Vous aimerez peut-être aussi
- Analyzing Performance of Moroccan Pension Plans Using Case-Type ApproachDocument21 pagesAnalyzing Performance of Moroccan Pension Plans Using Case-Type ApproachYoussef JabirPas encore d'évaluation
- Social and Solidarity EconomyDocument4 pagesSocial and Solidarity EconomyAndrzej KlimczukPas encore d'évaluation
- Media Effects TheoriesDocument16 pagesMedia Effects TheoriesUsama Ali shahPas encore d'évaluation
- Etude de Cas Club MedDocument3 pagesEtude de Cas Club MedSimon Philippon100% (1)
- Vero Health SystemDocument11 pagesVero Health Systemzaks mainaPas encore d'évaluation
- Presentation On Health Care System ModelsDocument37 pagesPresentation On Health Care System ModelsTashi Makpen100% (1)
- Healthcare System in JapanDocument4 pagesHealthcare System in JapanBayuAkbarSyarifPas encore d'évaluation
- Health SystemsDocument8 pagesHealth SystemsLloyd SalesPas encore d'évaluation
- Health Care Schemes Project at KamineniDocument78 pagesHealth Care Schemes Project at KamineniVenugopal VutukuruPas encore d'évaluation
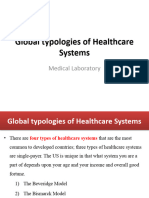
- Global Typologies of Healthcare SystemsDocument12 pagesGlobal Typologies of Healthcare SystemstewodrosbayisaPas encore d'évaluation
- Social Issue & Social Policy (Healthcare)Document10 pagesSocial Issue & Social Policy (Healthcare)my_aqilahPas encore d'évaluation
- Health InsuranceDocument46 pagesHealth InsuranceVaishali UzzielPas encore d'évaluation
- Health Insurance Programs in Korea, Israel and South Korea.Document5 pagesHealth Insurance Programs in Korea, Israel and South Korea.George MainaPas encore d'évaluation
- Subsyems Policies in USADocument13 pagesSubsyems Policies in USAWanjikuPas encore d'évaluation
- Health System: Navigation Search Organization Health Care HealthDocument10 pagesHealth System: Navigation Search Organization Health Care Healthfahri_amirullahPas encore d'évaluation
- Health System Model of VietnamDocument20 pagesHealth System Model of Vietnamsneha khuranaPas encore d'évaluation
- Health InsuranceDocument36 pagesHealth Insurancevijaya lakshmi100% (1)
- Health Insurance and Third Party Administrators Issues and ChallengesDocument25 pagesHealth Insurance and Third Party Administrators Issues and ChallengesANish AhmedPas encore d'évaluation
- Health Care in CanadaDocument13 pagesHealth Care in CanadaGayatri PandeyPas encore d'évaluation
- US Health Care SystemDocument27 pagesUS Health Care SystemmukultcsPas encore d'évaluation
- MekdishaaaaaDocument12 pagesMekdishaaaaatewodros bayisaPas encore d'évaluation
- Traductorado Público de InglésDocument5 pagesTraductorado Público de InglésTini librosPas encore d'évaluation
- Report On Health Insurance 2Document23 pagesReport On Health Insurance 2DrJaideep KumarPas encore d'évaluation
- Canada: Robert G. Evans University of British ColumbiaDocument10 pagesCanada: Robert G. Evans University of British ColumbiaDylan MartinezPas encore d'évaluation
- Indonesia: Providing Health Insurance For The Poor: Series: Social Security Extension Initatives in South East AsiaDocument7 pagesIndonesia: Providing Health Insurance For The Poor: Series: Social Security Extension Initatives in South East Asiadamai02Pas encore d'évaluation
- MCO Cession10-1Document31 pagesMCO Cession10-1monir61Pas encore d'évaluation
- Chapter 5 Health EconDocument7 pagesChapter 5 Health EconDoffCruzPas encore d'évaluation
- Unit 4: Subtopic:Documentation For Health Insurance and ClaimsDocument16 pagesUnit 4: Subtopic:Documentation For Health Insurance and ClaimsNiketa KirtiPas encore d'évaluation
- Medical Savings AccountsDocument16 pagesMedical Savings AccountsbutterPas encore d'évaluation
- Health Financing FunctionsDocument4 pagesHealth Financing FunctionsFredy GunawanPas encore d'évaluation
- GBA The Concept of HealthDocument6 pagesGBA The Concept of HealthMa'aku Bitrus AdiPas encore d'évaluation
- Paper 24Document38 pagesPaper 24ABEL KETEMAPas encore d'évaluation
- UHC With Emphasis On Third World CountriesDocument2 pagesUHC With Emphasis On Third World CountriesSalma GamalPas encore d'évaluation
- Major Stakeholders Satyajit MamDocument11 pagesMajor Stakeholders Satyajit MamAnchal thakurPas encore d'évaluation
- A Universal Health Care Plan For MissouriDocument20 pagesA Universal Health Care Plan For MissouriPhysicians for a National Health ProgramPas encore d'évaluation
- Emerging Health Insurance in India-An Overview - J AnithaDocument17 pagesEmerging Health Insurance in India-An Overview - J AnithaSwayam Suraj NayakPas encore d'évaluation
- HSP FacilitiesppDocument31 pagesHSP Facilitiesppapi-308826929Pas encore d'évaluation
- National Health Insurance: Drawing Lessons From South KoreaDocument6 pagesNational Health Insurance: Drawing Lessons From South Koreaamdeepbhatia8489Pas encore d'évaluation
- Hi 225 FinalpaperDocument11 pagesHi 225 Finalpaperapi-708689221Pas encore d'évaluation
- Sik Weny LoboDocument15 pagesSik Weny LobonoviPas encore d'évaluation
- Health Systems 2009 20aug ADocument74 pagesHealth Systems 2009 20aug ANational Child Health Resource Centre (NCHRC)Pas encore d'évaluation
- ChisDocument34 pagesChisAnagha MaryPas encore d'évaluation
- Health Care USA Chapter 8Document76 pagesHealth Care USA Chapter 8David TurnerPas encore d'évaluation
- Healthcare SystemsDocument2 pagesHealthcare SystemsFlor IgartuaPas encore d'évaluation
- Running Head: HEALTH CARE MODELS 1Document6 pagesRunning Head: HEALTH CARE MODELS 1bavonenanePas encore d'évaluation
- Averting The Medicare Crisis: Health IRAs, Cato Policy AnalysisDocument8 pagesAverting The Medicare Crisis: Health IRAs, Cato Policy AnalysisCato InstitutePas encore d'évaluation
- Healthcare in IndiaDocument40 pagesHealthcare in Indiamanisha paikaray100% (1)
- Fixing India's Healthcare System - Carnegie Endowment For International PeaceDocument3 pagesFixing India's Healthcare System - Carnegie Endowment For International PeaceMohammad UzairPas encore d'évaluation
- Ealth Nsurance IN Ndia: R M - 05PH2010Document6 pagesEalth Nsurance IN Ndia: R M - 05PH2010api-26832469Pas encore d'évaluation
- LCGHC Mission StatementDocument1 pageLCGHC Mission StatementAlliance for DemocracyPas encore d'évaluation
- 3.2 Major Stake HoldersDocument51 pages3.2 Major Stake HoldersSwati SharmaPas encore d'évaluation
- HEALTH INSURANCE IN INDIA: NEED, PRESENT SCENARIO AND POTENTIALDocument6 pagesHEALTH INSURANCE IN INDIA: NEED, PRESENT SCENARIO AND POTENTIALsupriyaPas encore d'évaluation
- May06 100Document4 pagesMay06 100IATSEPas encore d'évaluation
- AllDocument48 pagesAllnanchiePas encore d'évaluation
- Philippine Health Insurance CorporationDocument7 pagesPhilippine Health Insurance CorporationEllen Glae DaquipilPas encore d'évaluation
- Hcentive Health Insurance Exchange PlatformDocument16 pagesHcentive Health Insurance Exchange PlatformalishanorthPas encore d'évaluation
- Health Insurance Explained: Benefits, Types, Issues & SolutionsDocument6 pagesHealth Insurance Explained: Benefits, Types, Issues & SolutionsMANIMEGALAIPas encore d'évaluation
- Health Practices of CanadaDocument17 pagesHealth Practices of CanadasnehaoctPas encore d'évaluation
- Placement Changes and Emergency Department Visits in The First Year of Foster CareDocument9 pagesPlacement Changes and Emergency Department Visits in The First Year of Foster CareJesse M. MassiePas encore d'évaluation
- Effective Discipline To Raise Healthy Children: Policy StatementDocument12 pagesEffective Discipline To Raise Healthy Children: Policy StatementJesse M. MassiePas encore d'évaluation
- Identifying Child Abuse Fatalities During Infancy: Clinical ReportDocument11 pagesIdentifying Child Abuse Fatalities During Infancy: Clinical ReportJesse M. MassiePas encore d'évaluation
- Oral and Dental Aspects of Child Abuse and Neglect: Clinical ReportDocument10 pagesOral and Dental Aspects of Child Abuse and Neglect: Clinical ReportJesse M. MassiePas encore d'évaluation
- Suidi Oklahoma ProviderDocument28 pagesSuidi Oklahoma ProviderJesse M. MassiePas encore d'évaluation
- Emergency Severity IndexDocument114 pagesEmergency Severity Indexpafin100% (3)
- Making The Most of Mentors: A Guide For MenteesDocument5 pagesMaking The Most of Mentors: A Guide For MenteesJesse M. MassiePas encore d'évaluation
- Ongoing Pediatric Health Care For The Child Who Has Been MaltreatedDocument18 pagesOngoing Pediatric Health Care For The Child Who Has Been MaltreatedJesse M. MassiePas encore d'évaluation
- Clinical Considerations Related To The Behavioral Manifestations of Child MaltreatmentDocument15 pagesClinical Considerations Related To The Behavioral Manifestations of Child MaltreatmentJesse M. MassiePas encore d'évaluation
- Difficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsDocument19 pagesDifficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsJesse M. MassiePas encore d'évaluation
- Jpeds Aom 208Document3 pagesJpeds Aom 208Jesse M. MassiePas encore d'évaluation
- Growth Chart IDocument1 pageGrowth Chart IJesse M. MassiePas encore d'évaluation
- IJMEDocument7 pagesIJMEJesse M. MassiePas encore d'évaluation
- i-PASS OBSERVATION TOOLDocument1 pagei-PASS OBSERVATION TOOLJesse M. MassiePas encore d'évaluation
- Persistent Fear and Anxiety Can Affect Young Childrens Learning and Development PDFDocument16 pagesPersistent Fear and Anxiety Can Affect Young Childrens Learning and Development PDFCristina AlexeevPas encore d'évaluation
- Ckeck List Operacional - Usda Inst Saude e SegDocument3 pagesCkeck List Operacional - Usda Inst Saude e SegQualidade CooperalfaPas encore d'évaluation
- Vroom Tips: Brain Building BasicsDocument16 pagesVroom Tips: Brain Building BasicsJesse M. MassiePas encore d'évaluation
- Status EpileticusDocument2 pagesStatus EpileticusJesse M. MassiePas encore d'évaluation
- dBA PROTECT YOUR HEARINGDocument4 pagesdBA PROTECT YOUR HEARINGJesse M. MassiePas encore d'évaluation
- SB773Document257 pagesSB773Jesse M. MassiePas encore d'évaluation
- What Is Child Abuse and Neglect? Recognizing The Signs and SymptomsDocument8 pagesWhat Is Child Abuse and Neglect? Recognizing The Signs and SymptomsJesse M. MassiePas encore d'évaluation
- Vroom Tips: Brain Building BasicsDocument7 pagesVroom Tips: Brain Building BasicsJesse M. MassiePas encore d'évaluation
- 2018 OdhhsDocument124 pages2018 OdhhsJesse M. MassiePas encore d'évaluation
- Cbig Cross-ReportingDocument25 pagesCbig Cross-ReportingJesse M. MassiePas encore d'évaluation
- COVID Positive/PUI: PAPR Prioritization MatrixDocument1 pageCOVID Positive/PUI: PAPR Prioritization MatrixJesse M. MassiePas encore d'évaluation
- Recommendations For Preventive Pediatric Health Care: Bright Futures/American Academy of PediatricsDocument2 pagesRecommendations For Preventive Pediatric Health Care: Bright Futures/American Academy of PediatricsJesse M. MassiePas encore d'évaluation
- Preventing Adverse Childhood Experiences (Aces) :: Leveraging The Best Available EvidenceDocument40 pagesPreventing Adverse Childhood Experiences (Aces) :: Leveraging The Best Available EvidenceJesse M. MassiePas encore d'évaluation
- Child Abuse Neglect Prevention OklahomaDocument44 pagesChild Abuse Neglect Prevention OklahomaJesse M. MassiePas encore d'évaluation
- Intimate Partner Violence, Sexual Violence, Stalking: Before The Age of 18Document1 pageIntimate Partner Violence, Sexual Violence, Stalking: Before The Age of 18Jesse M. MassiePas encore d'évaluation
- Domestic Violence Oklahoma 2017Document44 pagesDomestic Violence Oklahoma 2017Jesse M. MassiePas encore d'évaluation
- Resltado OBJ Preliminar Ensino Medio Completo Guarda Municipal de 2a ClasseDocument341 pagesResltado OBJ Preliminar Ensino Medio Completo Guarda Municipal de 2a Classefrancisca pachecoPas encore d'évaluation
- The Sanctuary Made Simple Lawrence NelsonDocument101 pagesThe Sanctuary Made Simple Lawrence NelsonSulphur92% (12)
- Hippo 3 Use 2020 V1.EDocument2 pagesHippo 3 Use 2020 V1.ECherry BushPas encore d'évaluation
- ELECTRONIC TICKET For 4N53LY Departure Date 27 06 2023Document3 pagesELECTRONIC TICKET For 4N53LY Departure Date 27 06 2023حسام رسميPas encore d'évaluation
- Big Bazaar Case Study 11.07.10Document18 pagesBig Bazaar Case Study 11.07.10Bhawna Gosain0% (1)
- Spider Man: No Way Home First Official Poster Is Out NowDocument3 pagesSpider Man: No Way Home First Official Poster Is Out NowzlatanblogPas encore d'évaluation
- Differences in Indian Culture and American Culture: Comparison EssayDocument2 pagesDifferences in Indian Culture and American Culture: Comparison EssayHan Huynh PhamPas encore d'évaluation
- Availability Dependencies EN XXDocument213 pagesAvailability Dependencies EN XXraobporaveenPas encore d'évaluation
- Understanding Plane and Solid FiguresDocument9 pagesUnderstanding Plane and Solid FiguresCoronia Mermaly Lamsen100% (2)
- 8 Edsa Shangri-La Hotel Vs BF CorpDocument21 pages8 Edsa Shangri-La Hotel Vs BF CorpKyla Ellen CalelaoPas encore d'évaluation
- Bangla Book "Gibat" P2Document34 pagesBangla Book "Gibat" P2Banda Calcecian100% (3)
- Abyip MagcagongDocument10 pagesAbyip MagcagongJhon TutorPas encore d'évaluation
- Liberal Arts Program: Myanmar Institute of TheologyDocument6 pagesLiberal Arts Program: Myanmar Institute of TheologyNang Bu LamaPas encore d'évaluation
- Display of Order of IC Constitution and Penal Consequences of Sexual HarassmentDocument1 pageDisplay of Order of IC Constitution and Penal Consequences of Sexual HarassmentDhananjayan GopinathanPas encore d'évaluation
- Clinical Risk Factor For Preterm BirthDocument22 pagesClinical Risk Factor For Preterm BirthGabyBffPas encore d'évaluation
- The Girl of Fire and Thorns Discussion GuideDocument1 pageThe Girl of Fire and Thorns Discussion GuidePitchDark100% (1)
- Resume With Leadership New 2Document2 pagesResume With Leadership New 2api-356808363Pas encore d'évaluation
- Charlotte Spencer - Student - SalemMS - Manifest Destiny and Sectionalism Unit PacketDocument9 pagesCharlotte Spencer - Student - SalemMS - Manifest Destiny and Sectionalism Unit Packetcharlotte spencerPas encore d'évaluation
- Determining Audience NeedsDocument5 pagesDetermining Audience NeedsOrago AjaaPas encore d'évaluation
- 2016 AP Micro FRQ - Consumer ChoiceDocument2 pages2016 AP Micro FRQ - Consumer ChoiceiuhdoiPas encore d'évaluation
- 1201086022Document8 pages1201086022robert_higgins6352Pas encore d'évaluation
- Networking and TESOL career goalsDocument2 pagesNetworking and TESOL career goalsSadiki FltaPas encore d'évaluation
- Benito Mussolini - English (Auto-Generated)Document35 pagesBenito Mussolini - English (Auto-Generated)FJ MacalePas encore d'évaluation
- 5658 1Document5 pages5658 1Afsheen ZaidiPas encore d'évaluation
- TestbankDocument11 pagesTestbankA. MagnoPas encore d'évaluation
- Product BrochureDocument18 pagesProduct Brochureopenid_Po9O0o44Pas encore d'évaluation
- RA 8293 Key Provisions on Compulsory Licensing and Patent RightsDocument30 pagesRA 8293 Key Provisions on Compulsory Licensing and Patent RightsPrincessPas encore d'évaluation
- 2023 Whole Bible Reading PlanDocument2 pages2023 Whole Bible Reading PlanDenmark BulanPas encore d'évaluation
- Teacher's PlannerDocument3 pagesTeacher's PlannerEmylie Alvarez LantoriaPas encore d'évaluation
- Case Study 2, Domino?s Sizzles With Pizza TrackerDocument3 pagesCase Study 2, Domino?s Sizzles With Pizza TrackerAman GoelPas encore d'évaluation