23.Nayyar A, Walton RE, Leonard LA. An
amalgam coronal-radicular dowel and core
technique for endodontically treated poste-
rior teeth. J Prosthet Dent 1980;43:511-5.
24.Bergman B, Lundquist P, Sjgren U,
Sundquist G. Restorative and endodontic
results after treatment with cast posts and
cores. J Prosthet Dent 1989;61:10-5.
25.Guzy GE, Nicholls JI. In vitro comparison
of intact endodontically treated teeth with
and without endo-post reinforcement. J
Prosthet Dent 1979;42:39-44.
26.Trope M, Maltz DO, Tronstad L. Resis-
tance to fracture of restored endodonti-
cally treated teeth. Endod Dent Traumatol
1985;1:108-11.
27.Rosen H. Operative procedures on mutilat-
ed endodontically treated teeth. J Prosthet
Dent 1961;11:973-86.
28. Sorensen JA, Engleman MJ. Ferrule design
and fracture resistance of endodontically treated
teeth. J Prosthet Dent 1990;63:529-36.
29.Isidor F, Brndum K, Ravnholt G. The
influence of post length and crown ferrule
length on the resistance to cyclic loading
of bovine teeth with prefabricated titanium
posts. Int J Prosthodont 1999;12:78-82.
30.Libman WJ, Nicholls JI. Load fatigue of
teeth restored with cast posts and cores
and complete crowns. Int J Prosthodont
1995;8:155-61.
31.Fan P, Nicholls JI, Kois JC. Load fatigue of
five restoration modalities in structurally
compromised premolars. Int J Prosthodont
1995;8:213-20.
32.Smukler H, Chaibi M. Periodontal and
dental considerations in clinical crown
extension: a rational basis for treat-
ment. Int J Periodontics Restorative Dent
1997;17:464-77.
33.Kocadereli I, Tasman F, Gner SB. Com-
bined endodontic-orthodontic and prosth-
odontic treatment of fractured teeth. Case
report. Aust Dent J 1998;43:28-31.
324 Volume 104 Issue 5
The Journal of Prosthetic Dentistry Patel et al Uy et al
34.Gegauff AG. Effect of crown lengthening
and ferrule placement on static load failure
of cemented cast post-cores and crowns. J
Prosthet Dent 2000;84:169-79.
35.Sahafi A, Peutzfeldt A, Ravnholt G, Asmus-
sen E, Gotfredsen K. Resistance to cyclic
loading of teeth restored with posts. Clin
Oral Investig 2005;9:84-90.
36.Pereira JR, de Ornelas F, Conti PC, do Valle
AL. Effect of a crown ferrule on the frac-
ture resistance of endodontically treated
teeth restored with prefabricated posts. J
Prosthet Dent 2006;95:50-4.
37.de Oliveira JA, Pereira JR, Lins do Valle
A, Zogheib LV. Fracture resistance of
endodontically treated teeth with different
heights of crown ferrule restored with pre-
fabricated carbon fiber post and composite
resin core by intermittent loading. Oral
Surg Oral Med Oral Pathol Oral Radiol
Endod 2008;106:e52-7.
38.Al-Wahadni A, Gutteridge DL. An in vitro
investigation into the effects of retained
coronal dentine on the strength of a tooth
restored with a cemented post and partial
core restoration. Int Endo J 2002;35:913-8.
39.Uy JN, Lian JN, Nicholls JI, Tan KB. Load-
fatigue performance of gold crowns
luted with resin cements. J Prosthet Dent
2006;95:315-22.
40.Hsu YB, Nicholls JI, Phillips KM, Libman
WJ. Effect of core bonding on fatigue fail-
ure of compromised teeth. Int J Prostho-
dont 2002;15:175-8.
41.Fissore B, Nicholls JI, Yuodelis RA. Load
fatigue of teeth restored by a dentin bond-
ing agent and a posterior composite resin. J
Prosthet Dent 1991;65:80-5.
Corresponding author:
Dr Joanne N. Uy
Department of Restorative Dentistry
Faculty of Dentistry
National University of Singapore
5 Lower Kent Ridge Rd
SINGAPORE 119074
Fax: +6567785742
E-mail: rsdujn@nus.edu.sg
Acknowledgements
The authors thank Professor Jack Ivan Nicholls
for his invaluable guidance and help on this
project.
Copyright 2010 by the Editorial Council for
The Journal of Prosthetic Dentistry.
Clinical Implications
The new materials evaluated may prove advantageous in clinical
practice compared to traditional irreversible hydrocolloid impres-
sion material. As has been demonstrated in vitro, they are more di-
mensionally stable and exhibit better detail reproduction both when
impressed and when cast with gypsum. However, further clinical
testing may be warranted to establish this.
Statement of problem. A number of manufacturers have introduced new products that are marketed as alternatives
to irreversible hydrocolloid impression materials. However, there is a paucity of laboratory and clinical research on
these products compared to traditional irreversible hydrocolloid.
Purpose. The purpose of this study was to evaluate the detail reproduction, gypsum compatibility, and linear dimen-
sional change of 3 recently introduced impression materials designed as alternatives to irreversible hydrocolloid.
Material and methods. The tested materials were Position Penta Quick, Silgimix, and AlgiNot. An irreversible hydro-
colloid impression material, Jeltrate Plus Antimicrobial, served as the control. The parameters of detail reproduction,
gypsum compatibility, and linear dimensional change were tested in accordance with ANSI/ADA Specifications No. 18
and 19. The gypsum compatibility was tested using a type III stone (Microstone Golden) and a type IV stone (Die-
Keen Green). The data were analyzed using the Kruskal-Wallis rank test and the Mann-Whitney U test (=.05).
Results. The test materials demonstrated significantly (P<.001) better detail reproduction than the control material.
Silgimix exhibited the best compatibility with Microstone, whereas AlgiNot and Position Penta Quick exhibited the
best gypsum compatibility with Die-Keen. An incompatibility was observed over time between the Jeltrate control ma-
terial and the Microstone gypsum material. For linear dimensional change, the mean dimension of the control mate-
rial most closely approximated the distance between the lines on the test die, but it exhibited the greatest variability in
measurements. All of the test materials exhibited linear dimensional change within the ADAs accepted limit of 1.0%.
Conclusions. The 3 new impression materials exhibited better detail reproduction and less variability in linear dimen-
sional change than the irreversible hydrocolloid control. Gypsum compatibility varied with the brand of gypsum used,
with an incompatibility identified between the control material (Jeltrate Plus Antimicrobial) and Microstone related to
surface changes observed over time. (J Prosthet Dent 2010;104:325-332)
An in vitro investigation into the
physical properties of irreversible
hydrocolloid alternatives
Rishi D. Patel, BDS, MS,
a
Mathew T. Kattadiyil, DDS, MDS, MS,
b
Charles J. Goodacre, DDS, MSD,
c
and Myron S. Winer, DDS
d
Loma Linda University School of Dentistry, Loma Linda, Calif
a
Assistant Professor, Department of Restorative Dentistry.
b
Program Director, Advanced Education in Prosthodontics, Department of Restorative Dentistry.
c
Professor of Restorative Dentistry and Dean.
d
Assistant Professor, Advanced Education in Prosthodontics, Department of Restorative Dentistry.
New impression materials are mar-
keted as alternatives to irreversible hy-
drocolloid. However, there is a paucity
of laboratory and clinical research on
these materials compared to traditional
irreversible hydrocolloid.
One of the earliest studies on ir-
reversible hydrocolloid alternatives was
performed by Eames and Litvak.
1
They
investigated the irreversible hydrocol-
loid silicone material, Ultrafine (Buffalo
Dental Mfg Co, Syosset, NY). The au-
thors reported higher tear and compres-
sive strengths compared to convention-
al irreversible hydrocolloid, but there
Noteworthy Abstracts of the Current Literature
Nanostructured alumina-coated implant surface: Effect on osteoblast-related gene ex-
pression and bone-to-implant contact in vivo
Mendonca G, Mendonca DB, Simoes LG, Araujo AL, Leite ER, Duarte WR, Cooper LF, Aragao FJ.
Int J Oral Maxillofac Implants 2009;24:205-15.
Purpose. The use of nanotechnology to enhance endosseous implant surfaces may improve the clinical control of
interfacial osteoblast biology. This study investigated the inuence of a nanostructure-coated implant surface on os-
teoblast differentiation and its effects on bone-to-implant contact (BIC) and removal torque values.
Materials and Methods. Titanium disks were machined (M) or machined and subsequently treated by acid etching
(Ac) or by dipping in an aluminum oxide solution (Al
2
O
3
). Surfaces were characterized by scanning electron mi-
croscopy, atomic force microscopy, and x-ray microanalysis. For the in vitro experiment, rat mesenchymal stem cells
(rMSCs) were grown in osteogenic supplements on the disk surfaces for 3 days. Real-time polymerase chain reaction
(PCR) was used to measure mRNA levels of several gene products (bone sialoprotein, osteocalcin, osteopontin, and
RUNX-2). For the in vivo experiment, titanium implants were placed in rat tibiae and harvested after 3 to 21 days for
measurement of bone-specic mRNA levels by real-time PCR. Removal torque and BIC were measured 3 to 56 days
after placement.
Results. Average height deviation (Sa, in nm) values for M, Ac, and Al
2
O
3
implants were 86.5, 388.4, and 61.2, re-
spectively. Nanostructured Al
2
O
3
topographic features applied to machined implants promoted MSC commitment to
the osteoblast phenotype. Greater bone-specic gene expression was observed in tissues adjacent to Al
2
O
3
implants,
and associated increases in BIC and torque removal were noted.
Signicance. Nanostructured alumina may directly inuence cell behavior to enhance osseointegration.
Reprinted with permission of Quintessence Publishing.
Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Travel Sketching in Mixed Media - SuppliesDocument2 pagesTravel Sketching in Mixed Media - SuppliesClaudio Sumonte HernandezPas encore d'évaluation
- Clinical Use of A Sectional Matrix and Ring: Clinical Technique/Case ReportDocument5 pagesClinical Use of A Sectional Matrix and Ring: Clinical Technique/Case ReportClaudio Sumonte Hernandez100% (1)
- Individualized Wedge: Clinical Technique/Case ReportDocument4 pagesIndividualized Wedge: Clinical Technique/Case ReportClaudio Sumonte HernandezPas encore d'évaluation
- Effect of Different Bur Grinding On The Bond Strength of Self-Etching AdhesivesDocument7 pagesEffect of Different Bur Grinding On The Bond Strength of Self-Etching AdhesivesClaudio Sumonte HernandezPas encore d'évaluation
- The Restoration of Endodontically Treated, Single-Rooted Teeth With Cast or Direct Posts and Cores: A Systematic ReviewDocument7 pagesThe Restoration of Endodontically Treated, Single-Rooted Teeth With Cast or Direct Posts and Cores: A Systematic ReviewClaudio Sumonte HernandezPas encore d'évaluation
- The Empire Strikes Back Sketch BookDocument97 pagesThe Empire Strikes Back Sketch BookClaudio Sumonte Hernandez88% (17)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- FMF-01-10-911-302 - 100 GPM - 60 HZ Electric Motor DriveDocument1 pageFMF-01-10-911-302 - 100 GPM - 60 HZ Electric Motor DriveMarkPas encore d'évaluation
- Maths Project: Made By:-Shubham Class: - Viii-CDocument25 pagesMaths Project: Made By:-Shubham Class: - Viii-CsivaPas encore d'évaluation
- Rangkaian Om Telolet OmDocument5 pagesRangkaian Om Telolet Omwalid suwalidPas encore d'évaluation
- Calflo Heat Transfer Fluids Tech DataDocument4 pagesCalflo Heat Transfer Fluids Tech DataKhaled ElsayedPas encore d'évaluation
- Student Personal Prescriptive Path 2Document29 pagesStudent Personal Prescriptive Path 2api-377332228Pas encore d'évaluation
- Civl432 Bridge Design SummaryDocument5 pagesCivl432 Bridge Design SummarySheikh Mizanur RahmanPas encore d'évaluation
- BaseballDocument37 pagesBaseballBeeWinPas encore d'évaluation
- DLP Math 10 q1 Week 8 Day 1Document16 pagesDLP Math 10 q1 Week 8 Day 1Henel Mar100% (1)
- Copula Modeling: An Introduction For Practitioners: Pravin K. Trivedi and David M. ZimmerDocument111 pagesCopula Modeling: An Introduction For Practitioners: Pravin K. Trivedi and David M. ZimmervinizioPas encore d'évaluation
- How To Build An Offshore CraneDocument5 pagesHow To Build An Offshore CraneWestMarinePas encore d'évaluation
- Oracle Alerts: Mona Lisa SahuDocument35 pagesOracle Alerts: Mona Lisa Sahuanishokm2992Pas encore d'évaluation
- 03 - Random Effect ModelDocument10 pages03 - Random Effect ModelAdji Pelangi SaputriPas encore d'évaluation
- Lecture Slides: Shigley's Mechanical Engineering DesignDocument95 pagesLecture Slides: Shigley's Mechanical Engineering DesignpurnaPas encore d'évaluation
- Sound Intensity Level CalculationDocument10 pagesSound Intensity Level CalculationvenkateswaranPas encore d'évaluation
- KTM Tokamak Project. Present and Future Activity: January 2008Document9 pagesKTM Tokamak Project. Present and Future Activity: January 2008AB XEROXPas encore d'évaluation
- En 2014 New Brochure WebDocument20 pagesEn 2014 New Brochure WebSasa NackovicPas encore d'évaluation
- Pipe Fabrication Brochure CompressedDocument2 pagesPipe Fabrication Brochure CompressedLeDzungPas encore d'évaluation
- Weather ForecastsDocument5 pagesWeather ForecastsGianina MihăicăPas encore d'évaluation
- HW7 A SolutionsDocument6 pagesHW7 A Solutionsmmsingh91100% (1)
- Data StructuresDocument2 pagesData StructuresRavi PalPas encore d'évaluation
- Image Processing PDFDocument7 pagesImage Processing PDFRavindar Negi0% (1)
- 2003 - Serriano - Form Follows SoftwareDocument21 pages2003 - Serriano - Form Follows SoftwareMina Hazal TasciPas encore d'évaluation
- BioavailabilityDocument16 pagesBioavailabilityTyshanna JazzyNicole BariaPas encore d'évaluation
- CEH PRACTICAL NOTES - Pratik KaranDocument23 pagesCEH PRACTICAL NOTES - Pratik Karanproton infosecPas encore d'évaluation
- Cytomat Software InformationDocument34 pagesCytomat Software InformationCarlosReisPas encore d'évaluation
- Boiler Efficiency PresentationDocument13 pagesBoiler Efficiency PresentationAhmad Sabree Abdul BasitPas encore d'évaluation
- Siegel57Nonparametric PDFDocument8 pagesSiegel57Nonparametric PDFTarisna AryantiPas encore d'évaluation
- Sag 38 2 12 0709 2Document7 pagesSag 38 2 12 0709 2Yoselin GomezPas encore d'évaluation
- 2009 06 02 Library-Cache-LockDocument9 pages2009 06 02 Library-Cache-LockAbdul WahabPas encore d'évaluation
- Fork LiftDocument4 pagesFork Lifttamer goudaPas encore d'évaluation