Vous aimerez peut-être aussi
- Newman FISA ResultsDocument6 pagesNewman FISA ResultsAnnaLuxePas encore d'évaluation
- SH Tournament InviteDocument2 pagesSH Tournament InviteAnnaLuxePas encore d'évaluation
- UVIC 2013 Speaker ScoresDocument6 pagesUVIC 2013 Speaker ScoresAnnaLuxePas encore d'évaluation
- Basic CNDF GuideDocument2 pagesBasic CNDF GuideAnnaLuxePas encore d'évaluation
- Dsabc Tabs Individual Results Junior DivisionDocument8 pagesDsabc Tabs Individual Results Junior DivisionAnnaLuxePas encore d'évaluation
- UVIC Invitational Jr. TeamDocument3 pagesUVIC Invitational Jr. TeamAnnaLuxePas encore d'évaluation
- Mock Trial OutlineDocument10 pagesMock Trial OutlineAnnaLuxePas encore d'évaluation
- AP Exam Past Exam PaperDocument3 pagesAP Exam Past Exam PaperAnnaLuxePas encore d'évaluation
- AP Exam Past Exam PaperDocument3 pagesAP Exam Past Exam PaperAnnaLuxePas encore d'évaluation
- AP Exam Past Exam PaperDocument3 pagesAP Exam Past Exam PaperAnnaLuxePas encore d'évaluation
- IB English Commentary InstructionsDocument4 pagesIB English Commentary InstructionsAnnaLuxePas encore d'évaluation
- AP Exam Past Exam PaperDocument312 pagesAP Exam Past Exam PaperAnnaLuxe100% (3)
- AP Comparative Government FRQsDocument5 pagesAP Comparative Government FRQsAnnaLuxePas encore d'évaluation
- AP Comparative Government and Politics 2011 Free-Response QuestionsDocument3 pagesAP Comparative Government and Politics 2011 Free-Response QuestionsAnnaLuxePas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Neighborhood InvestigationDocument4 pagesNeighborhood Investigationapi-302394994Pas encore d'évaluation
- "Truth, Excellence, Service": Historical Review, 114 (2), 279-306Document5 pages"Truth, Excellence, Service": Historical Review, 114 (2), 279-306Chen Adrien Z. ThorPas encore d'évaluation
- 1Document54 pages1Maria Francessa AbatPas encore d'évaluation
- Appl TranscriptsDocument3 pagesAppl Transcriptssriram_parthaPas encore d'évaluation
- Method and Media Health EducationDocument10 pagesMethod and Media Health EducationAshok Mishra100% (2)
- Outline of Rizal's Life 2Document73 pagesOutline of Rizal's Life 2Reyji Edduba100% (1)
- BSC Comp SC - CBCSS Syllabus PDFDocument42 pagesBSC Comp SC - CBCSS Syllabus PDFSooraj krishnan v.sPas encore d'évaluation
- National Policy On Education (NPE 1986)Document11 pagesNational Policy On Education (NPE 1986)deepak kumarPas encore d'évaluation
- Edf1304 Assignment 1 Part 1 - Emily Greenberg - 26005123 1Document5 pagesEdf1304 Assignment 1 Part 1 - Emily Greenberg - 26005123 1api-285104874Pas encore d'évaluation
- Activity 1Document4 pagesActivity 1Joy Kimberly PaglinawanPas encore d'évaluation
- Predictors of Board Exam Performance of The Dhvtsu College of Education GraduatesDocument4 pagesPredictors of Board Exam Performance of The Dhvtsu College of Education Graduates15-0001Pas encore d'évaluation
- What Is Reflection and Reflective WritingDocument3 pagesWhat Is Reflection and Reflective WritingR-wah LarounettePas encore d'évaluation
- Betty Final Draft Assignment 2 - 04Document13 pagesBetty Final Draft Assignment 2 - 04Sei ChanPas encore d'évaluation
- Internship ReportDocument17 pagesInternship ReportDavidChenPas encore d'évaluation
- Neelima K VDocument3 pagesNeelima K Vneelima kommiPas encore d'évaluation
- 04 Expressing Satisfaction & Dissatisfaction - ExerciseDocument2 pages04 Expressing Satisfaction & Dissatisfaction - ExerciseMarcello AntonyPas encore d'évaluation
- Upside Down Art - MichelangeloDocument3 pagesUpside Down Art - Michelangeloapi-374986286100% (1)
- Strategic Negotiation and Deal MakingDocument7 pagesStrategic Negotiation and Deal MakingRohanPas encore d'évaluation
- CBM IndexDocument8 pagesCBM IndexSaili SarmalkarPas encore d'évaluation
- Australian Universities 2013Document25 pagesAustralian Universities 2013L Liew Tuck OnnPas encore d'évaluation
- Supervisory Plan: School ID: 501222 Poonbato IS 09455370326 501222pis@deped - Gov.phDocument2 pagesSupervisory Plan: School ID: 501222 Poonbato IS 09455370326 501222pis@deped - Gov.phBryan JesterPas encore d'évaluation
- Nursing Theory-Patient-Centered Approaches To Nurses.Document10 pagesNursing Theory-Patient-Centered Approaches To Nurses.Bheru LalPas encore d'évaluation
- SED 1FIL-10 Panimulang Linggwistika (FIL 102)Document10 pagesSED 1FIL-10 Panimulang Linggwistika (FIL 102)BUEN, WENCESLAO, JR. JASMINPas encore d'évaluation
- North East Frontier Railway Recruitment 2013 Group D Posts 1230 VacancyDocument3 pagesNorth East Frontier Railway Recruitment 2013 Group D Posts 1230 VacancymalaarunPas encore d'évaluation
- Appendix I Faculty Evaluation System General InformationDocument11 pagesAppendix I Faculty Evaluation System General InformationDani PhilipPas encore d'évaluation
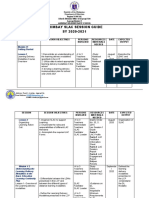
- Arimbay Slac Session Guide SY 2020-2021Document6 pagesArimbay Slac Session Guide SY 2020-2021Jen ApinadoPas encore d'évaluation
- FS2 Le18Document1 pageFS2 Le18Jorebell W. QuiminoPas encore d'évaluation
- Handbook of Social MedicineDocument577 pagesHandbook of Social MedicineTaufiq AsrulPas encore d'évaluation
- James Cameron: Early LifeDocument7 pagesJames Cameron: Early Lifeproacad writersPas encore d'évaluation
- UT Dallas Syllabus For Stat1342.501.11s Taught by Yuly Koshevnik (Yxk055000)Document7 pagesUT Dallas Syllabus For Stat1342.501.11s Taught by Yuly Koshevnik (Yxk055000)UT Dallas Provost's Technology GroupPas encore d'évaluation