Vous aimerez peut-être aussi
- Lesson 3 Módulo de Inglés Auxiliares Orales U de C (Blog)Document67 pagesLesson 3 Módulo de Inglés Auxiliares Orales U de C (Blog)Martha Leon FigueroaPas encore d'évaluation
- Cluster Randomized Trials PDFDocument47 pagesCluster Randomized Trials PDFMartha Leon FigueroaPas encore d'évaluation
- Lesson 1 Módulo de Inglés Auxiliares Orales U de C (Blog)Document56 pagesLesson 1 Módulo de Inglés Auxiliares Orales U de C (Blog)Martha Leon FigueroaPas encore d'évaluation
- Metodology of Non Inferiority PDFDocument8 pagesMetodology of Non Inferiority PDFMartha Leon FigueroaPas encore d'évaluation
- Cluster Randomized Trials PDFDocument47 pagesCluster Randomized Trials PDFMartha Leon FigueroaPas encore d'évaluation
- SJ BDJ 2011 764 PDFDocument4 pagesSJ BDJ 2011 764 PDFalfredoibcPas encore d'évaluation
- Statistical Methods in Clinical Trials PDFDocument3 pagesStatistical Methods in Clinical Trials PDFMartha Leon FigueroaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hydrochloric Acid MSDS: 1. Product and Company IdentificationDocument7 pagesHydrochloric Acid MSDS: 1. Product and Company IdentificationdeaPas encore d'évaluation
- Reward Response in The BrainDocument18 pagesReward Response in The Brainapi-566508933Pas encore d'évaluation
- Health Leaflet for Cataract PatientsDocument31 pagesHealth Leaflet for Cataract PatientsLorelie AsisPas encore d'évaluation
- Barangay Disaster Risk Reduction Management PlanDocument25 pagesBarangay Disaster Risk Reduction Management PlanGain Gain100% (1)
- 15 Annotated Bibliography (Final)Document8 pages15 Annotated Bibliography (Final)ethanPas encore d'évaluation
- DrugsDocument2 pagesDrugsJan PatrickPas encore d'évaluation
- Cbydp & AbyipDocument17 pagesCbydp & AbyipJanine PigaoPas encore d'évaluation
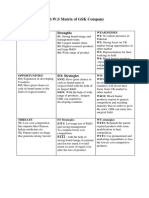
- Tows GSKDocument2 pagesTows GSKQanita Shah100% (2)
- An Appraisal On Complex Relationship Between From Ayurveda: Vyayama (Physical Activity) and Health: InsightsDocument12 pagesAn Appraisal On Complex Relationship Between From Ayurveda: Vyayama (Physical Activity) and Health: InsightsVivian FernandesPas encore d'évaluation
- Lisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationDocument6 pagesLisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationCliff by the seaPas encore d'évaluation
- Chemical Composition of Sewage Sludges in IowaDocument13 pagesChemical Composition of Sewage Sludges in IowaPalash YadavPas encore d'évaluation
- Health Education On Elderly PDFDocument25 pagesHealth Education On Elderly PDFReyta NoorPas encore d'évaluation
- Sample Letter Medical NecessityDocument2 pagesSample Letter Medical NecessityMin SoePas encore d'évaluation
- CollaProfiles - 21CL08Document8 pagesCollaProfiles - 21CL08Deolinda FerreiraPas encore d'évaluation
- Art Therapy and Neuroscience (Article)Document25 pagesArt Therapy and Neuroscience (Article)rosalindkitty100% (1)
- Vinayaka Missions University: Vinayaka Mission's Kirupananda Variyar Engineering CollegeDocument4 pagesVinayaka Missions University: Vinayaka Mission's Kirupananda Variyar Engineering CollegeNoor AhmedPas encore d'évaluation
- MSDS An180Document2 pagesMSDS An180Mohamed ArafatPas encore d'évaluation
- CH 2 IntroductionDocument4 pagesCH 2 IntroductionSyafiq D ZulPas encore d'évaluation
- Research About Comparative and Superlative AdjectivesDocument3 pagesResearch About Comparative and Superlative AdjectivesMaryurys SalasPas encore d'évaluation
- The Journal of Prosthetic Dentistry Volume 62 Issue 2 1989 (Doi 10.1016 - 0022-3913 (89) 90323-5) Arthur M. LaVere - Anterior Retention For Removable Partial DenturesDocument1 pageThe Journal of Prosthetic Dentistry Volume 62 Issue 2 1989 (Doi 10.1016 - 0022-3913 (89) 90323-5) Arthur M. LaVere - Anterior Retention For Removable Partial DenturesWin BramahagaPas encore d'évaluation
- SORIANO, Angelica Joan M. - NURSING CARE PLAN Activity 2. NCM 114Document5 pagesSORIANO, Angelica Joan M. - NURSING CARE PLAN Activity 2. NCM 114Angelica Joan SorianoPas encore d'évaluation
- Zumbro Shopper: Gorman'sDocument14 pagesZumbro Shopper: Gorman'sKristina HicksPas encore d'évaluation
- 55122505241#5852#55122505241#9 - 16 - 2022 12 - 00 - 00 AmDocument2 pages55122505241#5852#55122505241#9 - 16 - 2022 12 - 00 - 00 AmAdham ZidanPas encore d'évaluation
- Accessibility To Potable Water Supply and Satisfaction of Urban Residents in Lokoja, NigeriaDocument20 pagesAccessibility To Potable Water Supply and Satisfaction of Urban Residents in Lokoja, NigeriaGovernance and Society ReviewPas encore d'évaluation
- Hernia World Conference ProgramDocument112 pagesHernia World Conference ProgramYovan Prakosa100% (1)
- Campbells Kids Club 2016 2017 Welcome LetterDocument2 pagesCampbells Kids Club 2016 2017 Welcome Letterapi-314708963Pas encore d'évaluation
- The Case of George EthicsDocument4 pagesThe Case of George EthicsPau De GuzmanPas encore d'évaluation
- Date/Time Patient PT Status Age Sex DOB LocationDocument56 pagesDate/Time Patient PT Status Age Sex DOB Locationzeerak khanPas encore d'évaluation
- Green Playful Welcome Back To School NewsletterDocument16 pagesGreen Playful Welcome Back To School NewsletterJocelyn RoxasPas encore d'évaluation
- Frontal LobeDocument14 pagesFrontal Lobebilal100% (2)