Vous aimerez peut-être aussi
- Polycystic Kidneys: Adult PKD: ComplicationsDocument1 pagePolycystic Kidneys: Adult PKD: ComplicationsUsman Ali AkbarPas encore d'évaluation
- Urinary Tract Infection & PyelonephritisDocument3 pagesUrinary Tract Infection & PyelonephritisUsman Ali AkbarPas encore d'évaluation
- Chronic Renal Failure: Concise Long Case ApproachDocument3 pagesChronic Renal Failure: Concise Long Case ApproachUsman Ali AkbarPas encore d'évaluation
- Obstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalDocument53 pagesObstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalUsman Ali AkbarPas encore d'évaluation
- Renal Tubular Acidosis Summary - AdjDocument1 pageRenal Tubular Acidosis Summary - AdjUsman Ali AkbarPas encore d'évaluation
- King Khalid University Hospital Department of Obstetrics & Gyncology Course 481Document40 pagesKing Khalid University Hospital Department of Obstetrics & Gyncology Course 481Usman Ali AkbarPas encore d'évaluation
- DialysisDocument2 pagesDialysisUsman Ali AkbarPas encore d'évaluation
- DR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityDocument18 pagesDR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityUsman Ali AkbarPas encore d'évaluation
- Anaemia in PregnancyDocument13 pagesAnaemia in PregnancyUsman Ali AkbarPas encore d'évaluation
- GI Bleeding Team Work - 2nd EditionDocument9 pagesGI Bleeding Team Work - 2nd EditionUsman Ali AkbarPas encore d'évaluation
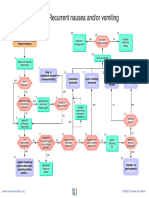
- Recurrent Nausea Andor VomitingDocument8 pagesRecurrent Nausea Andor VomitingUsman Ali AkbarPas encore d'évaluation
- Recurrent VomitingDocument16 pagesRecurrent VomitingUsman Ali AkbarPas encore d'évaluation
- When Hope DiesDocument2 pagesWhen Hope DiesUsman Ali AkbarPas encore d'évaluation
- Alas!! EmpytinessDocument2 pagesAlas!! EmpytinessUsman Ali AkbarPas encore d'évaluation
- Cord ProlapseDocument2 pagesCord ProlapseUsman Ali AkbarPas encore d'évaluation
- Organophosphate PoisoningDocument23 pagesOrganophosphate PoisoningUsman Ali AkbarPas encore d'évaluation
- Subject: Permission For Badminton Court NID, Multan: TH THDocument1 pageSubject: Permission For Badminton Court NID, Multan: TH THUsman Ali AkbarPas encore d'évaluation
- GRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Document1 pageGRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Usman Ali AkbarPas encore d'évaluation
- Through The Strange WindsDocument5 pagesThrough The Strange WindsUsman Ali AkbarPas encore d'évaluation
- Untold Stanza... : - Nasim Alam (N-61)Document1 pageUntold Stanza... : - Nasim Alam (N-61)Usman Ali AkbarPas encore d'évaluation
- Lect 1:: M2Pasysl21 Urinary SystemDocument4 pagesLect 1:: M2Pasysl21 Urinary SystemUsman Ali AkbarPas encore d'évaluation
- Death and The Mother For MergeDocument4 pagesDeath and The Mother For MergeUsman Ali AkbarPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Canine ParvovirusDocument13 pagesCanine ParvovirusSandrine WoolcockPas encore d'évaluation
- Circular Regarding Opening of School For Class X & XII - Aug 2021Document2 pagesCircular Regarding Opening of School For Class X & XII - Aug 2021Shubhangi PriyaPas encore d'évaluation
- CuesDocument8 pagesCuesFloyd SevillaPas encore d'évaluation
- Lana Moussa Aleech - Senior Project Research PaperDocument13 pagesLana Moussa Aleech - Senior Project Research Paperapi-655770614Pas encore d'évaluation
- Vaccine and ImmunityDocument32 pagesVaccine and ImmunityAlona SangamPas encore d'évaluation
- Alzheimer's DisorderDocument1 pageAlzheimer's DisorderKassandra MerrillPas encore d'évaluation
- Nursing Care PlanDocument3 pagesNursing Care PlanJASMINE JOY BADUAPas encore d'évaluation
- Infectious DiseaseDocument82 pagesInfectious DiseaseMedical videos67% (3)
- Department of Education: Republic of The PhilippinesDocument8 pagesDepartment of Education: Republic of The PhilippinesRodgen GerasolPas encore d'évaluation
- Top Dermatology Multiple Choice Questions and AnswersDocument30 pagesTop Dermatology Multiple Choice Questions and AnswersMuha RajPas encore d'évaluation
- Syphilis Staging Chart PDFDocument2 pagesSyphilis Staging Chart PDFShah NawazPas encore d'évaluation
- Lung CarcinomaDocument29 pagesLung Carcinomavinoedhnaidu_rajagopalPas encore d'évaluation
- Approach To HIV: Dr. Tejaswee BanavathuDocument46 pagesApproach To HIV: Dr. Tejaswee BanavathuAbinash SwainPas encore d'évaluation
- Asthma Treatment GuidlineDocument56 pagesAsthma Treatment GuidlineEsther OdumanyePas encore d'évaluation
- Influenzaandviral Pneumonia: Rodrigo Cavallazzi,, Julio A. RamirezDocument19 pagesInfluenzaandviral Pneumonia: Rodrigo Cavallazzi,, Julio A. Ramirezlevani memarnePas encore d'évaluation
- Actual Nursing Care PlanDocument2 pagesActual Nursing Care Planshaileene bugayongPas encore d'évaluation
- Behcet's Disease (Adamantiades Syndrome) : DefinitionDocument9 pagesBehcet's Disease (Adamantiades Syndrome) : DefinitionNuzairah AynoorPas encore d'évaluation
- 108 New Charm, CharmaidDocument3 pages108 New Charm, CharmaidAmit Kumar PandeyPas encore d'évaluation
- Epidemiology Computational ModelsDocument16 pagesEpidemiology Computational ModelsIbrahim Jynx FalamaPas encore d'évaluation
- Treatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsDocument65 pagesTreatment of Pulmonary and Extra-Pulmonary Tuberculosis in AdultsLloyd Daniel BarrantesPas encore d'évaluation
- PGI Sarip - Covid 19Document92 pagesPGI Sarip - Covid 19Junayyah Abdullah SaripPas encore d'évaluation
- Tongue DisordersDocument10 pagesTongue DisordersMohan VeerabomalaPas encore d'évaluation
- Peds McqsDocument6 pagesPeds McqssvvrajaPas encore d'évaluation
- Prevalensi Kristal Urat Dalam Urin Pada Subjek Dewasa Muda Berat Badan Lebih Dan ObesDocument5 pagesPrevalensi Kristal Urat Dalam Urin Pada Subjek Dewasa Muda Berat Badan Lebih Dan ObesBawaslu KabGianyarPas encore d'évaluation
- NCP-fluid Volume DeficitDocument4 pagesNCP-fluid Volume DeficitChrissa Mae Aranilla MayoPas encore d'évaluation
- Pathophysiology of MeningitisDocument4 pagesPathophysiology of MeningitisDaryl BalanguePas encore d'évaluation
- Khorana AA - Thromboembolism in Hospitalized Neutropenic Cancer PatientsDocument8 pagesKhorana AA - Thromboembolism in Hospitalized Neutropenic Cancer PatientsFarid RakhmanPas encore d'évaluation
- Pancreatitis, Acute: Clinical PresentationDocument26 pagesPancreatitis, Acute: Clinical Presentationapi-19641337Pas encore d'évaluation
- Jonathan B. de Guzman Olfuvalsection8: ObjectiveDocument4 pagesJonathan B. de Guzman Olfuvalsection8: ObjectiveJonathan DeguzmanPas encore d'évaluation
- Writers Cramp - A Major Conundrum: Review Article44Document7 pagesWriters Cramp - A Major Conundrum: Review Article44IJAR JOURNALPas encore d'évaluation