Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Breath Sounds - From Basic Science To Clinical Practice 2018Document314 pagesBreath Sounds - From Basic Science To Clinical Practice 2018programgrabber100% (2)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Dermatologic and Cosmetic Procedures in Office Practice, Expert Consult - Online and Print 1st EsDocument48 pagesDermatologic and Cosmetic Procedures in Office Practice, Expert Consult - Online and Print 1st Esprogramgrabber67% (3)
- ABG Tic Tac ToeDocument3 pagesABG Tic Tac ToeprogramgrabberPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Med Surg Study GuideDocument98 pagesMed Surg Study Guideprogramgrabber100% (2)
- Maternity Nursing Lecture NotesDocument198 pagesMaternity Nursing Lecture Notesprogramgrabber75% (4)
- Drug Calculations For Nurses A Step by Step ApproachDocument265 pagesDrug Calculations For Nurses A Step by Step ApproachPeter Moulatsiotis67% (9)
- DBT Goals of Skills TrainingDocument6 pagesDBT Goals of Skills TrainingDaniel Andres Racines JervesPas encore d'évaluation
- Dengue Fever Health TeachingDocument3 pagesDengue Fever Health TeachingDante Sales100% (3)
- Toefl PBT TestDocument34 pagesToefl PBT TestMonica Jazmin Olivera AguirrePas encore d'évaluation
- Disease Prevention Primary Secondary TertiaryDocument1 pageDisease Prevention Primary Secondary TertiaryprogramgrabberPas encore d'évaluation
- FJCFL, Vol XxboardofeditorsDocument1 pageFJCFL, Vol XxboardofeditorsprogramgrabberPas encore d'évaluation
- 7 IcpDocument9 pages7 IcpJah AcabPas encore d'évaluation
- Med Surg Study GuideDocument98 pagesMed Surg Study Guideprogramgrabber100% (23)
- Dukan Diet Food ListDocument2 pagesDukan Diet Food ListprogramgrabberPas encore d'évaluation
- Copd and PneuDocument38 pagesCopd and Pneuprogramgrabber100% (1)
- Anemia LectureDocument12 pagesAnemia LectureprogramgrabberPas encore d'évaluation
- HESI Pediatric HESI ReviewDocument41 pagesHESI Pediatric HESI Reviewprogramgrabber96% (24)
- Jail House Lawyers' Handbook - 2010 EditionDocument158 pagesJail House Lawyers' Handbook - 2010 EditionUmesh HeendeniyaPas encore d'évaluation
- Physical Assessment Exam Study GuidesDocument45 pagesPhysical Assessment Exam Study Guidesprogramgrabber100% (1)
- CDC Isolation 2007Document225 pagesCDC Isolation 2007programgrabberPas encore d'évaluation
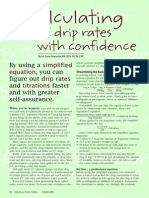
- IV Drip CalculationsDocument4 pagesIV Drip CalculationsmydewyboyPas encore d'évaluation
- 5a's 5R's AlgorithmDocument2 pages5a's 5R's Algorithmprogramgrabber100% (1)
- Arguments: THW Ban Miss UniverseDocument3 pagesArguments: THW Ban Miss UniverseGen eralPas encore d'évaluation
- The World's Expanding Waistline: Diet by Command?Document3 pagesThe World's Expanding Waistline: Diet by Command?KIET DO50% (2)
- Risk Management AwarenessDocument19 pagesRisk Management AwarenessRamalingam ChandrasekharanPas encore d'évaluation
- Kooner - Google SearchDocument2 pagesKooner - Google Searchmiir ikbalPas encore d'évaluation
- 2 Tissue Culture at Home ReportDocument7 pages2 Tissue Culture at Home ReportXwag 12Pas encore d'évaluation
- Self-Esteem Moderates The Associations Between Body-Related Self-Conscious Emotions and Depressive SymptomsDocument11 pagesSelf-Esteem Moderates The Associations Between Body-Related Self-Conscious Emotions and Depressive SymptomsAlliyah Roma CadaPas encore d'évaluation
- Draft LKPDDocument34 pagesDraft LKPDaliPas encore d'évaluation
- Lockout/Tagout (Loto) Checklist: 1. Scope of WorkDocument3 pagesLockout/Tagout (Loto) Checklist: 1. Scope of WorkPutri UnaPas encore d'évaluation
- Research Paper OutlineDocument3 pagesResearch Paper Outlineapi-317142831Pas encore d'évaluation
- 08 Permit To Work ProcedureDocument24 pages08 Permit To Work Procedureniteshsh31100% (1)
- Manual de Usuario Panasonic Toughbook CF-31 (44 Páginas)Document3 pagesManual de Usuario Panasonic Toughbook CF-31 (44 Páginas)Angel VelascoPas encore d'évaluation
- 015 Barium ChlorideDocument7 pages015 Barium Chlorideeng20072007Pas encore d'évaluation
- 3.1.1.3 CONTOH Pedoman Manual Mutu OKKKKDocument39 pages3.1.1.3 CONTOH Pedoman Manual Mutu OKKKKsapnah SKM100% (1)
- Daftar Pustaka EpilepsiDocument3 pagesDaftar Pustaka EpilepsiekaPas encore d'évaluation
- Let'S Dive Deeply!: Discussion Points: Read The Case Scenario and Relate It To The TheoryDocument1 pageLet'S Dive Deeply!: Discussion Points: Read The Case Scenario and Relate It To The TheoryAnn Mariz DominguezPas encore d'évaluation
- Garden Trust Launches A CompetitionDocument3 pagesGarden Trust Launches A CompetitionCami GrossiPas encore d'évaluation
- ETCO2 ReadingDocument19 pagesETCO2 ReadingTuan TrinhPas encore d'évaluation
- Indonesia Disaster ManagementDocument16 pagesIndonesia Disaster ManagementjaxassssPas encore d'évaluation
- 1 4Document2 pages1 4Chenna RosePas encore d'évaluation
- Government of Canada Report On Emend (Aprepitant)Document6 pagesGovernment of Canada Report On Emend (Aprepitant)jennabushPas encore d'évaluation
- MetricefDocument2 pagesMetricefPrakashNallappanPas encore d'évaluation
- Clientele and Audiences in Social Work SEMIS DIASSDocument30 pagesClientele and Audiences in Social Work SEMIS DIASSCharles CabarlesPas encore d'évaluation
- Aruna Ramchandra Shanbhug V Union of IndiaDocument4 pagesAruna Ramchandra Shanbhug V Union of IndiaTanya TandonPas encore d'évaluation
- Maharashtra DoctorsDocument55 pagesMaharashtra DoctorsVAIBHAV P ANPATPas encore d'évaluation
- Kaye CommDocument14 pagesKaye CommElaine AgustinPas encore d'évaluation
- Freiburg Flap ApplicatorDocument3 pagesFreiburg Flap Applicatorapi-299403846Pas encore d'évaluation
- Landmark Case: Indian Medical Association Vs V.P. ShanthaDocument4 pagesLandmark Case: Indian Medical Association Vs V.P. ShanthaRiken TandelPas encore d'évaluation