Académique Documents
Professionnel Documents
Culture Documents
Assessment of Procurement System & Capacity of Health Department, Khyber Pakhtunkhwa
Transféré par
Ali Raza Hanjra0 évaluation0% ont trouvé ce document utile (0 vote)
217 vues175 pagesGovernment Procurement System Assessment on OECD-DAC Model
Copyright
© © All Rights Reserved
Formats disponibles
PDF, TXT ou lisez en ligne sur Scribd
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentGovernment Procurement System Assessment on OECD-DAC Model
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
0 évaluation0% ont trouvé ce document utile (0 vote)
217 vues175 pagesAssessment of Procurement System & Capacity of Health Department, Khyber Pakhtunkhwa
Transféré par
Ali Raza HanjraGovernment Procurement System Assessment on OECD-DAC Model
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
Vous êtes sur la page 1sur 175
TRF is funded by UKaid from the Department for International Development and AusAID, and managed by HLSP
Assessment of the Procurement System and
Capacity of the Health Department
December 2012
Khyber Pakhtunkhwa
"
Table of Contents
1 Acknowledgements................................................................................................
iii
2 Abbreviations & Keywords....................................................................................
v
3 Executive Summary................................................................................................ 1
3.1 Strengths & Weaknesses of the Procurement System of DoH Khyber
Pakhtunkhwa....
1
4 Background 5
4.1 Technical Assistance.. 5
4.2 Terms of Reference (TORs).............. 6
4.3 Organizational Structure of Health Department, Khyber Pakhtunkhwa..
6
4.4 Procurement Entities of Health Department Khyber Pakhtunkhwa. 8
4.5 Procurement Practices in Health Department, Khyber Pakhtunkhwa
9
5 Section-1: Situational Analysis & Assessment of Existing Procurement
Procedures and Procuring Entities of Health Department Khyber
Pakhtunkhwa 12
5.1 Assessment Methodology.............................................................................. 12
5.2 Introduction of Factors Assessed under the Methodology............................. 13
5.3 Sampling Statistics......................................................................................... 13
5.4 Limitations & Constraints................................................................................
14
5.5 Summary of the Assessment Scores....
14
5.6 Pillar-I: Legislative and Regulatory Framework.....................................
19
Indicator-1: Public procurement legislative and regulatory
framework complies with applicable obligations with
regard to national and international
requirements................................ 19
Indicator-2: Existence of implementing regulations and
documentation. 43
5.7 Pillar-II: Institutional Framework & Management Capacity 49
Indicator-3: The public procurement system is mainstreamed
and well integrated into the public sector
governance system.................................................. 49
Indicator-4: The province has a functional normative and/or
regulatory body...
56
Indicator-5: Existence of institutional development capacity....... 56
5.8 Pillar III: Procurement Operations and Market Practices... 60
Indicator 6.
The provincial procurement operations and
practices are efficient 60
Indicator-7: Functionality of the public procurement market 65
Indicator-8: Existence of contract administration and
dispute resolution provisions 70
5.9 Pillar IV: Integrity and Transparency of the Public Procurement
System........................................................................................................... 76
Indicator-9: The province has effective control and audit
systems. 76
Indicator-10: Efficiency of appeals mechanism 80
Indicator-11: Degree of access to information.. 84
Indicator-12: The province has ethics and anticorruption
measures in place.............
85
!!
6
Section-II: Supply Chain Management of Pharmaceuticals in the Health
Department..
91
7 Section-III: Assessment of Identified Risks & Their Mitigation
Strategies............ 95
8 Section-IV: Spend Analysis of Health Sector Procurements............................ 109
9 Section V- Recommendations on Institutional Measures 112
9.1 Health Sector Procurement Manual................................................................
112
9.2 Strengthening of the Existing Procurement Cell at DGHS KP........................ 113
9.3 Utilization of a dedicated web-portal for the Health
Department..................................................................................................... 114
9.4 Human Resource Management...................................................................... 115
9.5 Inventory & Warehousing Management.......................................................... 116
9.6 Proposed Mission of Procurement Cell........................................................... 116
9.7 Proposed Administrative Structure of Procurement Cell, DGHS, KP............. 117
9.8 Individual Job Responsibilities & Qualifications of the Procurement Officials
for Procurement Cell& TORs.........................................................................
129
10 Annexures
10.1 List of Persons interviewed............................................................................ 158
10.2 Training Calendar for Health Department Khyber Pakhtunkhwa................... 161
10.3 Questionnaires used for Review Processes 163
List of Figures:
Figure: 5.9
Graphical Presentation of Strengths & Weaknesses of the
DoH Procurement System....................................................
3
Figure: 9.7.1 Organizational Organogram of Procurement Cell, DGHS
KP.......................................................................................... 118
Figure: 9.7.2 Functions of Wings in the Procurement Cell, DGHS, KP......
119
Figure: 9.7.3 Hierarchy of Pre/Post-Qualification Wing........................... 120
Figure-9.7.4: Hierarchy of Technical Wing 122
Figure-9.7.5: Tendering & Coordination Wing.
125
Figure-9.7.6: The hierarchy of the Budget & Planning Wing
128
Figure-9.8.1: Nature & Requirement of Individual Job Function.... 129
Tables:
Table 8.1: Comparison of Current Budget spending with Development
Budget for the Years 2009-12............................. 109
Table 8.2: Budgets allocated for the Purchase of Drugs & Bio-Medical
Equipment for the Years 2009-12 for all District
Governments and the Provincial Government 110
Table 8.3: Provincial vs District Budget Estimates & Actual
Expenditure for the Year 2012-13 ... 111
"""
1. Acknowledgement
This report has been prepared by Muhammad Ali Raza, Procurement Consultant, Technical
Resource Facility (TRF), Khyber Pakhtunkhwa. The Consultant is grateful to Mr. Farooq Azam,
Team Leader TRF Islamabad and Mr. Khalid Mahmood, Procurement Specialist TRF
Islamabad without whose continuous support, facilitation and morale boosting, formulation of
this Report couldnt have been possible. For facilitation and coordination at Khyber
Pakhtunkhwa, the Consultant is grateful to Dr. Muhammad Rahman Khattak, Provincial
Coordinator TRF KP and Syed Sharf ul Haq Trimizi, Project officer TRF KP.
The Consultant is grateful for support of Mr. Ashfaq Ahmad Khan, Secretary Health Khyber
Pakhtunkhwa, Mr. Zahir Alam, former Additional Secretary DoH Khyber Pakhtunkhwa and Mr.
Sher Gul Safi, Chief Planning Officer DoH Khyber Pakhtunkhwa whose valuable input made
this Report possible. The Consultant is grateful for support of Mr. Nadeem Bashir, Additional
Secretary Finance, Department of Finance, Khyber Pakhtunkhwa.
The Consultant is also grateful to Mr. Sharif Ahmad Khan, Director General Health Services,
Department of Health, Khyber Pakhtunkhwa, whose close collaboration and support helped
him in finalizing the said Report.
The Consultant is also much grateful to Dr. Shabina Raza, Chief Coordinator Health Sector
Reforms Unit (HSRU), DoH, Khyber Pakhtunkhwa, for giving her support and assistance in
understanding the new policy framework for the reform initiatives for DoH Khyber
Pakhtunkhwa. The Consultant wishes to thank Mr. Ali Zahir Shah, Deputy Secretary Health
Department Health Department Khyber Pakhtunkhwa for their support in collecting information
on working of Health Secretariat.
The Consultant would also like to thank Govt-Medicine Coordination Cell (Govt-MCC), DoH
Khyber Pakhtunkhwa for coordinating, as Specialized Section for Drugs and Medicines, in
designing, revising and evaluating the Standard Bidding Documents (SBDs) for procurement
of Drugs & Surgical Disposables for DoH Khyber Pakhtunkhwa and assisting in providing a
better insight through discourse on comparative analysis of previous and current procurement
practices prevalent at Govt-MCC Section, DGHS, Khyber Pakhtunkhwa.
Disclaimer
This document is issued for the party which commissioned it and for specific purposes
connected with the above-captioned project only. It should not be relied upon by any other
party or used for any other purpose.
No responsibility is accepted for the consequences of this document being relied upon by any
other party, or being used for any other purpose, or containing any error or omission which is
due to an error or omission in data supplied by other parties.
!"
"
2. Abbreviations& Key words
AMI Autonomous Medical Institution
AAMI Association for the Advancement of Medical Instrumentation
API Active Pharmaceutical Ingredient
BHU Basic Health Unit
BOQs Bill of Quantities
BLIs Base Line Indicators
CBET Certified Bio-Medical Equipment Technician
CCE Certified Clinical Engineer
CE Communaut Europenne (Council of Europe)
CE Chief Executive (Autonomous Medical Institution)
CFAA Country Financial Accountability Assessment
cGMP Current Good Manufacturing Practices (for Pharmaceutical Industry)
CIPS Chartered Institute of Purchasing & Supply (UK)
CLES Certified Laboratory Equipment Specialist
CMW Community Midwife
CPCM Certified Professional Contract Manager (USA)
CPO Chief Planning Officer, Health Secretariat
CPPO Certified Public Purchasing Officer (USA)
CRES Certified Radiology Equipment Technician
CS Comparative Statement
DAC Departmental Accounts Committee
DDWP Departmental Development Working Party
DFID Department for International Development (UKAID)
DGHS Directorate General Health Services / Director General Health Services
DHO District Health Officer
DHQ District Head Quarter Hospital
DHS District Health Services/District Health Govt./Dept.
DI Drug Inspector
DoH Department of Health, Govt. of Khyber Pakhtunkhwa
DRA Drug Regulatory Authority
DTL Drug Testing Laboratory, Peshawar
ECRI
Emergency Care Research Institute, USA (Bio-Medical Equipment Database)
EDL Essential Drug List
EEC European Economic Community
EMA European Medicines Agency
EPI Expanded Immunization Program
ERP Enterprise Resource Planning (Automation Software)
ERP Emergency Relief Package
ETR End of Treatment Response
EU European Union
!"
EVR Early Virologic Response
ETR End of Treatment Response
FABS Financial Accounting & Budgeting System
FCPA Foreign Corrupt Practices Act
FDA Federal Drug Agency (United States)
FI Financial (SAP)
FIDIC Fdration Internationale Des Injuneurs Conseils (International Federation of
Consulting Engineers), Geneva
FPP Finished Pharmaceutical Products
FPPRA Federal Public Procurement Regulatory Authority
KP Khyber Pakhtunkhwa (Province)
GFR General Financial Rules (AGPR)
GMP Good Manufacturing Practices (for Pharmaceutical Industry)
Govt. Govt. Of the Khyber Pakhtunkhwa
Govt-MCC Government-Medicine Coordination Cell, DGHS
HIV Human Immunodeficiency Virus
HMC Hayatabad Medical Complex, Peshawar
IACCM International Association of Commercial & Contract Management (EU/UK)
ICGFM International Consortium on Governmental Financial Management
IFB Invitation For Bids
IMS Health Intercontinental Medical Statistics for Health (Pharmaceutical Database)
INN International Non-Proprietary Name
INOR !"#$%$&$' )* +&,-'./ 0",)-)12 3 4.5%)-)126 788)$$.8.5
IRNUM Institute of Radiology & Nuclear Medicines, Peshawar
KP Khyber Pakhtunkhwa
KTH Khyber Teaching Hospital, Peshawar
LHW Lady Health Worker (Program)
LMIS Logistics Management Information System
LRH Leady Reading Hospital, Peshawar
MM Materials Management (SAP)
MNCH Mother Neo-natal Child Health (Program)
MoH Ministry of Health (Federal Government)
MS Medical Superintendent (Administrative in charge of DHQ Hospitals)
MSD Medical Store Depot, Health Department
NFC National Finance Commission
NHS National Health Service, UK
NIT National Institute of Training, PPRA, Islamabad
NWFP North West Frontier Province
OECD-DAC Organization for Economic Cooperation & Development- Development
Assistance Committee
PACP Provincial Aids Control Program
PC Project Coordinator (Vertical Programs)
PDWP Provincial Development Working Party
"##
PE Procuring Entity
PEFA Public Expenditure & Financial Accountability
PFM Public Financial Management
PHSA Provincial Health Services Academy, Peshawar
PIFRA Project to Improve Financial Reporting & Auditing
PNAC Pakistan National Accreditatation Council
PPRA Public Procurement Regulatory Authority
PPRs Public Procurement Rules
PV Product Vocabulary
PWD Population Welfare Department
RHC Rural Health Center
RVR Rapid Virologic Response
SAP Systems Applications and Products in Data Processing
SBDs Standard Bidding Documents
SID4Health Supplier Information Database for Health, UK
SOPs Standard Operating Procedures
SVR Sustained Virologic Response
TA Technical Assistance
T&E Technical & Evaluation (Committee)
TRF Technical Resource Facility
THQ Tehsil Head Quarter Hospital
WHO World Health Organization.
!
1
3. Executive Summary
Contextual Challenges to the Health Sector
Khyber Pakhtunkhwa is currently having the NWFP Procurement of Goods, Works and Services
Rules 2003 in vogue which seem outdated in the context of the Federal Public Procurement Rules
2004 and the Provincial Procurement Rules of Sind & Punjab. Still the Health Department Khyber
Pakhtunkhwa has been engaged in the procurement of bio-medical equipment and pharmaceutical
products to the tune of Rs. 125 billion approximately for the year 2012-13 under the said Provincial
Rules.
In the wake of devolution of procurement functions by the 18
th
Constitutional Amendment the
procurement officials of the Health Department Khyber Pakhtunkhwa are very well aware of the
professional capacity needs to tackle such a voluminous purchasing challenge. In order to get
thoroughly acquainted to needs, technical possibilities and market conditions for conducting this
sensitive public sector operation, the Health Department Khyber Pakhtunkhwa requested the
Technical Resource Facility (TRF) to initiate a Technical Assistance to strengthen its existing
procurement systems and increase the professional capacity of its procurement officials to meet the
challenges of achieving best value for money in a fair and transparent manner. The Procurement
System Assessment conducted by the TRF is therefore a way forward to indicate the distortions in
the current procurement business processes and suggest mitigating strategies to improve the same.
Review of Existing Procurement Scenarios:
In the Review Section, the Assessment Report under reference gives the background of Technical
Assistance & a brief introduction of the TORs and the post-18
th
Amendment devolution scenario in
which the current procurement practices are being followed by the procuring institutions of the
Health Department Khyber Pakhtunkhwa. Though the current District Government system has been
abolished by Provincial Government vide notification No. SO(E-I)/E&AD/4-49/2012, dated
28.12.2012, it may not have any immediate significant change in the procurement practices
prevalent in the Health Department except for an anticipated outlay of funds at the disposal of the
Health Department for better annual procurement planning and the increased role of the Principal
Accounting Officer. However, the same is subject to any future review. The Review Section under
reference further elaborates the assessment methodology consisting of OECDs Base Line
Indicators (BLIs) which have the capacity to be used in assessing the national, sub-national and
agency procurement systems with equal efficiency and meticulous detail. The BLIs are based on
four pillars relating to Legislative and Regulatory Framework, Institutional Framework &
Management Capacity, Procurement Operations and Market Practices and lastly, Integrity and
Transparency of a Public Procurement System.
3.1 Strengths & Weaknesses of the Procurement System of DoH Khyber Pakhtunkhwa:
The four pillars contain various base line indicators which individually assess the strengths and
weaknesses of the Procurement System of Health Department Khyber Pakhtunkhwa in terms of
numerical scoring allocated to various parameters. Whereas the fourth BLI relating to a public
procurement regulatory authority in the domain of Institutional Framework & Management Capacity
2
could not be assessed due to absence of any such body uptil now despite its notification by the
Provincial Assembly vide Khyber Pakhtunkhwa Public Procurement Regulatory Authority Act 2012
dated 20.09.2012, the other BLIs were thoroughly assessed and scored against their benchmarks.
The graphical outcome of the strengths and weaknesses at page 14 of the Report displays the
state of affairs of the current procurement system of the Health Department Khyber Pakhtunkhwa.
Whereas the perfect square along the two axes shows an ideal compliance to all the Base Line
Indicators, the resulting geometric quadrilateral within the perfect square along the same axes gives
a snapshot of the extent of deviations or shortcomings of the existing procurement business
practices in the Department at the Provincial level. The resulting quadrilateral shows a stronger side
of the BLIs for the First Pillar relating to Legislative and Regulatory Framework which scored well in
the context of achieving performance benchmarks largely attributed to a strong and robust
regulatory mechanisms for pre-qualification of pharmaceutical firms/bio-medical suppliers existing in
the Health Department Khyber Pakhtunkhwa and pre-notified/ well-structured Departmental
committees for bid evaluation.
The assessment of the Second Pillar relating to Institutional Framework & Management Capacity
displayed that the Province is weakest in institutional framework due to absence of a public
procurement regulatory body and lack of enforcement in developing systems and procedures for
collecting and monitoring provincial procurement statistics. Though the planning side of the
budgetary process in the Department strives to give a well-coordinated picture of development
funds appropriations against procurement initiatives, absence of detailed procurement plans based
on contract actions and lack of initiatives of the Health Department towards imparting professional
trainings in the public procurement regulations to its employees engaged in purchasing function,
has weekend this Pillar.
The assessment of the Third Pillar relating to Procurement Operations and Market Practices gave
an average impact due to absence of any planning towards matching skills with the procurement
assignments, but with somewhat sturdier private sector partnership with the Health Department due
to increase in the demand of pharmaceutical products with the passage of time, and prevailing
traditional but tested contract management processes.
The assessment of the Fourth Pillar relating to Integrity and Transparency of the Public
Procurement System, gives an above average profile of performance for the procurement system
due to a strong vigilance and drug quality control enforcement by the Department. However,
absence of internal audit and a weak appeals mechanism did not let it gain any significant score in
this area.
3
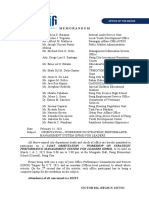
Pillar-I
Legislative Framework
3.0
2.07
Pillar-IV 3.0 0 3.0 Pillar-II
Integrity & Transparency 2.0 0.91 Institutional &
Management Capacity
1.6
Province Score
Maximum Score
3.0
Pillar-III
Procurement Operations & Markets
5.9 : Graphical Presentation of Strengths & Weaknesses of DoH Procurement System
In this graphic representation, scoring under each Pillar has been aggregated as a simple
arithmetical average of sub-indicators under the Pillar. The average scores for each Pillar are
compared to the maximum score of 3. The Province assessed is strongest in Pillar I, but has
weaknesses in the other three Pillars, with Pillar-II being the weakest.
The Assessment Report elaborates the major risks belonging to various regulatory, institutional,
process and operational aspects of the procurement life cycle in the Health Department identified
during the situational analysis. The said risks have been assessed in terms of their relative
importance, their strengths and probability of occurrence, and their mitigating strategies duly
chalked out to preserve the efficiency of the system.
In the end, certain institutional measures have been suggested for their likely consequences for
improving the efficiency of the system, e.g., a health sector procurement supplement in the form of
a Procurement Manual to be read in conjunction with the prevailing purchasing regulations,
developing a dedicated Human Resource Management for the procurement life cycle,
strengthening of the existing Procurement Cell at Directorate General Health Services and its
functional attributes alongwith probable staffing details, creation of a dedicated web-portal for
4
Contract Lifecycle Management, and recommendations on improving pharmaceutical warehousing
and inventory management operations and future strategies on procurement spend-trends of the
Department.
Lastly, a Procurement & Contract Management Training calendar for the next six months (January-
June 2013) for Khyber Pakhtunkhwa Health Department procurement professionals has been
appended to render training to meet their specific capacity building and mentoring needs.
5
4. Background
4.1: Technical Assistance
The Province of Khyber Pakhtunkhwa has assumed a daunting role in meeting the challenges due
to the enactment of 18
th
Amendment by National Assembly the form of devolution of social sectors
including health to provinces through abolition of concurrent legislative list. As per the
implementation plan, the Federal Ministry of Health has therefore been abolished with effect from
July 1, 2011 and except for Drug Licensing, Registration & Pricing functions, export/import of goods
and services to be retained as Federal functions and keeping professional councils such as
Pakistan Medical & Dental Council, Nursing Council and Pharmacy Council as Federal entities, the
initiatives like drafting and enactment of health and procurement regulations, management of
Vertical Programs and initiation of Health Sector reforms, have become provincial subjects. The
fiscal resources for the said initiatives have also been diverted or, are being diverted to the
Provinces with more administrative control.
In the wake of the said development, the Health Department Khyber Pakhtunkhwa has to shoulder
now a far greater responsibility of providing an affordable health care system which is easily
accessible to the common man elsewhere in the Province. Administrative and fiscal space of the
Provinces has increased multi-fold with a simultaneously increase in their responsibilities. In order
to provide equitable, affordable and accessible health care to the people, Provincial Governments
need to re-align and re-adjust their health care delivery systems, governance structures and
financial allocations.
The Government of Khyber Pakhtunkhwa therefore requires adoption of a renewed business
process in procurement of Health Sector Goods to achieve an acquisition lifecycle which addresses
all the complex needs of the Health Sector purchasing while keeping intact the requisites of
integrity, transparency, fair play in the process and providing equitable opportunity through open
competition for the Health industry. The Procurement System Assessment, initiated through the
Technical Assistance of TRF therefore strives to support the Khyber Pakhtunkhwa Health
Department to establish priorities for achieving best value for money in the purchasing perspective.
The analysis further identifies the areas wherein the Health Department may align its energies to
improve its procurement practices in view of Khyber Pakhtunkhwa Health Sector Strategy. The
enactment of Khyber Pakhtunkhwa Public Procurement Regulatory Authority Ordinance 2012 by the
Provincial Assembly has paved the way for the administrative notification of Khyber Pakhtunkhwa
Public Procurement Rules 2012 by the Provincial Government in due course of time and has also
made this assessment exercise worthwhile in the wake of adoption of international best practices in
procurement by the Health Department to replace the outdated NWFP Procurement of Goods,
Works & Services Rules 2003. The Health Department therefore needs to be geared up in advance
by standardizing its procurement practices and bidding documents and prioritizing necessary
capacity building initiatives for its procurement officials in the light of international best practices in
public contracting.
6
4.2: Terms of Reference (TORs)
Main Objective
The main objective of this assignment is to provide support to the Health Department,
Government of Khyber Pakhtunkhwa and Health Programmes in all issues related to
procurement and to build institutional capacity in procurement management.
Specific Objectives
Specifically the consultant will focus on:
i. identification of weaknesses and gaps in the procurement system and relevant supply
chain issues of Health Department and health programmes of Khyber Pakhtunkhwa
through a detailed assessment;
ii. development of action plan and strategy for implementation;
iii. proper implementation of rules framed by the Government of Khyber Pakhtunkhwa for
ongoing procurement of goods, works and services and consultancy services within the
Health Department and health programmes; with the prime purpose of effective,
efficient and transparent procurement system and processes;
iv. development and adaptation of procurement documents; with proper redressal of
complaints mechanism;
v. building capacity of procurement staff in procurement of goods, works and consultancy
services including recommendations for appropriate institutional structures and
mechanisms;
vi. provide on-the-job support to the procurement staff in all steps of procurement cycle;
vii. implementation of procurement monitoring mechanism and tools, within the DOH and
health programmes; and
viii. Coordination in implementation of procurement related Technical Assistance.
4.3: Organizational Structure of Health Department, Khyber Pakhtunkhwa
The Health Department has the following organizational structure in terms of Procurements:
a. Health Secretariat, Peshawar:
All procurement related polices are developed and their administrative approval conducted by
the Health Secretariat. However, Secretary Health has little to do with procurements except for
acting as an approving body for the contract award recommendations being chairman
Selection (Purchase) Committee and acting as the Principal Accounting Officer. The
procurements are now totally dealt by the Director General Health Services.
b. Director General Health
The office of the Director General Health Services procures medicines through a Medical
Coordination Cell (MCC) and bio-medical equipments/General Goods through a newly
established Procurement Cell based on the requirements received by the DG office from
7
various Districts & Vertical Programmes. The Procurement Cell, established after the
devolution of powers to the Provincial Government in the post-18
th
Amendment era, centrally
procures the bio-medical equipment for all the Districts by conducting all the Pre-Award
procurement planning, designing the Standard Bidding Documents, conducting technical and
financial evaluations, awarding the contract and administering the post-award contractual
relationships with the suppliers. The Govt-MCC, on the other hand, is involved in the Pre-
award planning, bidding documents design , bid evaluation and subsequently awards the
contract on unit rates prevailing for the whole financial year for the selected drugs and surgical
disposables for all the field formations including EDOs (Health), MS DHQs, Autonomous
Medical Institutions (AMIs) etc which in turn conduct the post-award process by placing the
Purchase Orders themselves on need-bases during the whole year. Govt-MCC further aims at
supervising/coordinating the procurements conducted in the field after approval of the
Integrated PC-I which is meant to consolidate & centralize all divisional, regional and
Programme-oriented purchasing.
c. District Health Departments:
The Districts headed by EDOs (Health), are independent procuring entities and as per the
current policy of the Health Department these place Purchase Orders for medicines/medical
supplies on the basis of unit rates approved by the Govt-MCC & get the bio-medical equipment
centrally procured through the Procurement Cell at Directorate General Health Services GHS
as per the their requirements within the available budget allocated to them. There are twenty
five districts in Khyber Pakhtunkhwa namely, Kohistan, Bannu, Chitral, Shangla, Tank, Haripur,
Lakki Marwat, Hangu, Karak, Dir Upper, Dir Lower, Nowshera, Swabi, Abbottabad, D.I. Khan,
Battagram, Buner, Mansehra, Tor Ghar, Charsadda, Malakand, Kohat, Mardan, Swat and
Peshawar.
d. District Headquarter Hospitals (DHQs):
Headed by the Medical Superintendents, the DHQs in all the Districts are under administrative
supervision of the EDOs (Health) but the Purchase Orders for delivery of medicines & surgical
disposables selected by the Govt-MCC under unit rate contracting are placed by the respective
Medical Superintendent DHQ.
e. Autonomous Medical Institutions (AMIs):
These Institutions are also independent procuring entities at the Provincial level headed by
Chief Executives and manage their procurements on the basis of unit rates selected by the
Govt-MCC as per their requirement & available budget within the broader policy framework
defined by the Health Department. AMIs may independently procure around 40% of the total
medicines which are not included in the Govt-MCC. Their Board of Management governs
matters related to Procurements.
f. Medical Colleges:
Medical colleges are headed by the Principals and the said entities independently procure bio-
medical equipment and laboratory chemicals for their college institutions for educational and
8
experimental purposes. The colleges follow a procurement structure similar to the DGHS, with
a T&E Committee, composed of concerned Associate Professors & Professors for preparation
of equipment specifications and finalization of acquisition by a high-level Selection (Purchase)
Committee headed by the Principal of the College.
g. Health/Vertical Programmes:
Vertical Programs, also known as Stand-alone, Categorical or Disease Control Programs,
focus either on a specific disease or health issue or target a specific demographic population.
The underlying objective of Vertical Programs is to achieve specific measurable outcomes
within a given timeframe. Vertical Programs have independent management and
implementation structures headed by Program Coordinators, which run parallel and in addition
to the general health system of the Health Department of Khyber Pakhtunkhwa. Vertical
Programs have been mostly Federally funded and procure their medicines specifically related
to their scope based on the pharmaceutical items selected by the Govt-MCC on unit rate
contracting and bio-medical equipment from special program funds. The Selection (Purchase)
Committee at the Health Department finalizes the procurement. Cessation of funding of
Vertical Programs through the PSDP after the tenure of 7
th
NFC Award in 2014 has led to
provincialize some of them while maintaining their vertical nature.
h. Special Projects:
Special Projects like Aids Control obtain their funding from donors and the Government. Their
procurement methodology is similar to the Vertical Programs.
i. HSRU:
Health Sector Reform Unit, headed by Chief HSRU, is under Secretary Health and procures its
deliverables with the donor funds under the Multi-Donor Trust Funds (MDTF), spearheaded by
the World Bank. It is currently engaged in the procurement of Management Services by hiring
Consulting firms under World Banks Guidelines on Selection of Consultants. The said firms
would provide integrated health services on the basis of Public Private Partnership (PPP) to
the six crises-stricken districts in Khyber Pakhtunkhwa, namely Battagram, Buner, Dera Ismail
Khan, Dir Lower, Kohistan and Tor Ghar by upgrading the civil structures, power supplies,
transportation and bio-medical equipment etc. in the said Districts.
4.4 Procurement Entities of Health Department Khyber Pakhtunkhwa
Following is a list of the Procurement Entities of the Health Department involved in Pre-Award,
Award and post-Award activities:
1. Directorate General Health Services (DGHS), Department of Health, KP
(a) Procurement Cell
(b) Government- Medicine Coordination Cell (MCC)
2. Executive District Officer Health (EDO-H) 25 Districts
3. District Headquarter Hospitals (DHQs) 25 Districts
9
4. Vertical Programs/Projects
(a) Maternal Natal & Child Health Program
(b) National Program for Family Planning & PHC (LHW Program)
(c) EPI
(d) TB Control Program
(e) Roll Back Malaria
(f) PMs Program for Hepatitis
(g) PACP / HIV
5. Autonomous Medical Institutions (AMIs)
(a) Khyber Teaching Hospital (KTH), Peshawar
(b) Lady Reading Hospital (LRH), Peshawar
(c) Hayatabad Medical Complex (HMC), Peshawar
(d) Ayub Teaching Hospital (ATH), Abbottabad
6. Medical Colleges
(a) Khyber Medical College (KMC), Peshawar
(b) Ayub Medical College (AMC), Abbottabad
(c) Khyber Girls Medical College (KGMC), Peshawar
(d) Khyber College of Dentistry (KCD), Peshawar
(e) Bacha Khan Medical College, Mardan
(f) Swat Medical College, Saidu Sharif, Swat
(g) Kohat Institute of Medical Sciences, Kohat
(h) Bannu Medical college, Bannu
(i) Khyber Medical University
7. Health Sector Reforms Unit (HSRU), Health Secretariat, Peshawar
8. Provincial Hospitals
(a) Mardan Medical Complex, Mardan
(b) Maulvi Ameer Shah Qadri Women & Children Hospital, GT Road, Peshawar
(c) Sifwat Gahyoor Memorial (Infectious Diseases) Hospital, Haji Camp, Peshawar
(d) Naseer Ullah Babur Hospital, Kohat Road, Peshawar
(e) Govt Maternity Hospital, Hashtnagri, Peshawar
(f) nstitute of Kidney Diseases, Hayatabad, Peshawar
(g) Govt Mental Hospital, Peshawar
(h) Khalifa Gulnawaz Memorial Hospital, Bannu
4.5: Procurement Practices in the Health Department, Khyber Pakhtunkhwa
The current procurement practices of the Health Department Khyber Pakhtunkhwa are based
on a matrix management system wherein the centralized procurements are done by the two
procuring units, namely the Govt-Medicine Coordination Cell (MCC) and Procurement Cell
located at the Directorate General Health Services Peshawar.
The Govt-Medicine Coordination Cell (MCC) contracts out the unit rates of the selected
pharmaceutical products of the pre-qualified and lowest evaluated responsive pharmaceutical
firms and the bulk of the said products are in turn bought by the 25 Health Districts for their
respective BHUs and RHCs, Autonomous Medical Institutions and Vertical Programs.
10
Before the establishment of Govt-MCC in 1996, medicines were provided to the health
institutions through Medical Stores Depot (MSD). The MSD was set up at Peshawar more than
25 years ago to make bulk purchase of quality medicines in the most economical manner
ensuring their timely delivery to the Government health institutions throughout the Province.
Medicines upto Rs. 20 million were usually purchased with no fixed time frame by the MSD and
the rest by the Health Department entities locally at different rates that stated to have led to
financial irregularities. Over a period of time, it failed to achieve its objectives and Audit raised
observations regarding mismanagement, sub-standard procurements, faulty distribution, undue
cost adjustments and storage shortages etc. MSD was finally re-designated as Government
Medicine Coordination Cell (MCC) on 01.07.1996 vide Health Departments Notification No.
SOH(V)9-5/96MCC dated 16.05.1996. The Govt-MCC was supposed to annually conduct a
centralized contracting of selected pharmaceutical products through restricted competitive
bidding engaging only those pharmaceutical firms which were registered and pre-qualified
annually by the Directorate General Health Services. As the prevailing practice, an approved
Drug List comprising consolidated demand of medicines from all health institutions based on
last years purchase and with around 10% variation, is put to the above stated restricted
competitive tendering process wherein the firms with lowest rates may get the single rate
contract from the Directorate General Health Services. The said products are in turn bought by
the 25 Health Districts, Autonomous Medical Institutions and Vertical Programs etc.
This hybrid contracting methodology under the devolution of power, gives autonomy to the
chief executives of the AMIs to the extent of procuring 40% of those pharmaceutical products
which are not included in the approved Drug List (Drug Formulary) of the Govt-MCC; allows
Program Coordinators of the Vertical Programs to carry out procurements related to their
Programs and allows Executive District Officers (EDO) Health and Medical Superintendents
DHQs to carry out their related procurements for medicines and surgical disposables at District
and District Headquarter Hospital level respectively. The Departmental entities in the form of
Preliminary Scrutiny Committee, Comparative Statement Committee, Technical & Evaluation
Committee and finally the Selection (Purchase) Committee, as discussed later, are part of the
whole purchasing life cycle.
The Procurement Cell, created vide DGHS Notification No. 10760-67/Personnel, dated
30.12.2011, is supposed to purchase bio-medical equipment and occasional non-Govt-MCC
drugs on the basis of requirements sent by the Health Districts and DHQs. As per the said
notification, the Cell is headed by a Deputy Director (Admn) and manned by an Assistant
Director (Admn), Superintendent Complaint/Coordination Cell DGHS Office, Superintendent
Accounts Section, DGHS and a Computer Operator. With the two top tiers of the Cell nowhere
in sight, the potential of the Cell seems underutilized and under-staffed keeping in view the
significantly important functions and sensitive tasks of gathering the requirements of the Health
Districts, technical specification preparation and conducting procurement of bio-medical
equipment.
Procurement demand is prepared and submitted as a component/scheme of the Annual
Development Plan (ADP) of the Health Department. The demand is submitted to the Health
11
Secretariat. Specifications and requirements are prepared by the end users which get
approved by the Departmental Technical Committee. Equipment is purchased under National
Competitive Bidding (NCB) by the Procurement Cell. The purchased equipment is then
delivered to the hospital/district. The Technical Committee may physically inspect the
equipment before final selection according to the specifications mentioned in the tender. The
Technical Committee, headed by the Director General Health Services is composed of
concerned Head of Department of the medical institution and Executive Engineer of electro-
medical workshop etc. Purchases recommended by the Technical Committee are approved by
the Departmental Purchase (Selection) Committee. Minor equipment, special drugs and
medicines which are not a part of the regular hospital supply are procured through the process
of local purchase.
12
5 Section-1: Situational Analysis & Assessment of Existing
Procurement Procedures and Procuring Entities of Health
Department Khyber Pakhtunkhwa
5.1 Assessment Methodology
Under the auspices of the joint World Bank and OECD Development Assistance Committee
(DAC) Procurement Round Table initiative, developing countries, bilateral and multilateral
donors worked together to develop a set of tools and standards that provide help in assessing
the quality and effectiveness for improvements in procurement systems. The Round Table
initiative culminated with the December 2004 adoption of the "Johannesburg Declaration"
including a commitment for the adoption of the Baseline Indicators (BLIs) as the agreed
international standards for assessment of national, sub-national and agency procurement
systems.
The application of the BLIs used in the subject Assessment is based on a review of the
existing regulatory framework and the procurement related institutional and operational
arrangements in Health Department Khyber Pakhtunkhwa. The BLIs are based on four main
pillars and consist of 12 indicators. Each indicator has been further divided into four to six sub-
indicators and each having a table containing four scenarios. Each baseline sub-indicator is
preceded by a short text explaining those aspects that the sub-indicator has attempted to
assess and some considerations about the nature and importance of the item in question.
Through this short text the relevant aspects have been reviewed whether the acceptable
standard has been achieved or not. After the description of the sub-indicator, scoring against a
particular scenario has been done in the table. The scoring system ranges from 3 to 0 for each
baseline sub-indicator. A score of 3 indicates full achievement of the stated standard. A score
of 2 has been given when the system has exhibited less than full achievement and needs
some improvements in the area being assessed and a score of 1 has been given for those
areas where substantive work is needed for the system to meet the standard.
A rating of 0 has been considered as the residual indicating a failure to meet the proposed
standard. The score for each sub indicator has been a whole number from 0 to 3. Based on
subjective professional judgment by the assessor, the BLI scores will therefore be part of a
narrative report providing information on changes that are underway, but have not yet
impacted the system sufficiently to change the score. This narrative discussion has enabled
the said assessment to provide information that could not be easily reflected in numeric
scoring.
The assessment through BLIs aims at providing a basis upon which Khyber Pakhtunkhwa
Province can formulate an institutional and capacity development plan to improve its
procurement system with a long-term goal to meet internationally recognized standards which
would enable greater effectiveness in the use of public funds to meet Provincial obligations.
The methodology includes a numeric scoring with defined criteria that will provide a qualitative
grading of the Health Departments procurement system by identifying its strengths and
weaknesses. By aggregating the scores at the pillar level a graphical profile of strengths and
13
weaknesses of the Procurement system of Health Department Khyber Pakhtunkhwa has been
obtained and is displayed in the Executive Summary. The information resulting from the said
assessment would provide the Province with information it can use to monitor the performance
of its current procurement system and the success of the reform initiatives in improving its
business processes.
5.2 Introduction of Factors assessed under the Methodology
This part of the report relates to the assessment of procurement systems within the
Department of Health, Government of the Khyber Pakhtunkhwa. The assessment was
conducted as required by the TORs of the Technical Assistance-52: Strengthening the
Procurement Systems through Support and Capacity Building of Health Department, Khyber
Pakhtunkhwa for identifying gaps in the provincial legislative framework and Departmental
business processes with particular focus on:
i. Existing procurement procedures and steps being followed by the DoH entities
ii. Extent of applicability of NWFP Procurement of Goods, Works & Services Rules 2003 in
the procurement system of the DoH Khyber Pakhtunkhwa
iii. Review of each step of the procurement cycle of the Health Department from planning till
the award of contract
iv. Evaluation of levels of public access and transparency in the procurement process,
contract management mechanisms and techniques in vogue.
v. Review of the Supply Chain of the Department of Health Khyber Pakhtunkhwa and
identification of gaps, if any, and their plugging measures.
vi. Review of Procurement documentation currently used by the Department of Health.
vii. Establish suppliers issues and concerns related to procurement process and obtain their
opinions for more effective procurement.
viii. Review of contract management and disputes resolution.
ix.
Following were the four main pillars under which the above stated factors were assessed
through various Base Line Indicators:
a) Existing legal framework that regulates procurement in the Province;
b) Institutional architecture of the Procurement System;
c) Operation of the System and competitiveness of the national market; and
d) Integrity of the Procurement System.
5.3 Sampling Statistics:
The information collected is based on document reviews, key informant interviews, collection
of data from existing records and perspective observations. The interviews were carried out
with around twenty personnel related to the DoH, four Districts, seven Vertical programs, three
AMIs, two Medical Colleges and four Pharmaceutical & Bio-medical equipment suppliers etc.
14
The interview were carried out with respect to the BLI sub-indicators and on specific
questionnaires developed for data collection.
5.4 Limitations & Constraints:
1. The reliability and integrity of information collected for the Assessment was based on the
record & information provided by the Health Department.
2. Indicator-4 of Pillar-II relates to the existence of a Public procurement Regulatory Authority
in the Khyber Pakhtunkhwa Province. Until the said regulatory body starts functioning and
exerts its influence on the Procurement System of the Health Department for a significant
outcome, it remains out of the subject discussion and has therefore been rated as zero.
5.5 Summary of the Assessment Scores:
Pillar &
Indicator
Sub-Indicator Score
Sub-
Indicator
Averaged for
Pillar &
Indicator
Pillar I: The legislative and regulatory framework 2.07
Indicator 1: Public procurement legislative and regulatory framework complies
with applicable obligations with regard to national and international requirements
2.25
1(a): Scope of application and coverage of the
legislative and regulatory framework
2
1(b): Procurement methods
2
1(c): Advertising rules and time limits
2
1(d): Rules on participation
2
1(e): Tender documentation and technical specifications
3
1(f): Tender evaluation and award criteria.
3
1(g): Submission, receipt, and opening of tenders
2
1(h): Complaints
2
Indicator 2: Existence of implementing regulations and documentation 1.83
2(a): Implementing regulations that provide defined
processes and procedures not included in higher- level
legislation
1
2(b): Model tender documents for goods, works, and
services
2
15
2(c): Procedures for prequalification 3
2(d): Procedures suitable for contracting for services or
other requirements in which technical capacity is a key
criterion
1
2(e): Users guide or manual for contracting entities 2
2(f): General conditions of contracts for public sector
contracts covering goods, works, and services
consistent with national requirements and, when
applicable, international requirements
2
Pillar II: Institutional framework and management capacity
0.91
Indicator 3: The public procurement system is mainstreamed and well integrated
into the public sector governance system
2.75
3(a): Procurement planning and associated
expenditures are part of the budget formulation process
and contribute to multiyear planning
3
3(b): Procurement planning and associated
expenditures are part of the budget formulation process
and contribute to multiyear planning
3
3(c): No initiation of procurement actions without
existing budget appropriations
3
3(d): Systematic completion reports are prepared for
certification of budget execution and for reconciliation of
delivery with budget programming
2
Indicator 4: The province has a functional normative and/or regulatory body 0
4(a): The status and basis for the normative and/or
regulatory body is covered in the legislative and
regulatory framework
0
4(b): The body has a defined set of responsibilities
0
4(c): The bodys organization, funding, staffing, and
level of independence and authority sufficient and
consistent with the responsibilities
0
4(d): The responsibilities should also provide for
separation and clarity so as to avoid conflict of interest
and direct involvement in the execution of procurement
transactions
0
16
Indicator 5: Existence of institutional development capacity 0
5(a): The province has a system for collecting and
disseminating procurement information including tender
invitations, requests for proposals, and contract award
information
0
5(b): The province has systems and procedures for
collecting and monitoring provincial procurement
statistics
0
5(c): A sustainable strategy and training capacity exists
0
5(d): Quality control standards are disseminated and
used to evaluate staff performance and address
capacity development issues
0
Pillar III: Procurement operations and market practices 1.6
Indicator 6: The provincial procurement operations and practices are efficient 0.75
6(a): The level of procurement competence among
government officials within the entity is consistent with
their procurement responsibilities
0
6(b): The procurement training and information
programs for government officials and for private sector
participants are consistent with demand
0
6(c): There are established norms for the safekeeping
of records and documents related to transactions and
contract management
1
6(d): There are provisions for delegating authority to
others who have the capacity to exercise
responsibilities
2
Indicator 7: Functionality of the public procurement market 2.33
7(a): There are effective mechanisms for partnerships
between the public and private sector
2
7(b): Private sector institutions are well organized and
able to facilitate access to the market
3
17
7(c): There are no major systemic constraints (e.g.,
inadequate access to credit, contracting practices, etc.)
inhibiting the private sectors capacity to access the
procurement market
2
Indicator 8: Existence of contract administration and dispute resolution
provisions
2.0
8(a): Procedures are clearly defined for undertaking
contract administration responsibilities that include
inspection and acceptance procedures, quality control
procedures, and methods to review and issue contract
amendments in a timely manner
2
8(b): Contracts include dispute resolution procedures
that provide for an efficient and fair process to resolve
disputes arising during the performance of the contract
1
8(c): Procedures exist to enforce the outcome of the
dispute resolution process
3
Pillar IV: Integrity and transparency of the public procurement system 2.0
Indicator 9: The province has effective control and audit systems 1.59
9(a): A legal framework, organization, policy, and
procedures for internal and external control and audit of
public procurement operations are in place to provide a
functioning control framework
2
9(b): Enforcement and follow-up on findings and
recommendations of the control framework provide an
environment that fosters compliance
2
9(c): The internal control system provides timely
information on compliance to enable management
action
3
9(d): The internal control systems are sufficiently
defined to allow performance audits to be conducted
0
9(e): Auditors are sufficiently informed about
procurement requirements and control systems to
conduct quality audits that contribute to compliance
1
18
Indicator 10: Efficiency of Appeals Mechanism 2.19
10(a): Decisions are deliberated on the basis of
available information, and the final decision can be
reviewed and ruled upon by a body (or authority) with
enforcement capacity under the law
2
10(b): The complaint review system has the capacity to
handle complaints efficiently and a means to enforce
the remedy imposed
2
10(c): The system operates in a fair manner, with
outcomes of decisions balanced and justified on the
basis of available information
3
10(d): Decisions are published and made available to
all interested parties and to the public
1
10(e): The system ensures that the complaint review
body has full authority and independence for resolution
of complaints.
3
Indicator 11: Degree of access to information 2.0
11(a): Information is published and distributed through
available media with support from information
technology when feasible
2
Indicator 12: The Province has ethics and anticorruption measures in place 2.14
12(a): The legal and regulatory framework for
procurement, including tender and contract documents,
includes provisions addressing corruption, fraud,
conflict of interest, and unethical behavior and sets out
(either directly or by reference to other laws) the actions
that can be taken with regard to such behavior
3
12(b): The legal system defines responsibilities,
accountabilities, and penalties for individuals and firms
found to have engaged in fraudulent or corrupt
practices
2
12(c): Evidence of enforcement of rulings and penalties
exists
3
12(d): Special measures exist to prevent and detect
fraud and corruption in public procurement
1
19
12(e): Stakeholders (private sector, civil society, and
the ultimate beneficiaries of procurement and/or end-
users) support the creation of a procurement market
known for its integrity and ethical behavior
2
12(f): The province should have in place a secure
mechanism for reporting fraudulent, corrupt, or
unethical behavior
2
12(g): Existence of codes of conduct or codes of ethics
for participants that are involved in aspects of the public
financial management systems that also provide for
disclosure for those in decision-making positions
2
5.6 Pillar I Legislative and Regulatory Framework
Indicator-1: Public procurement legislative and regulatory framework achieves the agreed
standards and complies with applicable obligations.
The indicator covers the legal and regulatory instruments from the highest level (national law, act,
regulation, decree, etc.) down to detailed regulation, procedures and bidding documents formally in
use. This indicator is broken down into eight sub-indicators (a-h) which are individually scored.
Sub-indicator 1(a) Scope of application and coverage of the legislative and regulatory
framework (For Directorate General Health Services, Vertical Programs & AMIs).
The said sub-indicator determines:
a) The structure of the regulatory framework governing the public procurement;
b) The extent of its coverage; and
c) The public access to the laws and regulations
After the abolition of concurrent legislative list through 18
th
Amendment in the Constitution of
Pakistan, the NWFP Procurement of Works, Goods & Services Rules 2003 promulgated through
NWFP Procurement of Works, Goods and Consultancy Ordinance 2002 are in vogue. The said
Rules originated in 2003 for procurement of civil works, supply of general goods and consultancy
services and were oriented towards construction works and related supplies by the civil contractors
and general suppliers. Though covering most of the procurement functions at that point of time and
spearheading the procurement legislation in the Country, the said Rules now seem deficient in
various aspects relating to procedures and thus suffer structural infirmities in view of the evolution in
international Procurement Law. Clauses relating to some of the procedures in the said Rules e.g.,
submission of bid security, negotiations on financial bids and contracting methodologies treat the
subject matter inadequately, are not in line with current international best practices or with
procurement practices prevalent at the Federal level; and are also in conflict with donor guidelines
on certain aspects. The said NWFP Procurement Rules 2003 are not designed to address the
particular needs of procurement of specialized items like drugs, vaccines and surgical disposables
20
wherein product efficacy plays major role in evaluating the quotes offered. Acquisition of Bio-
Medical equipment further requires well-defined product specifications for which these rules provide
no viable mechanism to deliberate upon any product definition.
The Directorate General Health Services (DGHS), Health Department Khyber Pakhtunkhwa located
at Health Secretariat Peshawar, had been previously engaged in procuring the medicines and bio-
medical equipment through a three-page Bidding Document alongwith an approved drug
list/formulary on the basis of single Stage Single Envelop bidding procedure. Under the judicial
directives in Writ Petition No. 3129/2010 dated 15.05.2012 of the Honourable Peshawar High Court
to clearly define its procurement policy and post it on DoH website, the Department, in 2012,
decided to conduct procurement of bio-medical equipment and drugs through Two-Stage Tendering
Process under Rule-40 of the NWFP Procurement Rules 2003. It therefore adopted semi-structured
bidding documents based on a sample WHO template for procurement of Bio-Medical equipment in
May 2012 for conducting procurements under the said Rules. Recently, the procurement of Drugs &
Surgical Disposables has also been carried out in August 2012 through the fully structured revised
Standard Bidding Documents (SBDs). These SBDs are based on internationally recognized FIDIC
templates as per the said Rules under Two Envelop Tendering process and the unit rates for the
selected drugs have been finalized and circulated among all the related procuring entities by the
Govt-MCC for the whole Province. Similarly, Vertical Programs relating to the Maternal Natal and
Child Health (MNCH) in the Province has also taken its procurement initiative for the acquisition of
CMW Kits for the Health districts by adopting the above stated revised Standard Bidding
Documents in September 2012 under the said Rules. Accordingly, Technical & Evaluation (T&E)
Committee and Selection (Purchase) Committee, officially nominated by the office of Secretary
Health for bid evaluation and contract award, have finalized the said activity. Surprisingly, some
Provincial procuring entities like the Autonomous Medical Institutions (AMIs) e.g., Lady Reading
Hospital Peshawar are still not following the business processes under the said Rules and are
acquiring non-drug surgical disposables through the old three-page single stage single quotation
system despite Honourable Peshawar High Courts order on Suo Moto action in Writ Petition No.
3129/2010 dated 15.05.2012 to adopt a clear procurement policy by using the detailed Standard
Bidding Documents.
The NWFP Procurement Rules 2003 draw their strength from Section 45 of the North West Frontier
Province Procurement of Goods, Works & Consulting Services Ordinance, 2002. The adequacy of
the structure of the said regulatory framework is enshrined in the NWFP Procurement Rules 2003
and may be rated as bare minimum for procurement activities in the Health Department. That is why
Standard Bidding Documents, based on internationally recognized FIDIC templates, have been
adopted and customized as per the requirements of the health sector purchasing. The regulatory
framework in the form of NWFP Procurement Rules 2003 contain as an Appendix, the General
Principles for Evaluation of Application for Pre-Qualification and Technical Bids for Post-
Qualification, which elaborate the evaluation process of the bids received in three stages. These
Principles, as their name suggests, are just procedural guidelines for the evaluation committees to
harmonize their efforts towards achieving their goal through some standard practices. The
regulatory impact of the said principles is not defined in the Procurement Rules 2003.
21
The uniformity of coverage of the current legal framework in the form of NWFP Rules 2003 is
therefore not fully applicable on the procurement activities related to health-sector goods initiated by
the Health Department entities using public funds. Presently, no administrative approval is in place
for excluding any autonomous entity related to Health Department KP from adoption of Standard
Bidding Documents and two envelop tendering as per Rule 40 of NWFP Procurement Rules 2003.
This may contribute to unpredictability and distortion in the new business processes adopted by the
Health Department and may add to excessive costs in the operation of the procurement system.
NWFP Procurement of Works, Goods & Services Rules 2003, while having been published in
NWFP Local Government Planning Manual in 2003, are neither publicly accessible on any web-
portal of Health Department KP nor on the Government of Khyber Pakhtunkhwa website which
displays only North-West Frontier Province Procurement of Goods, Works, Services and Consulting
Services Ordinance, 2002. It is worth mentioning that the said website hosts more than 900
different public rules, regulations, acts & laws made since 1798 till 2008 spanning over two hundred
years. While having met procurement officials of many autonomous entities of Health Department, it
was revealed that they seldom have the copies of the NWFP Procurement Rules 2003.
Scoring criteria Score
The legislative and regulatory body of norms complies with all the following
conditions:
(a)
Is adequately recorded and organized hierarchically (laws, decrees,
regulation procedures,) and precedence is clearly established. All laws
and regulations are published and easily accessible to the public at no
cost.
3
(b)
All laws and regulations are published and easily accessible to the public
at no cost
(c)
It covers goods, works and services (including consulting services) for
procurement using national budget funds.
The legislative and regulatory body of norms complies with (a) plus one of
the above conditions
2
The legislative and regulatory body of norms complies with (a) of the above
conditions.
1
The system does not substantially comply with any of the above conditions. .
0
Sub-indicator 1(b) Procurement Methods:
This sub indicator assesses whether the legal framework includes:
a) a clear definition of the permissible procurement methods; and
b) the circumstances under which each method is appropriate.
The legal framework provided by the NWFP Procurement of Works, Goods and Services Rules
2003 makes, under Rule 7, open competitive tendering the default method of procurement in
22
Khyber Pakhtunkhwa Province. All procurements exceeding financial thresholds of Rs 5 million for
contracts of non-development works, and those exceeding Rs 10 million for contracts of
development works need pre-qualification or post-qualification of suppliers or contractors with
unlimited participation. Pre-qualified suppliers or contractors offer their technical and financial
proposals as per Rule 40 under the Two Envelop Single Stage Tendering procedure which is a
restricted tendering process if only pre-qualified bidders participate as opposed to post-qualification.
However, opportunity to get pre-qualified in Khyber Pakhtunkhwa Province Health Department is
open to firms all across the Country. Rule 35 further defines the types of contracts with estimated
costs ranging from Rs 40,000 to Rs 5,00,000 to attract Request For Quotation (RFQ) procedure
with a minimum of three quotations / bids and prohibits fractioning of contracts to avoid open
competition. The Health Department Khyber Pakhtunkhwa abides by the stated financial thresholds
for competitive bidding.
Rule 36, 38 & 39 define the non-competitive procedures relating to Single Source Procurement,
Repeat Orders and Restricted Tendering respectively under specific circumstances. Financial
negotiations are allowed under Rule 37 upon approval from the Procuring Entity to safeguard
against quoting of exorbitant prices in Single Source Selection procedure. Currently financial
negotiations are considered inconsistent with the appropriate international standards for competitive
bidding and are apparently not being used by the Health Department Khyber Pakhtunkhwa.
Interestingly, the language regarding prohibition of financial negotiations in the Khyber
Pakhtunkhwa Public Procurement Rules 2012 expected to be notified by the Government soon,
also seems to bear the seeds of NWFP Procurement Rules 2003 and is considered lenient
compared to the Federal PPRA Rules 2004.
There is no specific law or set of rules supplemental to procurement of health-sector goods. Drugs
& surgical disposables are purchased in line with the Drug Act 1976 and NWFP Procurement Rules
2003. As per Rule 4 the NWFP Procurement Rules 2003, procurement of essential items & goods
of immediate nature, in case of emergency, is to be carried out by a committee consisting of District
Coordination Officer, District Revenue & Estate Officer and Executive District Officer (Finance &
Planning) by utilizing non-competitive contracting methods under Rules 36, 38 & 39 of the NWFP
Procurement Rules 2003. The said procedure is not being followed by the AMIs and direct
administrative sanction of Secretary Health is the sole means to tackle urgent procurements through
frequent purchase orders in emergency situations from the Emergency Relief Package (ERP)
Funds. Sometimes, in case of more emergencies, funds from the regular budgets for the AMIs are
transferred to the ERP funds with approval of the Competent Authority. The above said transient
practice is not in line with the afore-stated Rule 4 which may be due to the peculiar nature of
emergencies in the hospitals owing to the law & order situation in the Province and wherein timely
decision-making of such committees may be of little use. However, this may also relate to the
absence of a revised procedural setup after the devolution of powers to the Provinces under the 18
th
Constitutional Amendment.
Appropriate hierarchical levels have been established in the Health Department Khyber
Pakhtunkhwa through various Departmental committees consisting of health sector professionals
namely, Pre-Qualification Committee, Scrutiny Committee, Comparative Statement (CS)
Committee, Technical & Evaluation Committee and lastly the Purchase Committee to examine the
23
bids under a competitive bidding method. Composition of the said committees for a typical activity
regarding procurement of drugs and medicines is as under:
Committee Composition for Govt-MCC Procurements of Drugs
Functions:
1. Visit business premises of manufacturers and importers of pharmaceutical products and bio-
medical equipment all across the Country.
2. Submit Inspection Report to the Chairman Technical & Evaluation Committee within three days
of inspection for evaluation of firms for pre-qualification.
A typical Pre-Qualification Committee is mostly composed of 4-6 members selected from
among the designations mentioned above for different industrial estates in the Province and
the Committee may further divide the areas amongst sub-committees made from its members.
Technical Bids Scrutiny Committee:
S.No Designation
1. Deputy Director Administration DGHS KP Chairman
2. Drug Inspector, EDO (Health) Peshawar Secretary Member
3. Chief Pharmacist Lady Reading Hospital Peshawar Member
4. Section Officer (Drugs), DoH, Peshawar Member
5. Pharmacist Govt-MCC, DGHS Co-opted Member
Functions:
1. Carry out preliminary screening of the Technical bids received from the pre-qualified bidders
and develop their risk profiles in view of the documentation contained in the Technical Bids.
Pre-Qualification Committee:
S.No Designation
1. Additional Secretary (Dev) Health KP / DGHS KP / Medical
Superintendent LRH Peshawar / Director Admn, DGHS KP
Chairman
2. Professor of Surgery LRH Peshawar Member
3. Professor of Medicines LRH Peshawar Member
4. Deputy Secretary (Budget), Health Department, Peshawar Member
5. Chief Drug Inspector Peshawar Member
6. Deputy Director Pre-Qualifications Member
7. Pharmacist, Govt-MCC, DGHS Member
8. Drug Inspector, EDO (Health) Peshawar Member
24
2. Point out the deficiencies in secondary documentation and recommendation to the Technical &
Evaluation Committee for taking appropriate action in this regard.
3. After carrying out the preliminary screening, to submit the report to the Chairman Technical &
Evaluation (T&E) Committee for detailed evaluation of the Technical Bids by the T&E
Committee.
Note: With the recent, introduction of the new Standard Bidding Documents for procurement
of Drugs & Surgical Disposables, the Scrutiny Committee does all the preliminary screening
and risk profiling of the Bidders and the products offered by them by sifting out relevant data
required by the SBDs, getting the secondary documentation completed by the bidders and
preparing bidders corporate and product snapshots on the standard prescribed Bid Evaluation
Proformas for the various categories of suppliers, namely manufacturers/importers of general
drugs, manufacturers/importers of biological drugs, and manufacturers/importers of surgical
disposables and medical devices. The Preliminary Scrutiny Committee then submits screened
profiles of bidders and their products to the T&E Committee thereby informing them of bidders
preliminary compliance with the technical evaluation criteria with recommendations on certain
technical aspects of the bids for taking decision. This facilitates the T&E Committee to conduct
a detailed evaluation of the technically qualified bidders.
Comparative Statement (CS) Committee
S.No Designation
1. Deputy Director Personnel DGHS KP Chairman
2. Deputy Secretary Budget DGHS KP Secretary Member
3. Section Officer Drugs Health Department KP Member
4. Pharmacist, Govt-MCC KP Member
Functions:
1. Prepares a Comparative Statement (CS) of quotations after public opening of the financial bids
of the technically qualified bidders by the Technical & Evaluation (T&E) Committee.
2. Submits the CS to the Chairman Technical & Evaluation Committee for approval of Selection
(Purchase) Committee.
Technical & Evaluation (T&E) Committee:
S.# Designation
1. Additional Secretary(E&A), Govt: of Khyber Pakhtunkhwa Chairman
2. DGHS KP Secretary Member
3. Professor of Medicine, LRH Member
4. Professor of Surgery, LRH Member
5. Representative from Pharmacy Department, University of
Peshawar
Member
6. Senior Hospital Pharmacist, Kohat / Bio-medical Engineer Member
25
DGHS KP
7. Deputy Secretary (Drugs) Member
8. Medical Superintendent, LRH, Peshawar Member
Functions:
1. Carries out evaluation of different manufacturers and importers of drugs/bio-medical
equipment for pre-qualification for the purpose of Govt-MCC or DGHS Procurement Cell as
and when required.
2. Submits pre-Qualification Report to the Chairman Purchase Committee for approval.
3. Constitutes Technical Bids Scrutiny Committee or Comparative Statement Committee for
preparation of Comparative Statement for approval of the Purchase Committee.
4. Co-opts any person considered relevant to the process of evaluation.
5. Opens financial bids for selecting the lowest rates for drugs and bio-medical equipment quoted
by pre-qualified firms under centralized rate selection rgime.
6. Carries out clinical trials of drugs of various brands/types prior to selection of the drugs by the
Technical Bids Scrutiny Committee of Govt-MCC and instrument testing of bio-medical
equipment.
7. Performs any other task, if assigned.
8. Requires two third of its members to convene its meetings.
Selection (Purchase) Committee:
S.No Members
1. Secretary Health, Khyber Pakhtunkhwa Chairman
2. Additional Secretary Health (Dev), Khyber Pakhtunkhwa Vice Chairman
3. Director General Health Services, Khyber Pakhtunkhwa
/Officer Incharge
Secretary member
4. Professor of Medicine, HMC Member
5. Professor of Surgery, LRH Member
6. Professor of Gynaecology & Obstetrics Member
7. Professor of Pharmacology from any public sector Medical
College.
Member
8. Chief Pharmacist, Lady Reading Hospital Peshawar Member
9. Chief Drug Inspector, DGHS, Peshawar Member
Functions:
1. Approves pre-qualification of firms for Govt-MCC.
2. Approves pre-qualification of suppliers of Bio-Medical Equipment
3. Selects & approves pharmaceutical and bio-medical products and their rates from technically
qualified firms for Govt-MCC and Procurement Cell.
26
4. Co-opts any person considered necessary for carrying out the purpose of the Committee.
The above said committees are officially notified by Secretary Health annually though their
composition mostly remains the same with addition or replacement of some technical or
administrative entity. These committees tend to reasonably control and minimize the discretion of
individual agencies or procurement officials in using the methods that limit competition.
Committee Compositions for Procurement Cell Procurements for Bio-Medical Equipment
etc.:
Equipment & Instruments Committee:
S.No Designation
1. Additional Secretary (Dev) Health KP Chairman
2. Chief Drug Inspector Peshawar Secretary / Member
3. Bio-Medical Engineer Member
4. MS HMC Member
5. MS KTH Member
6. MS LRH Member
Functions:
1. Pre-Qualification of firms producing non-drug surgical disposables & Bio-Medical equipment.
2. Visit business premises of manufacturers and importers of pharmaceutical products and bio-
medical equipment
3. Submit Inspection Report to the Chairman Technical & Evaluation Committee within three days
of inspection for evaluation of firms for pre-qualification.
Inspection Committee:
S.No Designation
1. Senior Planning Officer-I Chairman
2. Concerned MS of Hospital Secretary / Member
3. Concerned EDO (H) of the District Member
4. Concerned Engineer of electro-Medical workshop Member
Functions:
1. Inspect the equipment purchased under the Development Schemes/Projects/Programs.
2. Check the installation & commissioning of equipment
3. Check the operationalization of the equipment & submit report to the Provincial Technical
committee & Provincial Purchase Committee.
4. Check record of payment in respect of procurement of equipment by the MS / EDO(H) / PM /
PD / Coordinator
5. Recommend disciplinary action against the MS/ EDO(H)/PM/PD/Coordinator concerned in
case of payment before the supply or operationalization of the equipment.
27
Technical Committee:
S.No Designation
1. Director Public Health, DGHS, Peshawar Chairman
2. Concerned Head of Department of LRH & KTH or their
representatives not below the rank of Associate Professors &
KCD in case of dental departments.
Secretary / Member
3. Executive Engineer Electro-Medical Equipment Workshop Member
4. Any other co-opted member expert in the field Member
Functions:
1. Preparation of Technical Specifications
2. Evaluation of Technical Bids
3. Inspection of Samples (if required) before final selection
4. Submission of final Technical & evaluation report within prescribed period to the
Purchase Committee for final approval.
5. Ensure technical evaluation of non-Govt-MCC drugs / drugs not quoted by bidders / included in
PC-I, to ease process of procurement of drugs
Purchase Committee:
S.No Designation
1. Secretary Health Chairman
2. Director General Health Services Secretary / Member
3. Chief Planning Officer, Health Department Member
4. Project Coordinator/MS/EDO (H) Member
5. Assistant Project coordinator Member
6. Any Co-opted member Member
Functions:
The Committee shall follow the procurement guidelines of the NWFP Procurement Rules 2003 and
World Bank Guidelines for procurement of deliverables in MTDF Project.
Scoring criteria Score
The legislative and regulatory body of norms complies with all the following
conditions:
(a) Allowable procurement methods are established unambiguously at an
appropriate hierarchical level along with the associated conditions under
which each method may be used, including a requirement for approval by
an official that is held accountable.
3
28
(b) Competitive procurement is the default method of public procurement.
(c) Fractioning of contracts to limit competition is prohibited.
(d)
Appropriate standards for international competitive tendering are specified
and are consistent with international standards
The legal framework meets the conditions of (a) and (b) plus one of the remaining
conditions.
2
The legal framework meets the conditions of (a) and (b). 1
The legal framework fails to substantially comply with any three of the conditions
(a) through (d).
0
Sub-indicator 1(c) Advertising Rules and Time Limits
This sub indicator assesses whether:
a) the legal framework includes requirements to publish contract awards as a matter of public
interest and to promote transparency;
b) there is wide and easily accessible publication of business opportunities; and,
c) there is adequate time provided between publication of opportunities and submission date,
consistent with the method and complexity of the procurement, to prepare and submit
proposals.
Rule 11(3) of the NWFP Procurement Rules 2003 permits the Tender Inviting Authority to provide
atleast fourteen days as minimum time between publication of Notice for Pre-Qualification in two
national dailies and the submission of Pre-qualification documents. In case of any clarification
sought by a contractor or supplier, the Tender Inviting Authority responds to the said request atleast
seven days prior to the deadline of submission of the application to pre- or post-qualify. The Health
Department abides by the stated time limits in the pre-qualification procedures.
Rule 20 (1) of the said Rules allows a minimum of thirty days between date of publication of the
Tender Inviting Notice (term used in the Rules for the Invitation For Bids) and submission of bids /
proposals. However, its sub-clause (2) authorizes head of the Procuring Entity to reduce this
mandatory time for reasons to be recorded in writing. As observed, this sub-clause has been used
to reduce this time to fourteen days or even one week in most of the procurement instances by the
procuring entities of the Health Department either owing to meeting an acquisition deadline or some
administrative expediency to avoid lapse of appropriated funds. On one side this reflects that the
planning side of the Department is either inadequately managed or ad-hoc based and on the other
side the standard time gets reduced wherein the prospective bidders could have adequately
prepared their bidding documents to quote well-thought prices, had more time be given to them.
Although content of the Invitation For Bids (IFB) for procurement of Pharmaceutical Products for
Govt-MCC DGHS for the year 2012-13 included sufficient information to enable potential bidders
to determine their ability and interest in bidding, the recently introduced Standard Bidding Document
for the said activity witnessed many revisions in the Technical Evaluation Criteria till the last minute
due to the deliberations between the bidders and the Health Department in the subsequent Pre-Bid
29
Meetings whose minutes could neither be circulated properly among the bidders through an
addendum published in a newspaper due to paucity of time nor could reasonable time be given to
them to reflect these changes in their Bidding Documents; hence majority of bids faced infirmities in
their secondary documentation despite the posting of the revised Standard Bidding documents on
the newly created DHIS web-link for the Govt-MCC.
The silence of NWFP Procurement Rules 2003 on providing a minimum time limit to bidders for
incorporating any such changes made by the client after the Pre-Bid Meeting has considerably
compromised the objective of promoting transparency in the bidding process and has reduced the
quality and level of competition expected. If multi-national firms having their business components
abroad are expected to compete, as many of them have participated through their pre-qualified local
offices, this is a serious factor to consider. The law and regulations should establish the criteria for
setting the minimum time between advertisement and submission of bids/proposals through some
administrative notification for competitive bidding, atleast for the time till the notification of the draft
Khyber Pakhtunkhwa Public Procurement Rules 2012 by the Government.
Scoring Criteria Score
The legal framework meets the following conditions:
3
(a)
Requires that procurement opportunities other than sole source or price
quotations be publicly advertised.
(b)
Publication of opportunities provides sufficient time, consistent with the
method, nature and complexity of procurement, for potential bidders to
obtain documents and respond to the advertisement. Such timeframes
are extended when international competition is sought.
(c)
Publication of open tenders is mandated in at least a newspaper of
wide national circulation or in a unique Internet official site, where all
public procurement opportunities are posted, that is easily accessible.
(d)
Content of publication includes sufficient information to enable potential
bidders to determine their ability and interest in bidding.
The legal framework meets the conditions of (a) and (b) plus one of the
remaining conditions.
2
The legal framework meets the conditions of (a) plus one of the remaining
conditions.
1
The legal framework only meets the conditions of (a) above. 0
Sub-indicator 1(d) Rules on participation:
This sub indicator assesses the participation and selection polices to ensure that these are non
discriminatory. As a general principle under this sub-indicator, firms, including pre-qualified
multinational firms/importers or suppliers, should not be excluded from participating in a tendering
process for reasons other than lack of qualifications. Those exclusions from the tendering process
that are not based on the qualifications of the firm, may arbitrarily limit competition and may result in
inefficient procurement and higher prices.
30
The Department of Health Khyber Pakhtunkhwa annually pre-qualifies manufacturers, importers or
supplier of bio-medical equipment and pharmaceutical products and surgical disposables whether
the said entities are local or multi-national. All such firms are therefore eligible for participation in the
competitive bidding process for supplying the above mentioned goods. The policies of the Health
Department in this regard are non-discriminatory and result in creating a pool of pre-qualified firms
from whom the Department strives in good earnest to procure quality pharmaceutical products and
equipment. However, it was observed that in certain procurement activities initiated by the
Directorate General of Health Services, Vertical Programs and AMIs, technically qualified bidders
were excluded on account of Rule 34 of the NWFP Procurement Rules 2003, from further
competition when less than three such bidders survived the technical evaluation phase. Right to
audience under Rule 32 of the said Rules was also not accorded to the surviving technically
qualified bidder in the referred cases to present a detailed analysis of workability of his bid before
the Department. A new procurement process therefore used to be re-initiated ensuring minimum of
three technically qualified bidders till the end by relaxing the evaluation criteria despite the fact that
in re-bidding, participation of a minimum of only two bidders is required at the time of bid submission
under Rule 34 of the said Rules. An analysis of these persistent practices in the light of
interpretation of afore mentioned Rules 34 & 32, therefore reveals a distorted interpretation of the
Rule 34 and tends to limit competition and induce rigidity in the business process resulting in
inefficient procurement and higher prices.
Rule 34 of the NWFP Procurement of Works, Goods and Services Rules 2003 states as under:
34. Modes of Procurement: (1) Except as otherwise provided by these rules, a Procuring Entity
for the Procurement of Goods, Works or Services shall adopt tendering proceedings.
(2) For the purpose of transparency, fair competition and efficiency, the Procuring entity shall
cause evaluation of offers, proposals or tenders only where a minimum of three responses
have been received, unless the Head of the Procuring Entity authorizes the evaluation of less
than three tenders after publishing a Notice Inviting Tenders for a second time in the
newspapers of wide circulation and for cogent reasons to be recorded in writing of the
Procuring Entity authorizes the evaluation of less than three tenders.
The above mentioned Rule 34 states the condition of submission of a minimum of three quotations /
responses by the bidders in the first round of invitation for Bids. These bids (a minimum of three for
the purpose of transparency, fair competition and efficiency) are required to be submitted to the
Procurement Entity at the Bid submission stage and the same will then be scrutinized in Stage-I
through Preliminary Screening as per General Principles For Evaluation of Application for Pre-
Qualification & Technical Bids for Post-Qualification (Appendix to the Rules 2003). Subsequent to
the Preliminary Screening, detailed evaluation is conducted by the Technical & Evaluation
Committee in Stage-II as per the above said General Principles. Whosoever, emerges as the lowest
evaluated responsive bidder, will be awarded the contract. The above stated Rule 34 and the
General Principles do not, at any stage, mention that all the three bidders who initially submitted
their bids have to emerge as technically qualified till the end. The said Rule also does not state that
any one bidder, who has emerged among the crowd as the sole technically qualified bidder during
31
the Preliminary Screening / Technical Evaluation, has to be excluded from the competition only
because other bidders have been rendered technically disqualified during the said preliminary
screening or technical evaluation. The guiding principle behind retaining in the competition the sole
technically qualified bidder, is embedded into the international best practice adopted World-wide by
all the donor institutions and OECD countries in their procurement rgimes, whereby a technically
qualified bidder is not penalized for the disqualification or absence of the other bidders, i.e., he
should not be disqualified for a mistake he has not committed.
Rule 32 of the NWFP Procurement of Works, Goods and Services Rules 2003 mentions the
discretion of the Tender Accepting Authority to reject all tenders, proposals, offers or quotations at
any time prior to the acceptance of a tender, proposal, offer or quotation. This rejection is based on
the assumption that the bid is unworkable. However, before rejection of tender on the said basis,
the stated Rule mentions that the Tender Accepting Authority has to give an opportunity to the said
bidder, upon his request, to demonstrate the workability of his bid. As a matter of opinion,
Justification of rejection of a workable bid of a technically qualified bidder by the Tender Accepting
Authority would be difficult if his price quotation is well within the budget allocated or nearly matches
the unit rate previously received by the client. The legal as well as audit implications of excluding
such a single technically qualified bidder for no cogent reason by the Procuring Entity may have to
be measured against delaying the purchasing process leading to subsequent acquisition of the
intended items on increased market prices and a belated health service delivery.
There may be cases in which the legal framework may allow restrictions that require purchasing
from or associating with domestic firms, or mandate the inclusion of a minimum locally
manufactured content. Many countries also allow price preferences for domestic firms. Excessive
price preferences or other concessions for domestic bidders may therefore deter effective
competition and reduce gains in efficiency.
Though the NWFP Procurement Rules 2003, under which the procurement of pharmaceutical
products and Bio-medical equipment are purchased, do not bar participation of any foreign or local
firm, these do require mandatory pre-qualification vide NWFP Government Notification No.
SOH(V)9-5/96(MCC), dated 20
th
May 1996 of all foreign/multi-national and local pharmaceutical
drugs manufacturers & distributors (distributors now banned by the Honourable Peshawar High
Court vide Para 9 of the Writ Petition No. 2478/2010 - Daily Mashriq Vs Secretary Health & Others)
by the Health Department Khyber Pakhtunkhwa as a condition to participate in a bid which may
become an entry barrier for many foreign firms as importers which have no pre-qualification profile
with the DGHS Khyber Pakhtunkhwa. The foreign firms must register with the Sales Tax
Department as importers and get pre-qualified accordingly with the Health Department Khyber
Pakhtunkhwa. However, keeping in view of the restrictions of Import Policy Order 2012-13, prior
verification of current Good Manufacturing Practices (cGMP) and pharmaceutical raw material
source gradation by the DGHS to achieve drug efficacy, pre-qualification requirement seem to out-
weigh the merits of an open no-barrier competition. Interestingly, in some procurement activities
relating to acquisition of bio-medical equipment, it has been observed that the said pre-qualification
requirement for suppliers not registered with the Health Department Khyber Pakhtunkhwa has been
waived of by the concerned procurement entity on depositing of double the amount of the bid
32
security to entertain them on-the-spot for post-qualification at the time of bid submission. Except for
the supply of drugs, medicines and surgical disposables where pre-determination of manufacturing
quality is essentially required to ensure product efficacy, there is no harm in considering the un-
registered suppliers of non-pharmaceutical products provided the option of their post-qualification at
the time of bid submission is already mentioned in the Standard Bidding Documents to ensure
transparency and wider competition. A strict interpretation of the Rule 8 regarding pre-qualification
of suppliers further suggests that the criteria set by the Health department for the said process are
not pre-qualification but are rather registration and industrial process verification by the Department.
Rules 9 & 10 of the NWFP Procurement Rules 2003 provide for the conditions under which a
suppliers bid can be rejected or he can be debarred from current or future procurement activities
e.g., his failure to perform in earlier contracts, making a cartel, submitting a false information or his
inducement to procurement officials. These Rules are then supplemented by the allied laws like
Drug Act 1976. However the stated Rules offer little in regard to grievance redressal in response to
any administrative debarment of a supplier on procurement matters. The Provincial Quality Control
Board (PQCB) Khyber Pakhtunkhwa under Section-11 of the Drug Act 1976 deals with the drug
quality control issues and subsequent prosecution of drug manufacturer/seller etc. The concerned
Licensing Board, constituted under Section-5 and Registration Board constituted under Section-7 of
the Drugs Act 1976, also deal with cancellation of registration and licensing of drug manufacturers.
This has therefore significantly reflected upon the existing complaint-handling procedures and
appeal forums with limited procedural & appropriate forum definition by the Health Department in
offering a due process to the barred/blacklisted supplier regarding rebuttal of any such allegations
on him pertaining to submission of false documentation, breach of contract or any other
procurement related issues. Hence, various complaints against debarments, disqualifications and
tender rejections at the DGHS, Vertical Programs and the AMIs in the Health Department Khyber
Pakhtunkhwa are being filed with different forums including the Honourable Peshawar High Court,
NAB and the Provincial Ombudsman Secretariat (under section 31 of the Khyber Pakhtunkhwa
Provincial Ombudsman Act 2010) instead of utilizing the appropriate forum like the office of the
Secretary Health. An independent Provincial Drug Court has recently been notified in October
2012 and awaits appointment of judges with so far no functional Terms of Reference in sight. Apart
from deciding the cases of spurious drugs and cancellation of drug licenses, its utility to fill the gap
of a proper Provincial Appellate Forum for procurement-related grievances is yet to be seen.
Scoring Criteria Score
The legal framework meets the following conditions:
3 (a)
Establishes that participation of any contractor or supplier or group of
suppliers or contractors is based on qualification or in accordance with
international agreements; requires the use of pass/fail basis for
determining qualifications to extent possible; limits domestic price
preferential, if allowed, to a reasonable amount (e.g.15% or less); and
requires justification for set asides that limit competition.
33
(b) Ensures that registration if required does not constitute a barrier to
participation in tenders and does not require mandatory association with
other firms.
(c) Provides for exclusions for criminal or corrupt activities, administrative
debarment under the law subject to due process or prohibition of
commercial relations.
(d) Establishes rules for the participation of government owned enterprises
that promote fair competition.
The law and regulations meet the conditions of (a) and (b) plus one of the
remaining conditions.
2
The law and regulations meet the conditions of (a) plus one of the remaining
conditions.
1
The law and regulations do not meet the conditions of a) through d) above. 0
Sub-indicator 1(e) Tender documentation and technical specifications
The sub indicator assesses the degree to which the legal framework specifies the content of
tendering or solicitation documents to enable suppliers to understand clearly what is requested from
them and how the tendering process is to be carried out.
Whereas Rule 23 of the Federal Public Procurement Rules 2004 clearly outlines a detailed list of
components to structure the Standard Bidding Documents (SBDs) for any competitive bidding, the
NWFP Procurement Rules 2003 do not particularly specify the content of the tendering documents
as to enable suppliers to understand clearly what is required from them and how the tendering
process is to be carried out. However, Rule 11 of the NWFP Procurement Rules 2003 dealing with
the Pre & Post-Qualification proceedings for the suppliers and contractors includes certain
information regarding instructions for preparing and submitting the pre or post-qualification
applications, a summary of the required terms and conditions of the contract to be entered into a
result of the procurement proceedings, documentary evidence required to be submitted by the
bidders in this regard and lastly, manner and place for submission of the said applications.
Rule 14 of the NWFP Procurement Rules 2003 further enumerates contents of invitation to pre or
post-qualify and invitation to tender which include the name & address of the Tender Inviting
Authority, nature, quantity and place of delivery of the goods to be supplied, the desired time for the
supply of goods, the criteria & procedure to be used for evaluating the qualifications of suppliers or
contractors, price for pre-qualification or tender documents, terms and conditions for payment of
mobilization advance and finally the place and deadline for the submission of tenders. The General
Principles for Evaluation of Application for Pre-Qualification & Technical Bids for Post-Qualification
(Appendix to the NWFP Procurement Rules 2003) also indicate some parameters relating to the
technical and financial evaluation of bidders.
In the absence of any standard instructions for structuring the Standard Bidding Documents in the
NWFP Procurement Rules 2003, the procuring entities of the Health Department of Khyber
Pakhtunkhwa have, over the time, grouped together all the above mentioned indicators of the Pre-
34
Qualification documents and General Principles for bid evaluation, to evolve a document to be used
simultaneously to serve the purpose of three documents i.e., (a) the Tender Inviting Notice (b) the
bidding document for purchasing of goods and (c) the contract template for contractual privity. Thus,
in a way, Rule 11, Rule 12 & the said General Principles (Appendix to the NWFP Procurement
Rules 2003) together establish the minimum content of the tender documents and require that
content is relevant and sufficient for bidders to be able to respond to the clients requirements.
Until recently, in Khyber Pakhtunkhwa, the Directorate General Health Services, the Autonomous
Medical Institutions and the Vertical Programs have been using this evolved 3-in-1 bidding
document for purchasing both pharmaceutical products and bio-medical equipment using Single
Stage Single Envelop procedure. However, the Health Department Khyber Pakhtunkhwa conducted
procurement of Bio-Medical equipment in April 2012 with the help of a more detailed version of
Bidding Documents for adopting Two Envelop Tendering procedure.
In August 2012, the said Bidding Documents were thoroughly revised and standardized in
accordance with the FIDIC templates for procurement of goods and fine-tuned to procurement of
pharmaceutical products i.e., drugs, medicines and biological vaccines as per Rule 40 of the NWFP
Procurement of Works, Goods & Services Rules 2003 under Two Envelop Single Stage Bidding
process. Similarly, Vertical Program relating to the Maternal Neo-natal and Child Health (MNCH)
Khyber Pakhtunkhwa has also taken its procurement initiative for the acquisition of Community Mid-
Wife (CMW) Kits for its 25 health districts through the above said revised Standard Bidding
Documents (SBDs) in September 2012 under the said Rules.
These Standard Bidding Documents (SBDs) for procurement of Drugs and Surgical Disposables, for
the first time in the procurement stream of the Health Department Khyber Pakhtunkhwa, offer a
proper documentation structured on international contracting standards displaying two sections, one
for fixed conditions and the other for variable conditions of contract. The Part-I of the Standard
Bidding Documents relating to the fixed conditions constitute Instructions To Bidders (ITB) and
General Conditions of Contract (GCC). Part-II of the said Documents constitute Invitation For Bids
(IFB), Bid Data Sheet (BDS) reflecting any changes in reference to the Instructions To Bidders in
Part-I of the SBDs, Special Conditions of Contract (SCC) reflecting any changes in reference to the
General Conditions of Contract (GCC) in Part-I of the SBDs, Technical & Financial Evaluation
Criteria with particular reference to acquisition of pharmaceutical products and bio-medical goods,
Inspection Checklist / Performa for Pre-Qualification of Pharmaceutical manufacturing units pre-
qualified by DGHS Khyber Pakhtunkhwa, Specialized/Biological Drugs List & Drug Formulary
approved by the DGHS, Specifications & Rate Table, Supply Schedules, Technical Specifications
for general medicines, biological drugs & bio-medical equipment and ancillary Services, Standard
Bid Forms and finally the list of eligible countries whose bidders can participate in the bidding
process for supplying goods to DGHS Khyber Pakhtunkhwa.
The Standard Bidding Documents recently adopted by the Directorate General Health Services
Khyber Pakhtunkhwa for procurement of pharmaceutical goods including drugs and surgical
disposables contain sufficient information to enable the submission of responsive bids and to
establish the basis for a transparent evaluation and award process. Specifications relating to
biological drugs and general medicines included as an annexure in the Standard Bidding
35
Documents through the approved Drug Formulary seem to be generic and refer to international
standards associated with the World Health Organization (WHO) and US Food & Drug
Administration (FDA) for their assessment in the Technical Evaluation Criteria.
Though a methodology to determine gradation of pharmaceutical raw material source with respect
to the quality for product efficacy (i.e., excellent, good or satisfactory grade etc) has not yet made its
way into the Technical Evaluation Criteria in the recently adopted Standard Bidding Documents
mentioned above for the want of finalization of the draft policy on raw material source pricing and
quality pending for approval by the Federal Government, other technical criteria have been
incorporated to ensure maximum possible efficacy of the product. The said criteria include past
performance of the bidder through Purchase Orders from major health institutions, market
experience of the bidder and percentage of market share of a biological drug, credibility of the
bidder through Good Manufacturing Practices (GMP) certification and drug manufacturing standards
set by the World Health Organization (WHO), US Federal Drug Agency (FDA), European
Communitys Directive 93/42/EEC (Annex-II, Article 3) and Pakistan National Accreditatation
Council (PNAC) etc.
To ensure drug efficacy, the technical expertise of the staff of the bidder in the areas of plant
management, quality control and quality assurance with an edge given to atleast five years
pprofessional experience in pharmaceutical production, has been given due weightage with
particular focus on handling and maintenance experience of cold chain for transportation of
temperature-sensitive biological/specialized drugs from manufacturing facility situated locally or
abroad to the end-user. Raw Material Stability certificates and Production Quality Control equipment
calibration certificates by third party calibrators for the manufacturing firms have also been
considered for including them in the Technical Evaluation Criteria.
It has been ensured in the Technical Evaluation Criteria that even if the source gradation is at the
moment not possible due to pending policy formulation at Federal level, atleast the source of
pharmaceutical raw material or of a medicine supplied in a finished form against a quoted item
should be ascertained / verified through import documentation e.g., product related Customs Goods
Declaration, Bill of Lading or Commercial Invoice showing the country of origin accompanied by a
bio-assay or an analysis for the said raw material / finished product in the form of an Analytical
Certificate or Quality Assurance Certificate duly issued by the concerned Drug Registration
Authority (DRA) of the country from where imported, e.g., the current GMP (cGMP) certificates
issued by renowned DRAs like USFDA, European Medicines Association (EMA), Medicines &
Healthcare Products Regulatory Agency (MHRA) UK, Therapeutic Goods Administration (TGA)
Australia, Pharmaceutical Medical Agency (PHARMAC) New Zealand, Pharmaceutical & Medical
Devices Agency (PMDA) Japan, Swiss Agency For therapeutic drugs (Swiss-medic) Switzerland,
Health Canada, Health Sciences Authority (HAS) Singapore and National Administration of Drugs &
the Food & Medical Technology (ANMAT) Argentina etc., all having recognized international
standards for full quality assurance system for pharmaceutical products. In the case of recently
drafted Standard Bidding Documents for procurement of cancer medicines for Begum Nusrat Bhutto
Oncology Services in Khyber Pakhtunkhwa for 2012-13 by Hayatabad Medical Complex, IRNUM,
INOR and Abbottabad Teaching Hospitals Oncology Department, the Technical Evaluation criteria
has been introduced which contains highly-scored raw-materials sources for anti-cancer medicines
36
certified from Category-A DRAs consisting of the above mentioned DRAs, and those lesser-scored
certified by Category-B DRAs of China, India, Pakistan, Brazil, Egypt, Korea, Malaysia and Jordon
etc. Various Pre-Qualification Criteria have also been omitted in view of the Post-Qualification in the
said SBDs.
With an estimated outlay of Rs. 629 million allocated for procurement of drugs out of the total Rs 1.2
billion for health sector related procurements for the current fiscal year in Khyber Pakhtunkhwa, the
procurement of medicines in general and biological drugs in particular attained a significant place on
the priority list of the Health Department. The need for specialized Bidding Documents customized
for procuring the said pharmaceutical products and related bio-medical equipment was therefore
direly felt. Directorate General Health Services made substantial efforts towards achieving the said
objective in collaboration with TRF Khyber Pakhtunkhwa.
It was therefore during the re-design and introduction of the revised Standard Bidding Documents
for procurement of pharmaceutical products in compliance with the international contracting
templates and health related acquisition Guidelines of the World Bank, WHO and USFDA that the
Directorate General Health Services has actively demonstrated its sensitivity towards achieving
highest grade for biological drugs keeping in view their life saving impact and assurance against
disease relapse.
Special provisions in the Technical Evaluation Criteria of the said Bidding Documents, in
consultation with pharmaceutical sector specialists in the Health Department, have thus been
introduced for the first time in the form of mandatory bio-equivalence studies to be provided by the
suppliers or manufacturers for anti-Tubercular products (Anti-TB Vaccines), requirement of pre-
qualification of suppliers by the WHO for EPI vaccines (BCG, Measles, Tetanus and Pentavalent:
DPT-HepB-Hib), mandatory Sustained Viral Response (SVR) studies containing clinical trials
performed with reference standards on efficacy of Hepatitis C vaccine (consisting of conventional
and Pegylated Interferon therapy) and having their clinical data demonstrating published efficacy &
disease relapse period in atleast one indexed journal of international repute with considerable
readership impact. Unfortunately however, the Surgical Disposables, earlier procured by Govt-MCC,
DGHS in the last many years and intended to be acquired through the revised Standard Bidding
Documents, have been handed over to the AMIs like Lady Reading Hospital Peshawar to use the
obsolete three page bidding document for their procurement of non-drug surgical disposables in the
current financial year through administrative approval from Health Secretariat, thus still leaving
some effort in harmonizing the procurement business practices based on the revised Standard
Bidding Documents.
Rule 33 of the NWFP Procurement Rules 2003 concerning description of goods, construction or
services ensures generic and unbiased technical specifications to be included in the tender
documents. The Bidding Documents designed in April 2012 for procurement of bio-medical
equipment and the revised Standard Bidding Documents for procurement of pharmaceutical
products and CMW kits for Govt-MCC, DGHS and MNCH Program respectively contain generic and
neutral technical specifications of goods in compliance to the above said Rule. The Technical
Criteria for the Bio-medical equipment contain product conformance certifications standards like US
Food and Drug Administration (FDA) 510K, European Community (CE) MDD or Japan Industrial
37
Standards (JIS alongwith the product performance certifications from authentic certifying bodies like
Association for the Advancement of Medical Instrumentation (AAMI), International Certification
Commission (ICC) and the United States Certification Commission (USCC) etc. Further, the
participating firms should have their technical resource persons to have expertise based on bio-
medical equipment oriented CCE, CBET, CRES, CLES Certifications etc.
Rule 33(2)(a) further requires recognition of standards which are equivalent when neutral
specifications are not available.
Scoring Criteria Score
The legal framework meets the following conditions:
3
(a) Establishes the minimum content of the tender documents and
requires that content is relevant and sufficient for tenderers to be able
to respond to the requirement.
(b) Requires the use of neutral specifications citing international standards
when possible.
(c) Requires recognition of standards which are equivalent when neutral
specifications are not available.
The legal framework substantially meets the conditions of (a) plus one of the
remaining conditions.
2
The legal framework meets the conditions of (a).
1
The content of the bidding documents is totally or largely left at the discretion
of the procuring entity.
0
Sub-indicator 1(f) Tender evaluation and award criteria
This sub indicator assesses:
a) the quality and sufficiency of the legal framework provisions in respect to the objectivity and
transparency of the evaluation process; and,
b) the degree of confidentiality kept during the process to minimize the risk of undue influences
or abuse.
Rules 23 to 29 in Chapter IV (Tender Evaluation) of NWFP Procurement Rules 2003 indicate
requirements for providing pre-disclosed and objective criteria essential for efficiency, fairness and
transparency in the evaluation of tenders. General Principles for Evaluation of Application for the
Pre-Qualification & Technical Bids for Post-Qualification (Appendix to NWFP Procurement Rules
2003) give three different stages for evaluation of bids or proposals. In Stage-I these make tender
evaluation less subjective by providing screening criteria for preliminary scrutiny, indicators of
compliance, eligibility and responsiveness. The General Principles render the said indicators
quantifiable by making pre-qualification criteria (for pharmaceutical firms and suppliers of bio-
medical equipment) an integral part of the tender evaluation for a detailed technical evaluation.
38
The General Principles further attach value to the legal status of the bidders by defining commercial
acceptability, public and private sector status for participating entities and probable joint ventures for
assessing the corporate relationship of the bidder. In Stage-II, the Principles extensively comment
on the financial and technical capabilities and relevant experience (including past experience) of the
bidders and further define the major features, groups of factors and distribution of points of the
scoring criteria that recognizes several factors collectively to give the client confidence about
whether a criterion has been met in terms of technical compliance by and commercial soundness of
the bidder.
After having defined the evaluation criteria, the General Principles, in Stage-III, opt for factors
constituting additional information for final determination of qualified bidders. The revised Standard
Bidding Documents being used by the DGHS and Vertical Programs in Khyber Pakhtunkhwa duly
incorporate the above stated features and factors influencing the evaluation criteria in the light of the
said Rules and General Principles to offer an objective assessment of the capabilities of the
bidders.
Rule 28 of the NWFP Procurement Rules 2003 gives indicators for determining the lowest
evaluated responsive bidder. The same has been adopted by the DGHS Khyber Pakhtunkhwa for
selecting the lowest unit rates in centralized contracting for the pharmaceutical products in Govt-
MCC and lowest item rates for the bio-medical equipment of all those suppliers/manufacturers in the
Procurement Cell at DGHS who have complied with the technical & commercial evaluation criteria
designed on lowest price. So far the merit point evaluation technique for choosing the best value for
money has not been applied in the above stated revised Standard Bidding Documents for the year
2012-13. Merit Point technique assigns significant marks to the non-price factors, thereby tilting the
balance of evaluation in favour of quality rather than price. It is hoped that future bidding documents
of the DGHS for the year 2013-14 may incorporate the merit point evaluation mechanism for bid
evaluation as Rule 24 of the NWFP Procurement Rules 2003 allows tender evaluation to be in
accordance with the evaluation criteria even if based on Merit Point Evaluation Method instead of
Lowest Price Method.
Confidentiality and regulated communications with the bidders during the evaluation period have
been duly advised under Rule 26 of the NWFP Procurement Rules 2003 to stop any abuse and
undue interference in the process. Rule 25 binds the evaluation committee to complete evaluations
within 15 days of the bid opening and allowing a further extension of ten days. However,
procurement record of the DGHS shows that the earlier evaluations got completed more than a
month or so though administrative approvals for extensions were not usually taken. Generally the
prices/quotations become a public property after opening of financial bids. However, it has been
observed that the Directorate General Health Services keeps them confidential till the
announcement of the lowest selected rates for Govt-MCC by mostly retaining the members
nominated in the preliminary scrutiny committees for initial profiling of the technical bids in the
subsequent committees like Comparative Statement Committee and working with a very limited
number of highly trusted Key Punch Operators/steno typists proficient in typing skills for entering the
voluminous price data against thousands of selected items for Govt-MCC. The inherent risk in such
business practices has the potential to amplify the bias of a committee member thereby vitiating or
39
jeopardizing the integrity of the procurement cycle. The high impact of this risk leads to a potential
conflict of interest.
Though Rule 42 binds the client to promptly inform the selected bidder, there is no provision in the
NWFP Procurement Rules 2003 for disclosing the information related to the evaluation process and
results to the participating or interested parties after the evaluation is complete. The Health
Department has therefore no proprietary mechanism for such disclosure of information except for
displaying in the end the final results of contract award on the website owned by the EPI Vertical
Program. The SBDs for procurement of Anti-cancer medicines have been recently posted as of
31.12.2012 on the Health Departments website in Tenders section.
Scoring Criteria Score
The legal framework mandates that:
3 (a)
The evaluation criteria are relevant to the decision, and precisely
specified in advance in the tender documents so that the award
decision is made solely on the basis of the criteria stated in the tender
documents.
(b) Criteria not evaluated in monetary terms are evaluated on a pass/fail
basis to the extent possible.
(c) The evaluation of proposals for consulting services gives adequate
importance to the quality and regulates how price and quality are
considered.
(d) During the evaluation period, information relating to the examination,
clarification and evaluation of tenders is not disclosed to the
participants or to others not involved officially in the evaluation process;
The legal framework covers the conditions of (a) and (b) plus one of the
remaining conditions.
2
The legal frame work covers (a) but does not fully cover the other conditions. 1
The legal framework does not adequately address any of the conditions (a)
through (d) above
0
Sub-indicator 1(g) Submission, receipt and opening of tenders
This sub indicator assesses how the legal framework regulates the process of reception of tenders
and tender opening.
Rule 18 of the NWFP Procurement Rules 2003 provides for public opening of tenders for proper
receipt and safe custody of the bids as a means of increasing transparency to an open tendering
exercise. The said Rule further provides for extension in bid submission time where certain changes
in the bidding documents resulting due to the deliberations between the Procuring Entity and the
prospective bidders during the Pre-Bid Meetings need to be communicated to the bidders and
reasonable time to be given to them through extension in bid submission time for reflecting their
thoughtful response by incorporating it in the bidding documents before bid submission. This
practice has not been strictly followed by the Directorate General of Health Services with respect to
40
the acquisition activity for pharmaceutical products despite requests from the prospective bidders;
hence receipt of various bids with limited and inadequate response to the changes carried out
during the Pre-Bid meetings. As the said Rule provides no specific time for any time extension in
this regard, a five to seven days period after proper communication of the changes in the bidding
documents to the bidders seems to be adequate to deal with such an issue.
Rule 19 of the NWFP Procurement Rules 2003 explains the procedure for submission of sealed
bids to the Procuring Entity. DGHS, AMIs and Vertical Programs have constituted Bid opening
committees in this regard where minutes of meeting, the names and addresses of the bidders and
the tender prices (and any withdrawals or modifications to tenders duly submitted) alongwith status
of responsiveness are read aloud and recorded. Records are retained and available for review and
audit purposes. Opening of technical bids is done immediately after the deadline for submission of
tenders which diminishes the possibility of loss or alteration of proposals or submissions.
Rule 20 (1) provides for minimum of thirty days time for submission of tenders. The current practice
in the Health Department relating to the said legal provision deviates on account of Rule 20 (2)
which allows reduction in the time to any number of days as authorized by the Head of the
Procuring Entity in the wake of any lapse of allocated funds for the procurement activity under
consideration or an exigency. Such practices not only reflect badly on the planning side of the
Department but may raise questions on the transparency of the open competitive process which
has been made restrictive by curtailing the mandatory participation time thereby defeating the very
purpose of providing adequate time for bid preparation and submission considered as one of the
international best practices. Rule 20 (2) may therefore be considered as a defective legal provision
which has the inherent characteristic for abuse of procurement process.
The Directorate General Health Services currently controls the majority of contracting actions of the
AMIs and Vertical Programs in the Health Department despite allocation of 40% of the procurement
to the AMIs regarding procurement of pharmaceutical products after devolution of powers to the
provinces whereby autonomy to the procuring entities associated with the Health Department
Khyber Pakhtunkhwa was granted. The AMIs have been administratively directed by the Health
Secretariat to get only those medicines procured under the allotted 40% share which have not been
included in the list of medicines procured through Govt-MCC, DGHS in medical emergencies or
otherwise. Reduction in bid submission time for all such contracting activities associated with these
entities is being carried frequently in consonance with the similar practice prevalent in the DGHS.
Rule 21 provides for public opening of financial bids wherein bidders or their representatives must
be permitted to attend. The Health Department complies with the said Rule and proper record of
public opening of the financial bids is maintained.
Rule 17 (2) provides for the Pre-Bid meeting wherein opportunity to the prospective bidders is given
through instructions by the Department to bring clarity on how to submit responsive bids and to
minimize the prospects of rejection of otherwise compliant bids by inadvertent mistakes. The
revised Standard Bidding Documents give elaborate Instructions To Bidders in this regard.
Guidelines on conducting Pre-Bid Meetings have recently been intimated to the procurement
officials of the Health Department by the TRF.
41
Scoring Criteria Score
The legal framework provides for the following conditions:
3 (a) Public opening of tenders in a defined and regulated proceeding
immediately following the closing date for bid submission.
(b) Records of proceedings for bid openings are retained and available for
review.
(c) Security and confidentiality of bids is maintained prior to bid opening
and disclosure of specific sensitive information during debriefing is
prohibited.
(d) The modality of submitting tenders and receipt by the government is
well defined to avoid unnecessary rejection of tenders.
The legal framework provides for (a) and (b) plus one of the remaining
conditions.
2
The legal framework provides for (a) plus one of the remaining conditions. 1
There is no requirement in the legal framework for public opening of tenders. 0
Sub-indicator 1(h) Complaints
The purpose of this indicator is to assess whether the legal framework establishes;
a) the right to review;
b) the matters that are subject to review;
c) the timeframe for such reviews; and,
d) the different steps in the review process.
Rule 43 of the NWFP Procurement Rules 2003 offers opportunity to an aggrieved bidder to file an
application for review of the decision/order of the Procuring Entity awarding a contract provided the
contract has not already entered into force. The review application should clearly mention the date
of acceptance of tenders, material defects and non-observance of rules in the contract award letter.
However, the reason assigned for review under the said Rule seems restrictive as it only addresses
a situation whereby a bid has been accepted by an unauthorized procuring entity. In the current
scenario of acceptance of bids in the DGHS and its allied procuring entities, proper Purchase
Committees have been formed and notified which have the sole authority to accept or reject a bid.
The opportunity for review under Rule 43 therefore seems irrelevant in this regard. Confidence in a
procurement system is a powerful incentive to competition. A fundamental part of this is the
establishment of the right to review procurement decisions by an efficient and functionally
independent process which should include opportunity to protest against exclusion of a
pharmaceutical firm/bio-medical equipment supplier on account of any pre-qualification or post-
qualification during bid evaluation conducted by the Department which in Firms view, has caused
grievance. Further to it, the Rule does not offer any protest against unlawful exclusion of a
technically qualified bidder by the Procuring Entity through abuse of Rule 32 of the NWFP
Procurement Rules 2003 who remained as the only one left after the detailed technical evaluation.
42
Rule 43 stated above also does not provide any opportunity to a bidder who feels aggrieved on
account of a biased application of technical or commercial evaluation criteria by the Technical
Evaluation Committee.
The first review exists at the level of the Secretary Health who considering the nature and gravity of
the complaint, either reviews the decision of the Procuring Entity himself or immediately creates a
committee to review the same. The review committee, usually headed by Special Secretary Health
or any Technical member, mostly comprises members who are not part of the referenced
purchasing process, and is fully authorized to review the Procuring Entitys decision. This attempts
to assure the independence of the complaint review body and to eliminate any conflict of interest.
However, the quasi-judicial review stated above is not independent of the procuring agency having
direct interest in the procurement process under reference and with no counter-part appellate
review in the form of any Health Appellate Tribunal in sight. This infirmity currently present in the
system often tempts the aggrieved bidders to directly seek remedy at forums like Provincial
Ombudsman, Provincial NAB or Honourable Peshawar High Court etc. or any other forum
independent of the procuring agency (but not defined in the NWFP Procurement Rules 2003)
without resorting to office of the Secretary Health as the first appropriate forum for a quasi-
judicial/administrative review. Hence, a foray of complaints and litigations at inappropriate forums
against the decisions of the Health Department. The proposed provincial appellate authority under
Section-9 or the functional Federal Appellate Board under Section-9A of the Drug Act 1976 deal
with drug registration, licensing and supplier disqualification issues etc. and do not cover
procurement related complaints.
Scoring Criteria Score
The legal framework provides for the following conditions:
3
(a) The right to review for participants in a procurement process.
(b) Provisions to respond to a request for review at the procuring agency
level with administrative review by another body independent from the
procuring agency that has the authority to grant remedies and includes
the right for judicial review.
(c) Establishes the matters that are subject to review.
(d) Establishes timeframes for issuance of decisions by the procuring
agency and the administrative review body.
The legal framework provides for (a) and (b) plus one of the remaining
conditions.
2
The legal framework provides for (a) plus one of the remaining conditions. 1
The right for review of the proper application of the procurement process is not
provided in the legal framework.
0
43
Indicator 2. Existence of Implementing Regulations and Documentation.
This indicator verifies the existence, availability and quality of implementing regulations, operational
procedures, handbooks, model tender documentation, and standard conditions of contract. Ideally
the higher level legislation provides the framework of principles and policies that govern public
procurement. Lower level regulations and more detailed instruments supplement the law, make it
operational, and indicate how to apply the law to specific circumstances. This indicator consists of
six sub-indicators (a-f).
Sub-indicator 2(a) Implementing regulation that provide defined processes and procedures
not included in higher-level legislation
This sub indicator aims at verifying the existence, clarity, accessibility and comprehensiveness of
regulations to the law that further detail and clarify its application.
The NWFP Procurement of Works, Goods & Consulting Services Ordinance 2002 & NWFP
Procurement of Goods, Works & Services Rules 2003 currently governing the procurements at the
provincial level in the Health Department constitute higher level legislation for providing the legal
framework for the same in a variety of applications. The NWFP Procurement of Goods, Works &
Services Rules 2003 do not get regularly updated as the responsibility for their updation by the
concerned entity is not clearly defined anywhere.
The recently revised Standard Bidding Documents created in view of procurement of
pharmaceutical products and bio-medical equipment for Directorate General Health Services
constitute the implementing regulations that provide defined processes and procedures not included
in the higher-level legislation with respect to Technical & Commercial criteria. However, the
technical evaluation is currently not based on Merit Point scoring as the same takes into account the
impact of non-price factors alongwith minimum price to get the combined evaluation score highest
of which gets the contract.
Scoring Criteria Score
There are regulations that supplement and detail the provisions of the
procurement law that meet the following requirements:
3
(a) They are clear, comprehensive and consolidated as a set of regulations
available in a single and accessible place.
(b) They are updated regularly.
(c) The responsibility for maintenance is defined.
The regulations meet the conditions of (a) plus one of the remaining conditions. 2
The regulations exist but there is no regular updating, the responsibility for
updating is not clearly defined or there are many important omissions in the
regulations or inconsistencies with the law.
1
There are no regulations or the existing ones do not meet substantially any of
the requirements listed above.
0
44
Sub-indicator 2(b) Model tender documents for goods, works, and services
Model documents of good quality promote competition and increases confidence in the system.
Potential contractors or suppliers are more willing to participate when they are familiar with the
documents and their interpretation.
The recently introduced revised Standard Bidding Documents for pharmaceutical products are
based on FIDIC templates customized to health sector requirements and contain the requisite
clauses which can be incorporated into contracts to enable the bidders to value the cost and risk of
mandatory clauses when performing a contract for the government. In consultation with
pharmaceutical sector specialists at the Directorate General Health Services, TRF has standardized
the Bidding Documents for medicines and bio-medical equipment in the light of international best
practices based on performance benchmarks of World Health Organization (WHO), US Federal
Drug Administration (FDA), EU Directive 93/42/EEC and Pakistan National Accreditation Council
(PNAC) etc. for the health sector.
Similar Standard Bidding Documents are being used for Vertical Programs like MNCH & EPI in the
Health Department Khyber Pakhtunkhwa for procurement of CMW Kits & general goods
respectively except for procurement of non-drug surgical disposables for Lady Reading Hospital
where an outdated three page bidding document has been used despite the availability of revised
Standard Bidding Documents. This reflects the vague policy of the Health Department on
mandatory usage of Standard Bidding Documents for ongoing procurements and demonstrates
distortion in adopting the standardized business practices.
The Health Sector Reforms Unit (HSRU) Khyber Pakhtunkhwa - Health Departments planning
interface for carrying out the World Bank funded project for outsourcing of health sector
management services delivery in six selected districts of Khyber Pakhtunkhwa, is utilizing World
Banks Standard Bidding Documents based on Cost & Quality based Selection (CQS) method.
Scoring Criteria Score
(a) There are model invitation and tender documents provided for use for a
wide range of goods, works and services procured by government
agencies;
3
(b) There is a standard and mandatory set of clauses or templates that are
reflective of the legal framework, for use in documents prepared for
competitive tendering.
(c) The documents are kept up to date with responsibility for preparation
and updating clearly assigned.
Model documents and a minimum set of clauses or templates are available, but
the use of such documents is not mandatory or regulated. The documents are
not updated regularly.
2
Model documents are not available, but a set of mandatory clauses is
established for inclusion in tender documents.
1
There are no model documents and the procuring entities develop
their own documents for with little or no guidance.
0
45
Sub-indicator 2(c) Procedures for pre-qualification
This sub-indicator covers the existence of procedures for pre-qualification of participants in a
particular procurement.
Rule 7 of the NWFP Procurement Rules 2003, discussed earlier at Sub-indicator 1(b) for
Procurement Methods, makes open competitive tendering the default method of procurement in
Khyber Pakhtunkhwa Province and attracts pre- or post-qualification of bidders as is being done at
the Directorate General Health Services. Till now pre-qualification of manufacturers and suppliers of
bio-medical equipment or pharmaceutical goods has been initiated as a separate exercise by the
DGHS usually conducted annually well before initiation of any scheduled procurement activity by
the Health Department.
For the pre-qualification of firms manufacturing or supplying different commodities like bio-medical
equipment, bedding clothing, medical gases, chemicals, kits, reagents, disinfectants, insecticides,
medical/office furniture, vehicle repair & related spare parts etc., the Department requires through a
detailed Inspection Checklist a firms corporate profile, valid registration from Registrar Companies
showing manufacturing / supplier status; or any valid agency agreement between importer &
manufacturer duly attested by the embassy of the country of origin in Pakistan or of Pakistani
embassy in that country. The Department also ensures that the firm is registered with FBR for
payment of Income Tax and Sales Tax and gets audited by a chartered accountant firm. Firms
annual import statement and sales record are also taken into account.
The pre-qualification criteria for drug manufacturers or suppliers, compared to ones for bio-medical
equipment, is based on somewhat more complex requirements geared at determining the
pharmaceutical product efficacy achievable only through strict implementation of a series of
complex Good Manufacturing Practices (GMP) at the local and foreign business premises alike and
is verified through a significantly detailed Inspection Checklist containing firms corporate profile,
type of activity being carried out by the company i.e., formulation of Active Pharmaceutical
Ingredients (API) and Non-Active Pharmaceutical Ingredients (excepients), repacking or basic
manufacturing, annual sales and import record, GMP compliance certificate and / or any other
certification from USFDA, EMA, WHO, ISO or PNAC etc. and related audit report, detail of technical
personnel in plant, production quality control and formulation development sections, manufacturing
information including usage of pharmaceutical raw materials, dosage form and production capacity,
SOPs regarding requisite operations in syrup, tablets, capsules, dry powder, ointment and liquid
injectable manufacturing sections and lastly operations regarding the related inventory
management, warehousing and supply chain of pharmaceutical products.
The GMP Certification is therefore achieved through regular inspections by a typical Pre-
Qualification Committee designated for a specific region and consisting of members from among
Health Department designations like Additional Secretary (Dev) Health KP / Director General Health
Services KP / Medical Superintendent AMI Peshawar / Director Admn, DGHS KP, Professor of Surgery AMI
Peshawar, Deputy Secretary (Budget), Health Department, Chief Drug Inspector Peshawar, Deputy Director
Pre-Qualifications, Pharmacist Govt-MCC DGHS, Drug Inspector, EDO (Health) Peshawar or any other as
designated. The said Pre-Qualification Committee submits Inspection Report to the Chairman Technical
46
& Evaluation Committee DGHS within three days of inspection for evaluation of firms for pre-
qualification.
Below is the typical annual calendar of activities regarding pre-qualification of firms for Govt-MCC,
DGHS, Khyber Pakhtunkhwa initiated from the office of Section Officer (Drugs), Health Department:
S.No Pre-Qualification Activity Date (each year)
1 Advertisement for application for pre-qualification 1
st
January
2 Last date for submission of application 24
th
January
3 Compilation of activities 30
th
January
4 Assessment of Documents attached with applications 20
th
February
5 Visit of business premises by Pre-Qualification Inspection
Teams & submission of their reports
Upto 25
th
March
6 Compilation of list of Pre-Qualified firms and its submission to
T&E Committee for verification & approval
Upto 30
th
March
7 Circulation of approved list of pre-qualified firms 1
st
week of April
With the introduction of the revised Standard Bidding Documents for procurement of drugs for Govt-
MCC in September 2012, criteria or benchmarks set for the Pre-qualification of manufacturers and
suppliers of pharmaceutical products have been incorporated therein to combine them with the
Technical Evaluation Criteria. However, keeping in view the complex nature of procurement of
general medicines/biological drugs, pre-qualification as a separate process has been retained by
the Health Department as a policy decision todate to make the said procurement more efficient by
limiting the number of participants and ensuring only qualified participants to be included thereby
saving departmental resources consumed in bid evaluation. This may help in excluding certain pre-
qualification aspects to be removed from the Technical Evaluation Criteria and introducing post-
qualification aspects instead to save repetition of effort and evaluation time.
Scoring Criteria Score
Procedures exist that define pre-qualification which:
(a) Provide for limitations on the content of pre-qualification criteria that are
based on the needs of the specific procurement.
3
(b) Specify the use of pass/fail for application of qualification criteria.
(c) Provide guidance on when to apply a pre-qualification procedure.
Procedures exist that cover (a) plus one of the remaining conditions. 2
Procedures exist that cover (a). 1
Procedures for the application of pre-qualification procedures do not exist. 0
47
Sub-indicator 2(d) Procedures suitable for contracting for services or other requirements
in which technical capacity is a key criterion
NWFP Procurement of Goods, Works and Services Rules 2003, despite the name given to them do
not include any regulations on hiring of consultancy services. This may be attributable to the time of
promulgation of the said Rules when hardly any regulations existed in Pakistan on services
contracting. Rule 40 of the above said Rules offers a Two Envelop Tendering procedure which
relates to procurement of construction work or supply and installation of goods, equipment or
tenders where post-qualification procedures is being followed. Though the technical capacity and
quality have been considered key criteria for detailed evaluation in the General Principles for
Evaluation of Applications for Pre-Qualification & Technical Bids for Post-Qualification (Appendix to
Rules), non-existence of any consultancy regulations make it irrelevant for the same. Directorate
General Health Services or its subsidiaries including Vertical Programs, Health Projects like AIDS
Control and AMIs therefore do not have any existing regulations for consultancy services. Any
Technical Assistance acquired by them is governed under the Donor Guidelines whose assistance
is extended to them in this regard.
To address this deficiency, the Provincial Government has notified through Governor KP an Inter-
Departmental Consultant Selection Committee (IDCSC) for selection of design and engineering
consultants for the government departments. The Committee is composed of line members from
Finance Division, Planning & Development Division, C&W Department and functional members
from the department for whom the consultant is being hired. In the light of certain administrative
instructions and SOPs, the IDCSC develops specific Preliminary Scope Statement, Project
Appraisal Document, TORs and RFP Documents for the intended activity.
Health Sector Reforms Unit (HSRU), Health Secretariat Khyber Pakhtunkhwa, on the other hand,
has recently adopted World Banks standard bidding templates, which have been customized with
the help of TRF for developing Request For Proposal (RFP) Documents to acquire Management
Consultancy services for revitalizing and strengthening the health service delivery in six crises
affected districts of Khyber Pakhtunkhwa, namely Battagram, Buner, Dera Ismail Khan, Dir Lower,
Kohistan and Tor Ghar under Public Private Partnership. The said project is being funded by the
Multi Donor Trust Fund (MDTF) through World Bank and therefore the World Bank Guidelines for
Hiring of Consultancy Services, revised in 2011, are being followed by the HSRU. The said
Guidelines adequately contain the methodology of a scored evaluation of technical qualification
against stated criteria in order to select the highest qualified proposal by combining the relative
weights allocated to technical capacity and price. Such donor funded scenarios derive their authority
from Rule 4(3) of the NWFP Procurement Rules 2003 whereby donor Guidelines would prevail over
local laws but the condition of Rule 4(3) for observing the lower financial limit of Rs 40,000 for
ascertaining the mode of procurement in the donor funded projects is not being followed. There
seems little coordination between the Health Department & the IDCSC for any probable selection of
management or design consultant for the HSRU for undertaking responsibilities of reforms of health
sector due to lack of ownership of the said restructuring component by the Directorate General
Health Services, Khyber Pakhtunkhwa.
48
Scoring Criteria Score
The legal framework and its implementing regulations provide for the following:
(a) Conditions under which selection based exclusively on technical capacity
is appropriate and when price and quality considerations are appropriate.
3
(b) Clear procedures and methodologies for assessment of technical capacity
and for combining price and technical capacity under different
circumstances.
Implementing regulations meet a) above but leave b) to the discretion of the
procuring entity.
2
Implementing regulations leave the possibility of use of technical capacity in
selection but neither the law nor the regulations elaborate on the procedure.
1
Neither the law nor implementing regulations cover this procedure. 0
Sub-indicator 2(e) Users guide or manual for contracting entities
This sub-indicator covers the existence of a users guide or manual for contracting entities.
Neither the NWFP Procurement Rules 2003 nor the Health Department offer any User Guide or
Procurement Manual which could act as an implementation tool to help provide Departments
procurement officials with information that incorporates the law, policy and procedures for turning
policy into practice. Procedures for registration and pre-qualification of firms supplying bio-medical
equipment and pharmaceutical products are in place but have not been translated into any manual
so far. With the creation of a centralized Procurement Cell at DGHS level, it is expected that the
Health Department in consultation with TRF may develop a Procurement Manual or more precisely
a Health Sector Supplement to be read in conjunction with public procurement rules for
procurement of pharmaceutical products and bio-medical equipment to create consistency of their
application within the government procurement system. Development of Technical Evaluation
Guidelines for pharmaceutical products and bio-medical equipment are underway by TRF which are
expected to find their way into the said proposed Supplement containing a calendar of monthly
customized training activities of the procurement officials and to provide an easy desk reference for
users.
Scoring Criteria Score
(a) There is a unique procurement manual detailing all procedures for the
correct administration of procurement regulations and laws.
3
(b) The manual is updated regularly;
(c) The responsibility for maintenance of the manual is clearly established.
There is no unique manual but there is an obligation for the procuring agencies
to have one that meets conditions (b) and (c).
2
There is no manual and no obligation to have one but many procurement
agencies have an internal manual for administration of procurement.
1
There is no manual or requirement to have one. 0
49
Sub-indicator 2(f) General Conditions of Contracts (GCC) for public sector contracts
covering goods, works and services consistent with national requirements and, when
applicable, international requirements
This sub-indicator deals with General Conditions of Contracts that set forth the basic provisions
which will be included in a contract with the government.
The bidding documents used earlier by the Directorate General Health Services and its subsidiaries
did not have any standard General Conditions of Contract but had a three-page contract document
that simultaneously served as an Invitation For Bids, a Contract Template for establishing privity
and Terms & Conditions. The new Standard Bidding Documents recently adopted by the Health
Department for procurement of pharmaceutical products contain the consistent and mandatory
General Conditions of Contract (GCC) based on FIDIC templates duly recognized World-wide. Any
changes in the GCC are thereby brought about in the Special Conditions of Contract (SCC) to
reflect the commercial codes that deal with contracts between parties for performance. The GCC
and resultant SCC therefore duly provide information that enables participants to understand the
allocation of risk between parties to a contract as well as other obligations including impact on price
that the signatories to the contract will incur. Exception to this is the procurement of non-drug
Surgical Disposables still being done on Single Envelop Single Stage by the AMIs with the above
stated three-page primeval contract document, abandoned by the DGHS itself.
Scoring Criteria Score
Both of the following apply:
(a) There are GCC for the most common types of contracts and their use is
mandatory.
3
(b) The content of the GCC is generally consistent with internationally
accepted practice.
There are GCC for the most common types of contracts, consistent with
international practice, but their use is not mandatory.
2
There are GCC for the most common types of contracts but they do not conform
to internationally accepted practice and their use is not mandatory.
1
There are no GCC and individual agencies use the form of contract of their
choice.
0
5.7 Pillar-II: Institutional Framework & Management Capacity
Pillar-II looks at how the procurement system as defined by the legal and regulatory framework in
Khyber Pakhtunkhwa Province is operating in practice through the institutions and management
systems that are part of the overall public sector governance in the Province.
Indicator 3. The public procurement system is mainstreamed and well integrated into the
public sector governance system.
This indicator looks at the procurement system to:
a) determine its suitability to discharge the obligations prescribed in the law without gaps or
overlaps;
50
b) whether the necessary links with other sectors of government affecting procurement
exist;
c) whether procurement operations are constrained by other external institutional factors;
and
d) whether the managerial and technical capacity of the system are adequate to do
procurement without unnecessary cost or delay.
This indicator deals with the degree of integration of the procurement system with other parts of
government and particularly with the financial management system given the direct interaction
between the two, from budget preparation and planning to treasury operations for payments.
There are four sub-indicators (a-d) to be scored under indicator 3.
Sub-indicator 3(a) Procurement planning and associated expenditures are part of the
budget formulation process and contribute to multi-year planning
The Planning Cell of the Health Secretariat, Khyber Pakhtunkhwa, under the supervision of the
Chief Planning Officer (CPO), plans for the schemes by formulating Annual Development
Programme (ADP). Work on preparation on ADP starts in January of the each financial year.
Demands for inclusion of schemes are received on prescribed formats from districts, autonomous
institution, programme managers and public representatives. The demands for new schemes are
analyzed/scrutinized in light of government policies and Departments priorities at various levels.
The draft ADP, after approval of Minister Health, is sent to P&D Department for approval. A number
of meetings are held at P&D Department level on the draft ADP. After scrutiny/analysis by the P&D
Department, the draft ADP is placed for approval of Chief Minister. Afterwards, the draft is placed
before the Provincial Cabinet and the Provincial legislature for approval. In ADP both ongoing and
new projects are included.
The following types of schemes are included in ADP:-
1. Account-Head-42:
Brick & Mortar: For construction of new health facility, upgradation of health facility,
addition/alteration in the existing health facility)
2. Account-Head-36:
For purchase of equipment/instruments/furniture for a health facility or programme. For
activities to achieve certain targets/goals. Such soft components like control of TB/Hepatitis
Program/EPI etc involvestaff salaries, purchase of medicines/equipment and other
operating costs.
After approval of the ADP from the Provincial Assembly, the scheme PC-Is is prepared and
approved from the following competent forums:
1. Departmental Development Working Party (DDWP): Schemes upto Rs.60 million.
2. Provincial Development Working Party (PDWP): Scheme upto Rs. 5 billion.
51
(However schemes involving Federal share or donor funding are sent to the Federal Govt. for
approval of CDWP/ECNEC irrespective of cost of the scheme).
Administrative approval of the scheme is issued and the allocation of scheme reflected in ADP for
release by the Finance Department. The funds released by the Finance Department are then placed
at the disposal of the concerned in the executing agency. Funds on capital side (construction) are
placed at the disposal of C&W Department and funds on the revenue side (equipment/furniture/
medicine/salaries etc) are placed at the disposal of concerned DDO.
The following procedures are followed for procurement of equipment/medicine approved in the PC-I
of the schemes:
1. Funds for purchases are placed at the disposal of DDO/Project Director.
2. Technical, purchase and Inspection committees are notified for the purchases.
3. The specification for equipment/item to be purchased are prepared by a technical
committed constituted for the purpose.
4. The equipment/items to be purchased are advertised in newspapers.
5. Comparative statements are prepared after receipts of bids.
6. The bids received are technically/financially examined by a technical committee.
7. Purchase Committee meeting is held to approve bids in light of the Technical Committee
SOPs and NWFP Procurement Rules 2003. The bids which are not approved are re-
advertised.
8. The Purchase Orders of the approved item/s are given to the selected firms.
9. After supply of the item/s by the firm, Inspection Committee inspects the supplied items in
light of the approved specification.
10. In case of satisfactory report of the Inspection Committee, payment is made by the DDO
to the firm.
Any distortion in the procurement planning and subsequent budget formulation process is seen in
the Province when politically motivated schemes or schemes based on expediency / urgency are
introduced for construction of some new facility i.e., a cardiac center etc or upgradation of the
existing medical facility i.e., from BHC to Category-C Hospital etc. In such cases, the realization of
the Standardization List specified for an upgraded facility results in erection of structures or
procurement of more sophisticated equipment which do not match with the disease burden or
outpatient load for that particular area where such facility is intended to be created. Hence best
value for money may not be achieved in this regard as the said requirements are not properly
envisaged at the time of their consolidation at the Department level which makes the cost data for
budget allocation less reliable. Politically triggered schemes are also one of the reasons for
inclusion of non-ADP budgetary estimates that are most of the time not realized due to some
reason. Around 25-30% of the development budget does not get spent every year and has to be
52
surrendered by the Department thereby losing its development impact.
Periodic updation of the budget by the Department is not frequent to reflect any revised changes
that take place in timing of contracts. However, the Health Department predicts the cost of similar
goods, works or services in future budget years based on experience of the actual cost of goods,
works and services provided in earlier years and may project the same from 10-20%. To the extent
of pharmaceutical goods and medical furniture, it may be near to actual costs as the product
development cost and market prices for the said products do not change much. For bio-medical
equipment significant variation in the price may occur for the machines and assemblies where
technical specification change frequently due to rapid advancements in technology. It has been
observed that the prices for the similar bio-medical items have remained almost same to the ones
bought earlier which means that the neither the technical specifications of such items have been
updated by the Department nor sufficient market research has been conducted in this regard. This
may pose a moderate risk in the costing scenario prepared by the Health Department procuring
entities.
There is visible contribution from the Planning Cell towards the ADP document in terms of support
to the health budget planning and its formulation for health sector. However, the Health Department
in general and the Directorate General Health Services in particular do not prepare any activity-
specific Procurement Plan in a standardized format to depict planned and actual dates for initiation
and closure of contract actions for procuring the intended goods indicated in the ADP above. Lump
sum estimated amounts are allocated in advance in ADPs. This shows a rather weak linkage of
contracting processes with the budget planning and may tend to compromise Departments
capability to understand the timing of major contracts, to predict cash flow needed to make timely
payments to the suppliers (often delayed due to late inspections of equipment) and to reduce the
extra costs associated with delayed contract completion. TRF has helped HSRU in preparing a
standard Procurement Plan on the internationally agreed-to prescribed format for procurement of
Management Services to provide integrated health services on the basis of Public Private
Partnership (PPP) to the six crises-stricken districts in Khyber Pakhtunkhwa. A similar Procurement
Plan can be utilized by the DGHS as well for its activities related to procurement of bio-medical
equipment.
Scoring Criteria Score
There is a regular planning exercise instituted by law or regulation that:
starts with the preparation of multiyear plans for the government agencies,
from which annual operating plans are derived.
followed by annual procurement plans and estimation of the associated
expenditures.
and culminates in the annual budget formulation.
Procurement plans are prepared in support of the budget planning and
formulation process.
3
53
The majority of procurement plans are prepared based on the annual and
multiyear operating plans independently from budget allocation but they are
revised to meet the forward budget estimates for the sector or agency allocations
before expenses are committed.
2
Procurement plans are normally prepared based on the annual and multiyear
operating plans. Links with budget planning are weak and plans are not required
to match the budgetary allocation available before expenses are committed.
2
There is no integrated procurement and budget planning of the nature described.
Procurement plans are drawn without obvious and direct connection with the
budget planning exercise and there is no requirement to match procurement
plans with availability of funds before expenses are committed.
0
Sub-indicator 3(b) Budget law and financial procedures support timely procurement,
contract execution, and payment.
This sub-indicator assesses the degree to which budget law and financial management procedures
are adequate to meet procurement needs.
(a) Budget funds are committed or appropriated within a week from the award of the contract
to cover the full amount of the contract (or amount to cover the portion of the contract to
be performed within the budget period).
(b) There are published business standards for processing of invoices by the government
agencies that meet obligations for timely payment stated in the contract.
(c) Payments are authorized within four weeks following approval of invoices or monthly
certifications for progress payments.
No timelines for committing budget funds for award of contracts have been prescribed by any
Provincial budget manual for utilization by the Health Departments Planning Cell as these are
already committed in the development budget. The current budget, prepared on the basis of needs
reflected earlier by the Department, is allocated in lumpsum to the Health Department from where it
is disbursed to the procuring entities by Section Officer Budget. However, the Planning Cell, in
addition to the Accountant General of Pakistans General Financial Rules (GFR), makes use of the
two manuals namely, Manual for Development Projects and Planning Commission Guidelines for
Project Management published by the Planning & Development Division Islamabad to offer
published business standards for processing of invoices.
The Manual for Development Projects alludes to Para 105 of GFR-Vol-I, AGPR Rules, which directs
the public sector authorities not to leave unpaid the indisputably payable amount as far as possible,
and that money paid should, under no circumstances, be kept out of accounts a day longer
than is absolutely necessary. The GFR also states that it is no economy to postpone inevitable
payments and it is very important to ascertain the budget estimates and then liquidate and
record the payment of all actual obligations at the earlier possible date. GFR further calls
attention to the fact that the Principal Accounting Officer shall make prompt On-Account
54
payments to suppliers and contractors against their invoices or running bills within the time
given in the conditions of the contract which shall not exceed thirty (30) days, as stipulated in Rule
43 of Federal Public Procurement Rules (PPR), 2004 issued by the Finance Division vide
SRO 432(1) / 2004 dated 8th June, 2004.
Though the development budget funds are already appropriated against the amount of contracts to
be awarded to the successful suppliers in various schemes through the ADP and are available, the
timelines for payments to suppliers generally seem to exceed the contractual timelines prescribed
above as Departmental inspection of Bio-Medical equipment is not conducted for months with no
significant reason and despite creation of liability under Rule 3 of the NWFP procurement of Works,
Goods & Services Rules 2003. This has been dealt in detail in Sub-Indicator 7(c ) & Sub-Indicator
8(a). The procurement, budget and financial management systems therefore need to interact in a
way that once procurement decisions are made and contract actions are completed these should
trigger the corresponding actions on the budget and financial side in due time for timely
disbursements.
Scoring Criteria Score
Budget and financial procedures in place meet the requirements of a) to c)
above formulation process.
3
Budget and financial procedures in place meet the requirements of a) but there
are no published business standards. Authorization of payments is generally
timely.
2
Procedures in place take longer than stated in a) and conditions b) and c) are
not generally met.
2
The procedures in place do not meet the requirements in a material way. 0
Sub-indicator 3(c) No initiation of procurement actions without existing budget
appropriations.
This indicator assesses whether there are safeguards in the system precluding initiation of
procurement actions unless funds have been allocated to the procurement in question. For this the
following requirements should be in place:
(a) The law requires certification of availability of funds before solicitation of tenders takes
place.
(b) There is a system in place (e.g. paper or electronic interface between the financial
management and the procurement systems) that ensures enforcement of the law.
AGPRs GFR Para 12 indicates the certification of availability of funds before solicitation of tenders
takes place. The schemes in the ADP contain development funds which have been allocated to the
procurement in question and therefore show availability of funds before solicitation of tenders. The
current budget is further made available for procurement of pharmaceutical products on emergency
basis to the Health Department for providing to the EDOs (Health). It sometimes happens that a
Non-ADP scheme gets introduced into the ADP if need arises. Funds to such schemes are provided
55
through re-appropriation within the sector. As PIFRAs electronic interface has yet not been able to
ensure initiation of financial management of contract actions by the Health Department, paper-
based management of the said procurement activity is prevalent.
Scoring Criteria Score
The system meets requirements (a) and (b) above.. 3
The system meets requirement (a) but requirement (b) is not fully enforced due
to weaknesses in the system.
2
The system meets requirement (a) only. 1
There system does not meet requirements (a) and (b). 0
Sub-indicator 3(d) Systematic completion reports are prepared for certification of budget
execution and for reconciliation of delivery with budget programming.
This sub-indicator is a measurement of the feedback mechanism needed to ensure that information
on contracts covering major budget expenditures is provided to the budgetary and financial
management systems in a timely manner to support the overall public financial management
system.
When the payment bill is deposited with the AG/District Accounts Officer, it gets processed and the
payment to the firm by AGPR. The expenditure is booked in the PIFRA System. The stated
information is reconciled and sent back to the AGPR for finalization of appropriations to accounts.
The said process is further extended for reconciliation and appropriation of running and final bill
payments to suppliers accounts and indicates the completion of major contracts by PIFRA.
However, giving a complete picture on the project sign-off or closure remains out of scope of this
financial management system in the absence of any Materials Management Module in the
procurement system of the Health Department.
As discussed earlier, health budget for procurement is directly appropriated to the EDO (Health)
after its sanction from DGHS, Peshawar for ADP Schemes. However, for the current budget some
EDOs (Health) do not even feel the need of the said sanctioning from DGHS and directly get
reimbursed from the DCO. This year 8 out of 25 districts did not seek the sanction of Directorate
General Health Services for disbursement of their health budgets for procurement. In this case, the
DGHS may not have any information on the procurements made at the district level. This exposes
the inherent weakness of the financial management system regarding disbursements on
procurement in some instances as it does not make the budget sanction mandatory by the DGHS.
Scoring Criteria Score
The procurement system is sufficiently integrated with the financial management
and budgetary systems to provide information on the completion of all major
contracts.
3
Information on completion of the majority of large contracts is submitted as
described above.
2
56
Information on the completion of contracts is erratic or is normally submitted with
considerable delay after the fiscal budgetary period.
1
The procurement system does not generally provide this information. 0
Indicator 4. The province has a functional normative/regulatory body.
Indicator-4 relates to the existence of a Public Procurement Regulatory Authority in the Khyber
Pakhtunkhwa Province.
Draft Khyber Pakhtunkhwa Public Procurement of Goods, Works and Services Bill 2012 has been
approved by the Provincial Assembly and notified on 20.09.2012 as Khyber Pakhtunkhwa Public
Procurement Regulatory Authority 2012. Khyber Pakhtunkhwa Public Procurement Rules 2012 are
now pending signatures of Chief Secretary Khyber Pakhtunkhwa & and their implementation in all
the Government departments in the Province. Creation of this regulatory authority would lead to
emergence of the procurement functions within the public sector and their proper discharge,
independence of the regulatory function, the effectiveness of performance and the degree of
coordination between responsible organizations. Until the said regulatory body is manned with
officials to function it will not have any utility and does not come under the scope of discussion
under reference at present. The scoring for this indicator therefore remains zero for the said
purpose.
Indicator- 5: Existence of institutional development capacity.
The objective of this indicator is to assess the extent to which the Province or Department has
systems to support and monitor the performance of the entire system, and to formulate and
implement improvement plans.
Sub indicator 5 (a) The Province has a system for collecting and disseminating
procurement information, including tender invitations, requests for proposals, and contract
award information.
The objective of this indicator is to determine
a) the existence and capacity of the procurement information system in the Province;
b) the accessibility of the information system;
c) the coverage of the information system; and,
d) whether the system provides one stop service (to the extent feasible) where those
interested can find information on procurement opportunities and outcomes.
Health Department does have a Planning Cell which has a capacity for analysis, feedback
mechanisms and planning for implementation of improvements. However, such capacity exists for
the purpose of annual planning, budget formulation and associated expenditures and does not
generate any annual or multi annual procurement plans. The District Health Information System
(DHIS), an Information Technology arm of the DGHS Khyber Pakhtunkhwa disseminates quarterly
57
provincial reports based on health-related data and posts subsequent analysis on its website for the
twenty five districts of Khyber Pakhtunkhwa.
Health Department also publishes on its website selected procurement information for public
access. Rule-31 (c to g) of the NWFP Procurement Rules 2003, in order to promote competition
and transparency, provides for access to general public only upon request, the information relating
to participating bidders on their qualification / disqualification, comparative Evaluation Summary and
grounds of their rejection either under Rule-32 (for sole technically evaluated bidder) or under Rule-
8(2) (for non-submission of secondary documentation).
For posting the Standard Bidding Documents for procurement of bio-medical equipment and
pharmaceutical products for Govt-MCC for the year 2012-13, temporary web-links were created on
DHIS website and published in the IFB for access by the prospective bidders. However, the DGHS
neither has a dedicated web-link or an automated ERP Contract Management system like
Prodagio
or Share Point
software programs which are dedicated solely to the collection and
dissemination of information focused on procurement nor does it offer any one-stop services related
to information on procurement opportunities and outcomes.
Scoring Criteria Score
There is an integrated information system that provides as a minimum, up-to-
date information as described above and is easily accessible to all interested
parties at no or minimum cost.
Responsibility for its management and operation is clearly defined.
3
There is an integrated system of the characteristics described that provides up-
to-date information for the majority of contracts at the central government level
but access is limited.
2
There is a system but it only provides information on some of the contracts and
the system accessibility is limited.
1
There is no procurement information system except for some individual agency
systems. Entities keep information on contract awards and some statistics.
0
Sub-indicator 5 (b) The Province has systems and procedures for collecting and
monitoring national procurement statistics.
For purposes of this sub-indicator, the focus is on data available on procurement undertaken using
provincial budget funds.
As statistical information on procurement is essential to evaluate the policies and the operation of
the system, it also provides a means for monitoring performance and compliance in a legal and
regulatory framework. Unfortunately, the Directorate General Health Services (DGHS) has not yet
been able to force the Districts, Vertical Programs and AMIs to send their annual requirements to
the Divisional Office in Peshawar well in advance for the sake of generating any statistical
information to be used as a tool for procurement planning and market analysis. This non-
58
compliance, though administrative in nature, may be attributable to lack of existence of any system
in operation to collect data on:
i) procurement by method,
ii) duration of different stages of the procurement cycle,
iii) awards of contracts,
iv) unit prices for most common types of goods and services;
v) any other information that allows analysis of trends, levels of participation, efficiency and
economy of the purchases and compliance with requirements.
This may be attributable largely to a mix of centralized and decentralized procurement systems
simultaneously at the Divisional and District levels. Resultantly, the credibility of any such
information on procurement conducted by the Health Department, especially by the DGHS and its
subsidiaries has been compromised as it has not been verified by any audit and no routine analysis
of any such information is carried out except for upgradation of the approved formulary/medicine list
by the Govt-MCC, DGHS.
Scoring Criteria Score
The country has a system that meets the four requirements (a) through (d) listed
above.
3
The country has a system that meets (a) plus two of the remaining conditions. 2
The system is in place to meet (a) plus one of the remaining conditions. 1
There is no statistical data collection system in place. 0
Sub-indicator 5 (c) A sustainable strategy and training capacity exists to provide training,
advice and assistance to develop the capacity of government and private sector participants
to understand the rules and regulations and how they should be implemented.
The purpose of this sub indicator is to verify existence of permanent and relevant training programs
for new and existing staff in government procurement.
Until recently, no dedicated training programs related to procurement skill enhancement were
conducted in the Health Department Khyber Pakhtunkhwa as there was no strategy existing at the
departmental level to envisage such needs to generate and maintain the supply of qualified
procurement staff. The Health Services Academy in Peshawar seems to have its major focus on
management training to the doctors. The ongoing USAID DELIVER Project in Khyber Pakhtunkhwa
is involved on the nation-wide supply chain of contraceptives through its Logistics Management
Information System (LMIS), besides catering to the training needs of the Districts staff in the LMIS
discipline. The said training component does not address the specific requirements of a
procurement life cycle. Keeping in view the magnitude of funds involved and sensitivity of time in
getting the best value for money and product efficacy, this neglected area poses far greater risk
than anticipated.
59
Scoring Criteria Score
There is a training and capacity building strategy that provides for:
(a) Substantive permanent training programs of suitable quality and content
for the needs of the system.
3
(b) Evaluation and periodic adjustment based on feedback and need.
(c) Advisory service or help desk to absolve questions by procuring entities,
suppliers, contractors and the public.
There is a training and capacity building strategy that provides for a) above. 2
The existing program is of poor quality and insufficient to meet the needs of the
system and there is no procurement help desk or advisory service.
1
No formal training or help desk programs exist. 0
Sub-indicator 5 (d) Quality control standards are disseminated and used to evaluate staff
performance and address capacity development issues.
The purpose of this sub-indicator is to verify existence, relevance and comprehensiveness of the
quality assurance and standards for processing procurement actions and to ensure their systematic
application to provide for monitoring of performance..
Although these types of standards will vary widely between different administrative levels, they
should as a minimum:
(a) Provide quality assurance standards and a monitoring system for procurement processes
and products
(b) Provide for a staff performance evaluation process based on outcomes and professional
behaviors.
(c) Ensure that operational audits are carried out regularly to monitor compliance with quality
assurance standards.
Though the NWFP Procurement Rules 2003 do mention response time for pre-qualification and
tender submission, no quality control standards with respect to purchasers performance evaluation
exist or have been disseminated at the level of Health Department to verify the existence of any
such standards which might include response times to reply to inquiries, or length of time to prepare
tender documents after receipt of a requirement. It is due to this fact that time and again the courts
feel the need to interfere on related matters in the Province regarding issues of product efficacy and
spurious drugs bought through procurement procedures which could not assure quality. The
Provincial Quality Control Board (PQCB) Khyber Pakhtunkhwa under the Health Department has a
robust mechanism for detecting, seizing and prosecuting spurious or sub-standard medicines in the
market but its operation may be a post-procurement measure and is not directly related to
procurement of drugs by the Department.
60
No monitoring system so far existed for assuring quality of procurement process or staff
performance in this regard including any performance based incentives for achieving efficiency in
procurement processes. Ironically, the only quality assurance mechanism existing at Departmental
level is the pre-qualification process by which mercantile and manufacturing expertise of suppliers
and manufacturers of bio-medical equipment, drugs and surgical disposables is judged by the
Department.
So far, at the level of Department of Health, to assess & evaluate purchasers performance no
mechanism has been developed for conducting the internal audit and observations from the
external audit have not been translated into a lesson i.e., developing some tangible form of
operational standards to avoid emergence of similar observations on procurements in future. The
external audit conducted by the AGPR also seems to have developed expertise on revenue receipt
audit and not on expenditure audit, resulting in observations by audit which are based not on non-
observance of procurement procedures by the procuring agency but on the probable financial
improprietary, as viewed by audit. The interesting examples in this regard are the audit observations
wherein the Health Department is asked to explain why the lowest evaluated responsive bid was
selected instead of instead of the lowest priced bid. Similarly, any drug procured through open
competition by Govt-MCC, if found costlier than the market, has also been objected by the Audit.
Such an instance is beyond the control of the Department and has been identified as a risk
alongwith its mitigation strategy in the Assessment Report.
Scoring Criteria Score
The procurement system complies with (a) through (c) above. 3
The procurement system complies with (a) and (b) above but there is no regular
auditing to monitor compliance..
2
The procurement system has quality standards but does not monitor nor use the
standards for staff performance evaluation.
1
The system does not have quality assurance or staff performance evaluation
systems.
0
5.8 Pillar III. Procurement Operations and Market Practices
This Pillar looks at the operational effectiveness and efficiency of the procurement system at the
level of the implementing entity responsible for issuing individual procurement actions. It looks at the
market as one means of judging the quality and effectiveness of the system when putting
procurement procedures into practice. This Pillar is distinguished from Pillars I and II in that it is not
looking at the legal/regulatory or institutional systems in a Province but more at how they operate.
Indicator-6. The Provinces procurement operations and practices are efficient.
This indicator looks at the efficiency of the operations and operational practices as implemented by
the procuring agencies.
61
Sub-indicator 6 (a) The level of procurement competence among government officials
within the entity is consistent with their procurement responsibilities.
The purpose of this sub-indicator is to assess the degree of professionalism and knowledge of
those responsible for implementation of procurement activities that:
(a) there are defined skill and knowledge profiles for specialized procurement jobs.
(b) there is systematic matching of skills against requirements for competitive recruitment.
(c) staff required to undertake procurement activities on an ad hoc basis have the knowledge
they need to undertake the activity or have access to professional staff that can provide
this knowledge.
The procurement for pharmaceutical products, surgical disposables, bio-medical equipment and
goods of general nature at the Directorate General Health Services (DGHS), Vertical Programs,
AMIs and Health Projects is being conducted in a traditional way by the related officials & staff who
are supposed to carry out the activity through drafting of the Tender Inviting Notice for publication,
updating the Formulary or the list of bio-medical equipment, preparing the list of general items and
submitting the same to the authorized departmental committees comprising sector specialists from
pharmacy, medicine, surgery and bio-medical engineering fields for review, approval and
subsequent purchasing.
The business functions stated above have so far ranged from clerical errands to the administrative
approvals & scrutiny in a repetitive way to establish traditional purchasing practices. The Director
General Health Services and the Chief Executives of the AMIs seemed proficient in current
procurement processes in the health sector. However, none of the above personnel seemed to
have any formal skill and knowledge profile for specialized procurement jobs as per the above
stated Sub-indicator 6(a) as neither there has been any dedicated effort to develop such profile on
any professional footing through customized procurement trainings in the Health Department nor
has there been any academic pursuit of getting a degree, diploma or certificate in procurement
management.
Very few officials of the Health Department Khyber Pakhtunkhwa have attended the two-day
training in public procurement management on PPRA Rules 2004 in National Institute of Training
(NIT) PPRA Office Islamabad in recent years. In the absence of any public procurement regulatory
authority in Khyber Pakhtunkhwa for initiating a formal training on public procurement in the
Province, NIT in Islamabad is therefore the only venue available which offers the procurement
officials of Health Department Khyber Pakhtunkhwa to align their purchasing functions with
international best practices in public sector contracting but has largely remained unexplored so far.
The Directorate General Health Services though, in July 2011, initiated a one-time effort on capacity
building of drug inspectors, Provincial Quality Control Board and Drug Testing Laboratory Khyber
Pakhtunkhwa under in terms of inspection and drug sampling protocols in a four-day workshop
through Drug Control Strengthening Project which focused on quality of the product but not on its
acquisition methodology.
62
Posting out of officials dealing with procurement from the concerned sections in the Health
Department have also made the fair implementation of procurement procedures ineffective.
Recently, establishment of a Procurement Cell in DGHS has been an important step in initiating
centralized purchasing of bio-medical equipment and general items on the basis of requirements
generated by the districts, but no formal officials have been dedicated for posting to the said Cell.
This may be attributed to lack of any systematic matching of skills against requirements of
competitive recruitment for the procurement function in the Health Department which is considered
as a secondary function vis--vis provision of health services as the primary function.
The variance in professional efficiency and operational practices of the procurement staff appointed
to undertake procurement activities on an ad-hoc basis has therefore resulted in delayed award of
contracts and occasional misprocurement due to procedural lapses.
The maturity assessment of the procurement function of Health Department Khyber Pakhtunkhwa
typically considers the dimensions like strategic planning and objectives, organization design,
strategic sourcing and category management, buying operations, supplier management, contract
management, risk and governance management, performance management, knowledge/
information management and organizational capability (skills). The Department has yet to develop
defined skills for the above said dimensions of the procurement functions through specialized
capacity building of their officials.
Scoring Criteria Score
The system meets the requirements (a) through (d) listed above. 3
The system meets (a) plus one of the remaining conditions. 2
The system only meets (a) above. 1
The system does not meet any of the requirements. 0
Sub-indicator 6(b) The procurement training and information programs for government
officials and for private sector participants are consistent with demand.
This sub indicator assesses the sufficiency of the procurement training and information programs in
terms of content and supply.
(a) Training programs design is based on a skills gap inventory to match the needs of the
system.
(b) Information and training programs on public procurement for private sector are offered
regularly either by the government or by private institutions.
(c) The waiting time to get into a course (for public or private sector participants) is
reasonable, say one or two terms.
Though the NWFP Procurement Rules 2003 remain a precursor to Federal PPRA Rules 2004 and
almost both tend to share best practices in transparency and contracting techniques, as earlier
discussed above in indicator 6(a) the Health Department has neither designed any dedicated
professional program based on any of the above stated set of Procurement Rules to develop
63
procurement skills of its officials nor has there been any academic pursuit of getting a degree,
diploma or certificate in procurement management by the concerned.
The strategic initiatives taken on provision of health service delivery for the masses in the Province
also seems devoid of any training programs and awareness workshops for the suppliers in the
private sector to educate them for submitting responsive bids. No training calendar has ever been
developed by the Health Department or the Provincial Health Services Academy (PHSA) in
Peshawar to cater to the needs for procurement related trainings at regular intervals. PHSA could
have been a valuable venue for such events for maturing Departmental resources into assets for
the procurement function with its faculty members as Master trainers on public procurement as well.
Scoring Criteria Score
The training and information programs available meet all the requirements listed
in (a)-(c) above.
3
The training programs are sufficient in terms of content and frequency (waiting
time) for government participants but there are few information programs for
private sector..
2
There are training programs but they are deficient in terms of content and
supply.
1
There is no systematic training or information program for public or private sector
participants.
0
Sub-indicator 6(c) There are established norms for the safekeeping of records and
documents related to transactions and contract management
The ability to look at implementation performance is dependent upon the availability of information
and records that track each procurement action. A system for safe-keeping of records and
documents should include the following:
(a) The legal/regulatory framework establishes a list of the procurement records that must be
kept at the operational level and what is available for public inspection, including
conditions for access.
(b) The records should include:
Public notices of bidding opportunities
Bidding documents and addenda
Bid opening records
Bid evaluation reports
Formal appeals by bidders and outcomes
Final signed contract documents and addenda and amendments
Claims and dispute resolutions
Final payments
Disbursement data (as required by the Provinces financial management system).
64
(c) There is a document retention policy that is compatible with the statute of limitations in the
Province for investigating and prosecuting cases of fraud and corruption and with the
audit cycles.
(d) There are established security protocols to protect records either physical or electronic.
Safekeeping of records and documents related to transactions and contract management is vital to
the functioning of both internal & external control systems and for reviewing the past contracting
actions preserved as organizational process assets. The Health Department Khyber Pakhtunkhwa
and its subsidiaries have kept the procurement record in safe custody for access to external audit
and inspection by other agencies. Separate file for each supplier/manufacturer has been maintained
with respect to his contract actions in most of the cases instead of a master file, containing the
proceedings from Tender Inviting Notice (TIN) to contract award. In the absence of a streamlined
filing system in Procurement Cell & Govt-MCC section, finding administrative approval regarding a
particular procurement activity becomes the sole specialty of the section assistant. However, the
overall sanctity of the preserved record seems intact.
Rule 31 of the NWFP Procurement Rules 2003 binds the Tender inviting Authority to maintain
record of procurement proceedings related to the nature of procurement activity, detail of
participating suppliers/contractors and their contract price, information relative to any qualification,
disqualification or rejection of bidders under Rule 32 of the said Rules, summary of comparative
evaluation of bids and name of Lowest Evaluated responsive Bidder who has been awarded the
contract. No visible security protocols established administratively, either physical or electronic,
were observed in the Department.
However, unlike Rule 46 of the Federal PPRA Rules 2004 whereby all procuring agencies have to
retain the related record for a minimum period of five years, the NWFP Rules 2003 do not assign
any such period. Despite the absence of a statute, the Department has kept procurement
documents since 1996 or earlier since the creation of Govt-MCC stuffed in cupboards in an un-
indexed form.
Scoring Criteria Score
The procurement system complies with the requirements (a) through(d) listed
above.
3
The procurement system complies with requirements (a), plus two of the
remaining conditions.
2
The procurement system complies with (a) but not with the rest. 1
There is no mandatory list of documents or retention policy leaving it to the
discretion of the procuring entity.
0
Sub-indicator 6(d) There are provisions for delegating authority to others who have the
capacity to exercise responsibilities.
Delegation of authority and responsibility is key to having a well functioning system especially when
procurement is decentralized.
65
Delegation should be undertaken in accordance with the following:
(a) Delegation of decision making authority is decentralized to the lowest competent levels
consistent with the risks associated and the monetary sums involved.
(b) Delegation is regulated by law.
(c) Accountability for decisions is precisely defined.
In the absence of any specific provision in NWFP Procurement Rules 2003 for delegation of
financial powers, the provisions of the North West Frontier Province Delegation of Financial Powers
under the Financial Rules & the Powers of Re-Appropriation Rules 2001 are observed vide which
the function of the Procuring Agency has been duly delegated from the Health Secretariat to the
Directorate General Health Services for central rate contracting for drug rates and subsequently to
the AMIs, Vertical Programs, Health Projects and EDOs of the districts for issuing purchase orders
through need-based decentralized contracting for pharmaceutical products mentioned in the
approved Formulary & bio-medical equipment (exclusive of non-drug surgical disposables and
general items etc. which are procured by the subsidiaries). Though the decentralization is governed
administratively, little accountability could be visible for the decisions taken by the DGHS
subsidiaries in terms of identifying or consolidating their procurement needs for annual procurement
planning hence over-specified bio-medical equipment is collecting dust in some districts &
Teaching Hospitals /medical units in the absence of both the personnel trained to run the said
machines and the intended end user.
Scoring Criteria Score
The system meets all requirements listed in a) c) above. 3
The law establishes delegation and accountabilities but the system concentrates
decisions at a high level creating congestions and delays.
2
Delegation is regulated in very general terms creating a need to clarify
accountability for decision making.
1
Delegation is not regulated by law and left at the discretion of the procuring
entity. There is lack of clarity on accountability.
0
Indicator-7: Functionality of the public procurement market.
The objective of this indicator is primarily to assess the market response to public procurement
solicitations. There are three sub indicators (a-c) to be scored.
Sub-indicator 7(a) There are effective mechanisms for partnerships between the public and
private sector.
The investment friendly policies of the Provincial Government of Khyber Pakhtunkhwa, the Health
Department being a reliable purchasing client and the increasing interest of the foreign donors in
helping the Department to eradicate & roll back diseases like Polio, Measles, HIV/AIDS, Malaria
and neo-natal tetanus etc through various Vertical Programs and Health Projects in the Province,
have generated considerable demand for bio-medical equipment, medical furniture, medical kits,
surgical disposables and pharmaceutical products etc. in the Province. This has attracted either
66
various pharmaceutical firms to establish their manufacturing premises in Khyber Pakhtunkhwa or
compete in the tendering process from other provinces to create a public procurement marketplace
and consequently a partnership wherein the government is the buyer and the private sector is the
supplier of the needed goods, works or services amounting to around Rs 1.25 billion annually.
However, most of the suppliers were of the view that they just wanted an introduction in the
Government business otherwise supplying pharmaceuticals to the Health Department consumed
much time and was not worth doing business compared to the their retail operations in private
sector market, private hospitals and other autonomous institutions like Railway and armed forces
etc.
Such an arrangement has led to a dire need for some dialogue between the Health Department and
the private sector with regard to practices by the Department relating to pre-qualification and
tendering that had undermined the competitive effectiveness of the private sector in some areas.
Though Rule 11 of NWFP Procurement Rules 2003 mentions some response time to the applicant
for pre-qualification, there is no minimum time specified in Rule 17 of the said Rules for
communicating the prospective bidders of changes, clarifications or amendments in the bidding
documents. Misuse of Rule 20(2) regarding reducing the mandatory period of 30 days to any
number of days without a cogent reason has potentially restricted the competitive environment for
which no forums are available in the Health Department for its dialog with the private sector on
deliberating upon any such practices. Similarly, the Standard Bidding Documents, after getting
advertised or posted on web, can only be amended or changed by the approved Technical &
Evaluation Committee as per approved administrative SOPs but the same are amended by the
Directorate General Health Services without intimation to the said Committee. The above said
operational lacunae have raised concern among competitors from the private sector. However, the
private sector has recently relied upon the Health Department as a partner-in-development under
the public private partnership arrangements for providing management consultancy services for
revitalizing and strengthening the health service delivery in six crises affected districts of Khyber
Pakhtunkhwa by the Health Sector Reforms Unit (HSRU), Health Department Khyber Pakhtunkhwa.
But it should be kept in mind that the said partnership has been ensured under the Multi-Donor
Trust Fund (MTDF) by the World Bank. An effective, reliable and transparent mechanism for
sustaining such a partnership from the Department itself has yet to come.
The Department, despite its arm-twisting prowess, has also not been able to create a forum for
initiating dialogue with the local pharmaceutical industry on eradication of spurious drugs. Such
dialogue could have initiated self-correcting actions by the drug associations themselves in the
private sector in taking measures to identify counterfeit medicines supplied in the market and taking
punitive measures against the unscrupulous manufacturers and suppliers with the help of the
Department. Any one-sided effort on the part of the Department so far by prosecuting the
unscrupulous suppliers through lenient penalties under Section 27 of the Drug Act 1976,
introducing alpha-numeric bar code stickers for supply of genuine drugs to the Department or any
other measures without the private sector stakeholders buy-in, has resulted in futility.
67
Scoring criteria Score
(a) Government encourages open dialogue with the private sector and has
several established and formal mechanisms for open dialogue through
associations or other means.
3
(b) The government has programs to help build capacity among private
companies, including for small businesses and training to help new entries
into the public procurement marketplace.
(c) The government encourages public/private partnerships and the
mechanisms are well established in the legal framework to make possible
such arrangements.
The system meets (a) plus one other condition above. 2
The system only provides for (a) above. 1
There are no obvious mechanisms for dialogue or partnership between the
public and private sector.
0
Sub-indicator 7(b) Private sector institutions are well organized and able to facilitate
access to the market.
This sub-indicator looks at the capacity within the private sector to respond to public procurement in
the Province.
Pharmaceutical firms, bio-medical equipment suppliers and general item suppliers from the private
sector are the usual small and medium enterprises (SMEs) which are the business partners of the
Health Department. Around two hundred registered and pre-qualified firms possess the necessary
organizational capacity to access the information and other services to promote their participation in
the tendering process initiated by the Department all the year round. The pharmaceutical sector, at
the moment, seems to be well organized and competitive in terms of its professional staff and
manufacturing capabilities with respect to the firms pre-qualified with the Department on stringent
criteria and is keen on competition.
However, some areas of competition, like vaccines for Hepatitis-B and Tuberculosis and biological
drugs like Hepatitis-C etc., are monopolized by certain multinational suppliers owing to their
probable dominance in global research. Standard Interferon anti-viral therapy for combating
Hepatitis-C has been pioneered since 2002 by a few multi-national companies like M/s Roche
Pharma Ltd and M/s Schering Plough Ltd etc. M/s Roche Pharma Ltd have further initiated the
observational Sustained Virologic Response (SVR) Research Studies for Biosimilar Pegylated
Interferon on multi-continental representative samples since 2007 for non-responders and relapsers
to the treatment of Hepatitis-C, which have been published in indexed journals of international
repute and has created some reference standards for conducting head-to-head clinical trials to be
carried out by other firms Local companies like M/s BF Biosciences and M/s Getz Pharma etc. tend
to compete with the multi-nationals in the bidding process but seem deficient in providing head-to-
head clinical trials based on a longer duration, in publishing any detailed SVR Research studies of
their competing products in indexed journals of international repute or demonstrating any significant
share in the local market as indicated by IMS Health USA, a global pharmaceutical database.
68
Though the said aspects may limit the competition for Hepatitis-C drug, the same need to be
included in the Technical evaluation Criteria to get quality medicines of high therapeutic value from
well-reputed pharmaceutical firms. The Technical Evaluation criteria also contains pharmaco-kinetic
& pharmaco-dynamic in-vivo Bio-Equivalence studies for Anti-Tubercular drugs for determining
proof of sustained response against the disease through continuous serum efficacy and the same
have been made mandatory for technical qualification of the bidders for specialized drugs.
The Directorate General Health Services has ensured that in order to achieve high efficacy of the
specialized product such reference standards should become part of the Technical Evaluation
Criteria of the revised Bidding Documents for procurement of specialized drugs for the Govt-MCC
for the year 2012-13. The above stated reference standards have restricted the participation of
many new entrants supplying or manufacturing specialized drugs dealing with Interferon therapy
who have been agitating against the inclusion of the said reference standards. However, despite
resistance, the Directorate General Health Services has taken a firm stand on achieving high quality
biological products keeping in view the sensitivity of the prevailing situation regarding Hepatitis-C
and Tuberculosis and has strived to ensure supply of quality biological drugs by retaining the
reference standards like SVR Reports for Interferon therapy and Bio-Equivalence Studies for Anti-
Tubercular drugs in the revised Standard Bidding documents.
Scoring Criteria Score
The private sector is competitive, well organized and able to participate in the
competition for public procurement contracts.
3
There is a reasonably well functioning private sector but competition for large
contracts is concentrated in a relatively small number of firms.
2
The private sector is relatively weak and/or competition is limited owing to
monopolistic or oligopolistic features in important segments of the market.
1
The private sector is not well organized and lacks capacity and access to
information for participation in the public procurement market.
0
Sub-indicator 7(c) There are no major systemic constraints (e.g. inadequate access to
credit, contracting practices, etc.) inhibiting the private sectors capacity to access the
procurement market.
This Sub-indicator has been assessed through a questionnaire distributed among various suppliers
of pharmaceutical products and bio-medical equipment. The majority of feedback revolved around
the pre-qualification exercise conducted by the Health Department annually to assess the efficacy of
the industrial processes of the manufacturers and supply chain mechanisms adopted by the
importers or suppliers. The suppliers of the bio-medical equipment and surgical instruments were
mostly the importers of the said equipment and were of the view that annual pre-qualification
exercise for them was redundant in view of the nature of supply, process involved and definition of
the product which remained almost constant due to established market practices and fixed product
definition with anticipated upgrades. They were of the view that manufacturers and importers of the
69
pharmaceutical products needed to be checked frequently during the year and through surprise
visits as well, to randomly verify the quality of daily, weekly or monthly batches of medicines and
drugs turning out of production locally.
The importers of the drugs & surgical disposables, on the other hand, were of the view that the
Batch Certificate on Form-7 under Rule 14(d)(i) of Drugs (Import & Export) Rules 1976 from the
Drug Regulatory Authority of the country of export or from manufacturer and submitted by the
importers fulfilled the need for ascertaining the source of raw material and quality of the product,
hence their annual pre-qualification was not needed.
Regarding private sectors access to credit by the Health Department in the form of any mobilization
advance, no such facility is provided in the contract clauses for procurement of bio-medical
equipment, pharmaceutical products or general items etc. Certain suppliers maintained that the
banks usually extended credit line facility to only those suppliers whose import volume was large
enough to comply with their corporate risk coverage; hence not many of the importers could get any
leverage from banks for opening Letter of Credit and had to import directly from the manufacturers
by sending cash in advance to cover the risk of manufacturers but in turn risking their investments.
Certain suppliers of the pharmaceutical products or bio-medical equipment had the strong
impression on the survey scale of intensity that their bid securities were not timely released despite
definite time period given in the bidding documents for their return and even after submission of
Performance Security in case of selection of their pharmaceutical products through central rate
contracting by the Govt-MCC at Peshawar. They had to wait for the Purchase Orders to be issued
from the EDOs (Health) to get their bid securities back and therefore remained at the mercy of the
EDOs (Health) The suppliers were of the view that results of the drug samples obtained by the
Department were not timely conveyed by the Drug Testing Laboratories leading to delay in their
final payments. This not only affected their investment circulation but reduced their financial
capability for participating in other contracts.
Many suppliers informed in the survey that originally they were distributors of pharmaceutical
products, including drugs, surgical disposables, medical supplies and bio-medical equipment on
behalf of the majority of the major local and multi-national manufacturers in pharmaceutical sector
but due to a recent decision of the Peshawar High Court vide Para 9 of the Writ Petition No.
2478/2010 (Daily Mashriq Vs Secretary Health & Others), they were barred from participating on
behalf of manufacturers. The said decision directs the Health Department to purchase drugs only
from original manufacturers or their authorized importers. However, in the new set-up the
manufacturers are still having the same distributors in the guise of their authorized suppliers serving
their interests owing to the reason that the manufacturers traditionally either do not have the reach-
out potential for marketing of their products to the extent the distributors have with their dedicated
expertise, or do not yet want to develop the same and save the expenditure on establishing any
inter-city corporate setup.
This scenario has created not only a dichotomy for the Health Department which is in realization of
the actual situation and may be keeping silent for a while in violation the Honourable High Courts
70
decree but also for the distributors working in the garb of authorized suppliers who now face a risky
situation in terms of their financial investment with manufacturers thereby having absolutely no
coverage for the bid securities and performance securities deposited by them on behalf of the
manufacturers. The inherent risk in this situation has emerged out of lack of their agency agreement
with the manufacturers with whom they club together for supply of pharmaceutical products without
any contractual privity. Resultantly with investment getting riskier, they are getting reluctant to
participate on behalf of the firms in the public sector affecting the competition of manufacturing firms
as well. The hue and cry raised by the representatives of the pharmaceutical companies recently
regarding increase in the bid security from Rs. 100,000 to Rs 500,000 by the Directorate General
Health Services Khyber Pakhtunkhwa as a primary qualification for participation in Govt-MCC
procurement of drugs for the year 2012-13 reflected the above mentioned state of affairs. The T&E
Committee evaluating in detail the Technical bids for the above mentioned procurement activity has
categorically instructed all the participating firms that the Department would not allow anybody else
except bidding firms regular employees with their salary slips to submit firms bids and their
presence at the time of firms financial bid opening for the year 2013-14.
Inclusion of KIBOR rate of interest in the contracting provisions for paying 2% of the delayed
amount to the seller by the government is considered to reasonably distribute the risk associated
with untimely payment upon performance of contract and helps offset the cost of doing business
with the government. However, the previous contractual arrangements between the Health
Department Khyber Pakhtunkhwa and the suppliers demonstrates that the pharmaceutical/bio-
medical engineering firms participating in tenders have long conceded their stated right by not
pressing upon the Health Department to include the above mentioned provision in the contract.
Hence the survey displays an alarming trend of delayed payments due to late inspections of bio-
medical equipment by the Department or late DTL Reports for pharmaceuticals to the sellers by the
Department forcing the suppliers to adopt undesirable practices for release of their payments and a
possible constraint to competitive bidding.
Scoring Criteria Score
There are no major constraints inhibiting private sector access to the public
procurement market.
3
There are some constraints inhibiting private sector access to the public
procurement market, but competition is sufficient.
2
There are multiple constraints inhibiting private sector access to the public
procurement market which often affect competition levels.
1
There are major constraints that discourage competition and the private sector
firms are generally reluctant to participate in public procurement.
0
Indicator- 8: Existence of contract administration and dispute resolution provisions.
This indicators objective is to assess the quality of contract administration practices which begin
after contract award and continue to acceptance and final payments. This is an area that many
procurement systems fail to consider. It is also a period where many issues arise that can affect the
71
performance of the contract and impact on service delivery. This indicator covers three sub-
indicators (a-c) to be scored.
Sub-indicator 8(a) Procedures are clearly defined for undertaking contract administration
responsibilities that include inspection and acceptance procedures, quality control
procedures, and methods to review and issue contract amendments in a timely manner.
This sub-indicator addresses all of the following procedures which are important aspects of contract
administration:
(a) Procedures for acceptance of final products and for issuance of contract amendments
are part of the legal/regulatory framework or are incorporated as standard clauses in
contracts.
(b) Clauses are generally consistent with internationally accepted practices (see IFI
standard contracts for good practice examples).
(c) Quality control (QC) procedures for goods are well defined in the model
contracts/documents or in the regulations. QC is carried out by competent officers,
inspection firms or specialized testing facilities. (DTL)
(d) Supervision of civil works is carried out by independent engineering firms or qualified
government supervisors and inspectors.
(e) Final payments are processed promptly as stipulated in the contract.
The Health Department had been using, until recently, a traditional contract template for
procurement of bio-medical equipment and pharmaceutical products which contained some
essential provisions dealing with payments, fraudulent practices, item delivery, products shelf life
or warranty and notices with basic level of treatment for each of them with respect to risk mitigation.
Little did the template offer any credible procedure to resolve contractual disputes through
arbitration considered vital for credibility of review procedures.
With the introduction of revised Standard Bidding Documents based on FIDIC Standard Templates
and customized for specialized operation related to the supply of health sector goods in August
2012, the internationally agreed-to standard contractual provisions found their way in the
procurement business processes for contract administration like Statement of Works (SOW),
Performance Reporting, Period of Performance, Roles & Responsibilities, Sellers Place of
Performance & Delivery, Pricing & Payment Terms, Inspection & Acceptance criteria, Warranty &
Product Support, Limitation of Liability, Penalties, Incentives, Insurance & Performance Bonds, Sub-
Contractor Approvals, Change Request handling, Incoterms for supply chain risk allocation,
Contract Termination and Alternative Dispute Resolution (ADR) Mechanisms for supplies and
Retainage fees for any civil works etc if required. Service Level Agreement (SLA) elaborating
maintenance requirements and training needs, has therefore become a standard appendage to the
main contract.
72
Instead of a single 100% payment method at the end of each accepted supply, a dual payment
rgime was introduced in the Special Conditions of Contract of the Standard Bidding Documents
based on 80% payment at the time of supply and 20% after the acceptance of product by the Client
and upon fulfillment of other contractual obligations.
This dual payment rgime aims at easing out the agony of the supplier who had been constantly
waiting for the Quality Assurance Report of the Drug Testing Laboratory (DTL) for approval of the
sample taken by the Department for making payments. In the wake of absence in the NWFP
Procurement Rules 2003 of any enforcement clause for payment by the Department in some
prescribed period, Section 22 of the Drugs Act 1976 provides a mandatory period of two months for
furnishing the same. The process may take upto one and a half month for injectables as the
prepared media in the Sterility Test may take atleast 14 days to show any positive growth thereby
leading to another two weeks to duplicate the test to ensure the said growth. The tablets or
capsules may take not more than two weeks if all goes well. This is the minimum time that the
supplier has to bear out with the Department for receiving its payment if no other bureaucratic
hurdles are created afterwards to extort any gratification from the supplier.
However, any genuine delay by the DTL should not undermine the significance of the sampling for
assuring Quality Control (QC) conducted by the Health Department as the said procedure derives
its strength from the Drug Act 1976 & standard SOPs developed for the Pre-Qualification process
and is used at the supply stage by involving the DTL to ensure product quality. In this regard, an
interesting observation has been reported by the DHIS Provincial Report of the 1
st
quarter 2012
stating that 100% of the drug samples collected are those being manufactured locally by local
companies and no sample has been taken from any multi-national pharmaceutical firm. This
requires some soul searching on the part of the members of the Govt-MCC Selection (Purchase)
Committee to make the right decisions based on quality and not on lowest price regardless of the
low cost quoted for bulk purchases of medicines to be supplied in the government hospitals.
Though the dual payment clause may now theoretically reduce the disbursement time during
contract administration, the 60-days mandatory period for drug sampling and testing practically
reduces the probability of any timely payment based on contractual terms. The suspension of the
KIBOR Clause by the Department through the inactivating Condition Subsequent in the Special
Conditions of Contract (SCC), as mentioned above in Sub-Indicator 7(c) has, under Common Law,
created a precedence in favour of the Client and may pose a contractual risk for the seller. The
same may therefore needs to be mitigated through supplementing any regulation for the said
additional time in the much awaited Khyber Pakhtunkhwa Public Procurement Rules 2012
conforming to the time period in the Drugs Act 1976 for the health sector to establish credibility of
the Department.
Scoring Criteria Score
Contract administration procedures provide for (a) to (e) above. 3
Contract administration procedures provide for (a) plus three of the remaining
requirements.
2
73
Contract administration procedures provide for (a) plus two of the remaining
requirements.
1
Contract administration procedures do not meet the requirements of (a) to (e)
above.
0
Sub-indicator 8(b) Contracts include dispute resolution procedures that provide for an
efficient and fair process to resolve disputes arising during the performance of the contract.
In order to avoid long delays while resolving disputes, a good resolution process should be defined
in the contract that provides for fair and timely resolution. The following describes current good
practice with regard to dispute resolution.
(a) There is an Arbitration law in the Province.
(b) The law is consistent with generally accepted practices for neutrality of arbitrators, due
process, expediency and enforceability.
(c) The Province accepts as a matter of course international arbitration for international
competitive bidding.
(d) Provisions for Alternative Dispute Resolution (ADR) are standard in contracts.
(e) ADR provisions conform to the international standard wording (may refer to IFI standard
bidding documents for sample of good international practice).
Rule 43 of the NWFP Procurement of Goods, Works & Services Rules 2003 provide for the appeal
procedure for the bidders who feel aggrieved by the Procuring Entity and want to file an application
for review of the decision. Unless the Procuring Entity (PE) entered into a contract the aggrieved
bidder may file an application to:
Head of PE if Tender Accepting Authority is other than Head of Procuring Entity
Secretary Industries if Tender Accepting Authority is Head of Procuring Entity
Secretary Law if Tender Accepting Authority is Secretary Industries
District Coordinating Officer if procurement is made with District Government funds
Though the said Rule binds the aggrieved bidder to accept the decision of Reviewing Authority as
final and not to challenge it in any court of law, said condition has been rendered ineffective by the
superior judiciary whereby no contractual provision can stop an aggrieved bidder from approaching
a court for redressal of his grievances. The different review tiers mentioned in the said Rule may not
be applicable now in the post-devolution scenario and need revision.
The Arbitration Act 1940 deals with domestic arbitration proceedings and applies to recognition and
enforcement of domestic awards but is not based on the UNCITRAL Model Law. A Bill for a new
consolidated arbitration law based on the UNCITRAL Model Law was presented to the Parliament
on 27 April 2009 and is still pending before the National Assembly. The Bill aims to consolidate law
relating to domestic arbitration, international commercial arbitration, recognition and enforcement of
foreign arbitral awards as well as settlement of international investment disputes. However, even
the Arbitration Act 1940 is consistent with generally accepted practices for neutrality of arbitrators,
74
due process, expediency and enforceability. The same has been included in the recently revised
Standard Bidding Documents for procurement of pharmaceutical products for Govt-MCC.
Pakistan Engineering Council (PEC) has issued the first edition of its Rules on Arbitration &
Conciliation drafted in March 2009. PEC has modeled its rules for conciliation on the principles and
lines of United Nations Commission on International Trade Law (UNCITRAL) taking into
consideration essential elements of Pakistan Arbitration Act, 1940 and relevant provisions of PEC
Regulatory Rgime. Section 283 of The Companies Ordinance 1984 also facilitates dispute
resolution through arbitration. However, for establishing credibility among the foreign donors/buyers,
arbitration forums like International Chamber of commerce (ICC), international Court of Justice
Hague, UNCITRAL model Rules on Arbitration and FIDIC Contract Dispute Resolution mechanism
have been added in the said Standard Bidding Documents for the public-private partnership
arrangements to acquire management consultancy services for revitalizing and strengthening the
health service delivery in six crises affected districts of Khyber Pakhtunkhwa by the Health Sector
Reforms Unit (HSRU) under the Multi-Donor Trust Fund (MTDF) by the World Bank.
Talking on the Country level, Section 49 of the Federal PPRA Rules 2004 provides for the
arbitration but leaves it to the procuring agencies to devise any methodology for that. The Rules of
Arbitration & Conciliation 2009 are well drafted by Pakistan Engineering Council. Adjudicators stand
appointed in the judicial branches of the public sector for dispute resolution. Alternate Dispute
Resolution Committees (ADRCs) to the extent of the Federal Board of Revenue (FBR) for resolving
the disputes outside the courts have already reduced the work load on the Supreme Court and are
a standard practice in the contracts.
In comparison, on the Provincial level Alternate Dispute Resolution (ADR) mechanism has yet to
make its mark in the procurement business processes adopted by the Health Department. In the
absence of any standard mechanism for arbitration under Rule 43 of the NWFP Procurement Rules
2003 and lack of any provincial appellate authority, the aggrieved bidders are free to file complaint
against a procurement process elsewhere ranging from DGHS to Honourable Peshawar High Court
as earlier discussed in Sub-indicator 1(d) regarding Rules on participation despite right of
independent audience granted by the Secretary Health. This has created a contractual risk in terms
of dispute resolution and the Department may definitely consider, in addition to making spontaneous
departmental review committees, adopting the general principles set by the Supreme Court of
Pakistan for recent dispute resolutions through the above mentioned Alternate Dispute Resolution
Committees (ADRCs) which settled a large volume of taxation related cases in Federal Board of
Revenue (FBR), Islamabad. Mediation can be another less hostile mode for dispute resolution
outside the courts which the Department may adopt in certain cases.
Scoring Criteria Score
The system meets all the good practice standards (a) to (e) above. 3
The system meets (a) plus three of the remaining good practice standards. 2
The system meets (a) plus two of the remaining good practice standards. 1
The system does not use ADR as a normal dispute resolution mechanism in
public contracts.
0
75
Sub-indicator 8(c) Procedures exist to enforce the outcome of the dispute resolution
process.
In order to be effective, the contract not only must provide for fair and efficient dispute resolution
procedures, it must also provide for enforcement of the outcome of the dispute resolution process.
The following are some basic conditions.
(a) The country is a member of the New York Convention on enforcement of international
arbitration awards.
(b) The country has procedures to enable the winner in a dispute to seek enforcement of the
outcome by going to the courts.
(c) The country has a process to monitor this area of contract administration and to address
performance issues.
The current good practices for timely resolution of the disputes lie in the free judiciary in the Country
for enforcement of the contract law. There is no specialist arbitration court in Pakistan. The High
Court and such other superior courts in Pakistan as may be notified by the Federal Government in
the Gazette has jurisdiction over recognition and enforcement of foreign awards. The judiciary in
Pakistan is familiar with the laws governing both domestic and international arbitrations.
The Arbitration Act 1940, supplemented by the Contract Act 1872, accepts the international
arbitration as Pakistan itself is a member of the forums regarding international dispute settlement
like Board of the Forum for International Conciliation and Arbitration (FICACIC). There are well
informed arbitration law firms to help enforce the settlement through the judiciary within the Country.
Pakistan is a member of the various other dispute resolution institutions like World Banks
International Center for Settlement of Investment Disputes (ICSID) which helps in the conciliation
and arbitration of international investment disputes. The International Chamber of Commerce (ICC)
is active through ICC Pakistan; however, presently it does not provide any arbitral services.
Pakistan became a signatory to the United Nations Convention on the Recognition and
Enforcement of Foreign Arbitral Awards, 1958, known as New York Convention on 30 December
1958.
The Recognition and Enforcement (Arbitration Agreements Foreign Arbitral Awards) Act
2011, known as The Convention Act, implements the New York Convention in Pakistan and is
limited to the enforcement of foreign arbitral awards. The New York Convention was first
implemented in Pakistan vide the Recognition and Enforcement (Arbitration Agreements and
Foreign Arbitral Awards) Ordinance, 2005 which was subsequently re-promulgated from time to
time before the enactment of the said Convention Act 2011.
Pakistan is party to the Geneva Protocol on Arbitration Clauses of 1923 and Geneva Convention on
the Execution of the Foreign Arbitral Awards of 1927. Pakistan is also a signatory to the
Washington Convention which is a Convention on the Settlement of Investment Disputes between
States and Nationals of Other States of 1965.
It is important to note that in the absence of clear definitions of domestic arbitration, domestic
award, and foreign arbitral award under the arbitration laws of Pakistan, the scope and ambit of
76
the aforementioned laws is unsettled. Accordingly it is possible that a particular arbitration
agreement or arbitral award may attract the application of the Arbitration Act 1940 and/or the
Convention Act 2011.
Scoring Criteria Score
The procurement system in the country meets the requirements of a-c above. 3
The country meets two of the three conditions above. 2
The country meets condition (a) above 1
The country does not meet any of the requirements. 0
5.9 Pillar IV. Integrity and Transparency of the Public Procurement System.
Pillar IV takes aspects of the procurement system and governance environment and seeks to
ensure that they are defined and structured to contribute to integrity and transparency.
Indicator -9: The Province has effective control and audit systems.
The objective of this indicator is to determine the quality, reliability and timeliness of the internal and
external controls preferably based on risk assessment and mitigation.
Equally, the effectiveness of controls needs to be reviewed in terms of expediency and
thoroughness of the implementation of auditors recommendations. The assessment should rely, in
addition to their own findings, on the most current Country Financial Accountability Assessment
(CFAA) or other analysis including PEFA/PFM assessment that may be available. This indicator has
five sub indicators (a-e) to be rated.
Sub-indicator 9(a) A legal framework, organization, policy, and procedures for internal and
external control and audit of public procurement operations are in place to provide a
functioning control framework.
The procurements conducted by the Health Department Khyber Pakhtunkhwa have been annually
audited by the external auditors of the office of the Provincial AGPR. Such an expenditure audit
exercise for oversight of the procurement function derives its legitimacy from the national legislation
establishing the office of the Federal AGPR as constitutional head for the said state organs even
after Post-18
th
Amendment.
However, an Internal Audit mechanism has not been in place in the Health Department for
establishing internal controls for periodically producing recommendations to the heads of the
individual procuring entities based on their findings. TRF has already suggested creation of an
Internal Audit mechanism in its Health Sector Strategy Document for the Province, complemented
by internal control and management procedures that provide for checks and balances within an
agency for processing of procurement actions.
Procurement Audit is an expenditure audit and owing to its process peculiarities, is different from
the Revenue Receipt Audit. Due to its specialized nature, the Health Department therefore needs to
77
develop a skilled Internal Audit workforce with special focus on Procurement Audit. TRF has
suggested the Directorate General Health Services some capacity building measures on
Procurement Audit in the annexed Training Calendar to abreast the Departmental audit officials with
the universally applicable expenditure audit skills to scrutinize individual contract actions in the
procurement activities.
Special Audits are also an infrequent feature for internal checks and balances on Health Projects,
Vertical Programs or any particular aspect of DGHS procurements and are called when required
administratively or for investigating any complaints. These audits address specific risks and check
any controls available for their mitigation and preservation of financial proprietary.
Scoring Criteria Score
The system in the country provides for:
(a) Adequate independent control and audit mechanisms and institutions to
oversee the procurement function.
3
(b) Implementation of internal control mechanisms in individual agencies with
clearly defined procedures.
(c) Proper balance between timely and efficient decision making and
adequate risk mitigation.
(d) Specific periodic risk assessment and controls tailored to risk
management.
The system in the country meets a) plus two of the above. 2
The system meets a) but controls are unduly burdensome and time-consuming
hindering efficient decision making.
1
Controls are imprecise or lax and inadequate to the point that there is weak
enforcement of the laws and regulations and ample risk for fraud and corruption.
0
Sub-indicator 9(b) Enforcement and follow-up on findings and recommendations of the
control framework provide an environment that fosters compliance.
The purpose of this indicator is to review the extent to which internal and external audit
recommendations are implemented within a reasonable time. This may be expressed as percentage
of recommendations implemented within six months, a year, over a year or never implemented.
Enforcement and follow-up of recommendations of External Audit by AGPR on past procurements
has to be linked with a monitoring and evaluation function which, unfortunately, is hardly existent as
reflected by the continued business practices on which some audit observations were made. The
audit observations, as seen from the record of the DGHS, were also not based on the standard
international contracting practices which show lack of external auditors skills in expenditure audit.
Among some glaring examples of such practices, one pertains to a distorted interpretation of Rule
34 (2) of the NWFP Procurement of Goods, Works and Services Rules 2003 whereby any surviving
technically qualified bidder is denied further evaluation/participation due to reduction in the number
78
of bidders from a minimum of three during technical evaluation. The said Rule requires a minimum
of three bidders at the time of submission of bids. Interestingly, the DGHS procurement officials
refer to the distorted requirement of the AGPR to include at least three technically qualified bidders
in the Comparative Statement, failing which any sole technically qualified would also be disqualified.
Another example relates to inadvertent submission of technical and financial bids in the same
envelop in a Single Stage Two Envelop Bidding process under Rule 40 of the said Rules 2003,
whereby the submitting firm is considered disqualified. Rules 19-22 of the NWFP Procurement
Rules 2003 dealing with the marking and sealing of bids are also silent on the issue. International
best practices in contracting consider such omissions as minor if the bidder has no objection in case
his financial bid gets revealed due to his own mistake. The Audit also makes observations on
competitive procurement of some surgical disposables which were quoted higher than the prevalent
market price. The said items usually have no labeling and their price quotation was beyond the
control of the Department in the event of open competitive bidding.
Scoring Criteria Score
Internal or external audits are carried at least annually and recommendations are
responded to or implemented within six months of the submission of the auditors
report.
3
Audits are carried out annually but response to or implementation of the auditors
recommendations takes up to a year.
2
Audits are performed annually but recommendations are rarely responded to or
implemented.
1
Audits are performed erratically and recommendations are not normally
implemented.
0
Sub-indicator 9(c) The internal control system provides timely information on compliance
to enable management action.
The following key provisions should be provided:
(a) There are written standards for the internal control unit to convey issues to management
depending on the urgency of the matter.
(b) There is established regular periodic reporting to management throughout the year.
(c) The established periodicity and written standards are complied with.
The Sub-indicator 1(b) related to Procurement Methods, has earlier been dealt adequately with the
appropriate hierarchical levels existing in the Health Department regarding internal controls over
procurement management through various departmental Committees all having written standards.
The said Committees, namely Pre-Qualification Committee, Scrutiny Committee, Comparative
Statement (CS) Committee, Technical & Evaluation Committee and lastly the Purchase Committee,
consist of health sector professionals for examining bids under a competitive bidding method. Their
composition has also been described in the said Sub-indicator. Though the periodic reporting to
management based on a procurement life cycle throughout the year is infrequent as prescribed time
limit for such periodicity is not very well defined in the administrative SOPs, the presence of a pre-
79
qualification calendar initiating such a procurement makes it an obvious attempt on the part of the
Health Department to initiate yearly procurement cycle on time.
Scoring Criteria Score
All requirements (a) through (c) listed above are met. 3
Requirement (a) plus one of the above are met. 2
Only requirement (a) is met. 1
There is no functioning internal control system 0
Sub-indicator 9(d) The internal control systems are sufficiently defined to allow
performance audits to be conducted.
There are written internal control routines and procedures to be adhered to by the auditors through
internal audit and control manual.
Unfortunately, no internal audit control mechanism exists so far in the Health Department as earlier
discussed in Sub-indicator 5(d) regarding Quality Control standards for evaluating staff performance
and addressing capacity development issues and as discussed in Sub-indicator 9(a) regarding
provision of a functioning control framework for public sector procurement.
Scoring Criteria Score
There are internal control procedures including a manual that state the
requirements for this activity which is widely available to all staff.
3
There are internal control procedures but there are omissions or practices that
need some improvement.
2
There are procedures but adherence to them is uneven. 1
The internal control system is poorly defined or non-existent. 0
Sub-indicator 9 (e) Auditors are sufficiently informed about procurement requirements and
control systems to conduct quality audits that contribute to compliance.
Perusal of the audit observation in the Health Department reveals that in view of the traditional
procurement practices conducted by the Department the auditors get the information based on the
said practices. There is hardly any system in place to ensure that
auditors working on procurement audits receive adequate training on expenditure audit or are
selected following the criteria that explicitly requires that they demonstrate sufficient knowledge of
the subject as described in Sub-indicators 5(d) & 9(b) regarding any Quality Control standards
disseminated and used to evaluate staff performance and address capacity development issues in
terms of procurement management.
The annexed Training Calendar proposed by the TRF contains some capacity building based on
short training workshops for procurement audit through which the auditors may receive formal
training on procurement requirements, principles operations, laws and regulations and processes.
80
Scoring Criteria Score
There is an established program to train internal and external auditors to ensure
that they are well versed in procurement principles, operations, laws, and
regulations and the selection of auditors requires that they have adequate
knowledge of the subject as a condition for carrying out procurement audits.
3
If auditors lack procurement knowledge, they are routinely supported by
procurement specialists or consultants.
2
There is a requirement that the auditors have general knowledge of procurement
principles, operations, laws, and regulations but they are not supported generally
by specialists in procurement.
1
There is no requirement for the auditors to have knowledge of procurement and
there is no formal training program and no technical support is provided to the
auditors.
0
Indicator 10. Efficiency of appeals mechanism.
The appeals mechanism was covered under Pillar-I with regard to its creation and coverage by the
legal regulatory framework. Indicator 10 further assesses a range of specific issues regarding
efficiency in contributing to the compliance environment in the Province and the integrity of the
public procurement system. There are five sub indicators (a-e) to be scored.
Sub-indicator 10(a) Decisions are deliberated on the basis of available information, and the
final decision can be reviewed and ruled upon by a body (or authority) with enforcement
capacity under the law.
This sub indicator looks at the process that is defined for dealing with complaints or appeals and
sets out some specific conditions that provide for fairness and due process.
(a) Decisions are rendered on the basis of available evidence submitted by the parties to a
specified body that has the authority to issue a final decision that is binding unless
referred to an appeals body.
(b) An appeals body exists which has the authority to review decisions of the specified
complaints body and issue final enforceable decisions.
(c) There are times specified for the submission and review of complaints and issuing of
decisions that do not unduly delay the procurement process.
Sub-indicator 1(h) has earlier assessed in detail the above stated processes covered under Rule 43
of the NWFP Procurement Rules 2003 which offers opportunity to an aggrieved bidder to file an
application for review of the decision/order of the Procuring Entity awarding a contract - provided the
contract has not already entered into force. The survey of the supplier feedback indicates that they
sometimes get the impression of harassment by the concerned officials for pursuing any complaint
and no specified Provincial appellant forum exists to redress the said issue. The Client feedback, on
the other side, interestingly indicates the frivolity prevalent among the bidders and the frequency
81
with which they lodge complaints on every bidding process. Both the feedbacks reflect the legal
aspects of compliance risks which relate to weak enforceability of regulations.
Scoring Criteria Score
The Province has a system that meets the requirements of (a) through (c) above 3
The Province has a system that meets (a) and (b) above, but the process is not
controlled with regard to (c).
2
The system only provides for (a) above with any appeals having to go through
the judicial system requiring a lengthy process.
1
The system does not meet the conditions of (a) (c) above, leaving only the
courts.
0
Sub-indicator 10(b) The complaint review system has the capacity to handle complaints
efficiently and a means to enforce the remedy imposed.
This indicator deals specifically with the question of the efficiency and capacity of a complaints
review system and its ability to enforce the remedy imposed.
In relation to capacity and efficiency of the grievance redressal system, the Health Department
Khyber Pakhtunkhwa is usually quick enough to arrange representations before the Departmental
Committee instituted in this regard. Keeping in view the outdated procurement regulations in vogue
and traditional administrative practices being carried out, the capacity to handle complaints
efficiently is directly proportional to the magnitude of procurement and sensitivity of allegations
involved. This Sub-indicator is closely related to sub indicator 10(a) which also refers to
enforcement and therefore any administrative indecision regarding compliance gets potentially risky
thereby involving the Department into further litigation.
Scoring Criteria Score
The complaint review system has precise and reasonable conditions and
timeframes for decision by the complaint review system and clear enforcement
authority and mechanisms.
3
There are terms and timeframes established for resolution of complaints but
mechanisms and authority for enforcement are unclear or cumbersome.
2
Terms and timeframes for resolution of complaints or enforcement mechanisms
and responsibilities are vague.
1
There are no stipulated terms and timeframes for resolution of complaints and
responsibility for enforcement is not clear.
0
82
Sub-indicator 10(c) The system operates in a fair manner, with outcomes of decisions
balanced and justified on the basis of available information.
The system needs to be seen as operating in a fair manner. The complaint review system must
require that decisions be rendered only on relevant and verifiable information presented and that
such decisions be unbiased, reflecting the consideration of the evidence presented and the
applicable requirements in the legal/regulatory framework.
The internal controls provided by the Departmental Committees on registration, pre-qualification and
technical evaluation of bidders in the Health Department Khyber Pakhtunkhwa have a fairly
elaborate hierarchical and written mechanism of taking decisions on the related issues. Being a
sensitive sector dealing with health service delivery for the common man on the street and having
little allowance for any error leading to fatalities, the outcome of decisions seems to be significantly
justified on the basis of available information and balanced in terms of suspension of drug licenses,
crackdown on spurious drugs in the Province despite political influence, and selection of efficacious
drug through competitive process. A survey into the medicine sale licenses issued by the EDOs
(Health) and the actual number of outlets selling medicines would give an insight into the problem of
sale of substandard or unregistered drugs since it is most likely that these drugs or a majority of
them originate from unlicensed sale points. The internal controls provided by the Departmental
Committees may therefore be judged on the said criterion as well. With the available remedies
provided for in the legal/regulatory framework under Rule 43 of the NWFP Procurement Rules 2003
and administrative SOPs, representations by the aggrieved parties are handled in such a way that
these have often resulted in unpublished remedies that pertained to the implementation of the
processes relating to pre-qualification and bid evaluation etc.
Scoring Criteria Score
Procedures governing the decision making process of the review body provide
that decisions are:
3
(a) based on information relevant to the case.
(b) balanced and unbiased in consideration of the relevant information.
(c) can be subject to higher level review
(d) result in remedies that are relevant to correcting the implementation of the
process or procedures.
Procedures comply with (a) plus two of the remaining conditions above. 2
Procedures comply with (a) above. 1
The system does not comply with any of the above. 0
Sub-indicator 10(d) Decisions are published and made available to all interested parties
and to the public
Decisions are public by law and posted in easily accessible places (preferably posted at a dedicated
government procurement website in the Internet).
83
As discussed in detail in the in Sub-indicator 6(c) regarding the established norms for the
safekeeping of records related to transactions and contract management, and in Sub-indicator 11(a)
regarding publication of information and its distribution through available media, the Health
Department Khyber Pakhtunkhwa publishes on the website of the EPI Program some procurement
information for public access of the participating bidders. This information relates to their
qualification/disqualification, comparative evaluation Summary, grounds of their rejection under
Rule-32 for sole technically evaluated bidder and under Rule-8(2) for non-submission of secondary
documentation. Specific procurement activities are advertised through IFBs and on DHIS website
but Technical Evaluation Reports are not published.
Scoring Criteria Score
All decisions are publicly posted in a government web site or another easily
accessible place.
3
All decisions are posted in a somewhat restricted access media (e.g. the official
gazette of limited circulation).
2
Publication is not mandatory and publication is left to the discretion of the review
bodies making access difficult.
1
Decisions are not published and access is restricted. 0
Sub-indicator 10(e) The system ensures that the complaint review body has full authority
and independence for resolution of complaints.
This indicator assesses the degree of autonomy that the complaint decision body has from the rest
of the system to ensure that its decisions are free from interference or conflict of interest. Due to the
nature of this sub indicator it is scored as either a 3 or a 0.
The Health Department Khyber Pakhtunkhwa has an administrative hierarchy headed by Secretary
Health and is run by the Rules of Business set by the Government for running day to day
governance through administrative SOPs and official guidelines. Secretary Health is also the Head
of the Selection (Purchasing) Committee and is part of the purchasing process. The process
provided for complaint redressal in Rule 43 of the NWFP Procurement Rules 2003 is not being
followed. Any complaint from the aggrieved person against his decision or against the decision of
the Technical & Evaluation (T&E) Committee is submitted to Secretary Health or routed to him
through Provincial Health Minister or Director General Health Services for grievance redressal.
In the absence any independent Provincial appellate authority, Secretary Health keeping in view the
nature of complaint, either immediately conducts review of the earlier decision himself or creates a
review committee comprising members which are not part of the referenced purchasing process,
usually headed by Special Secretary Health or any Technical member and fully authorizes them to
review the Procuring Entitys decision. This process tends to assure the independence of the
complaint review body and to eliminate any conflict of interest.
The creation of a Provincial appellate authority is indicated in Section-9 of the Drug Act 1976 but
unfortunately its intended functionality is related to drug registration/licensing issues only and is not
84
meant to serve as a appellate tribunal for redressing procurement related grievances. The Khyber
Pakhtunkhwa Public Procurement Regulatory Authority (PPRA) Bill 2012 has been enacted in
September 2012 by the Provincial Assembly four years after its tabling The Provincial Government
has neither manned the PPRA yet nor notified the draft Khyber Pakhtunkhwa Public Procurement
Rules nor notified the draft Khyber Pakhtunkhwa Public Procurement Grievance Redressal Rules.
Keeping in view the speed of legislative enactments by the Provincial Assembly and willingness of
the Provincial Government, not much optimism may be attached to the creation of a higher-level
Provincial Appellate Authority under Section-9 of the Drug Act 1976. But if it happens at some point
of time, its Terms of Reference (TORs) can be extended to include redressal of procurement-related
grievances as well; hence such a step by the Provincial Government will significantly help in
establishing the degree of autonomy and independence required for such state organs.
Scoring Criteria Score
The complaint review body is independent and autonomous with regard to
resolving complaints.
3
NA 2
NA 1
The complaint review body is not independent and autonomous with regard to
resolving complaints.
0
Indicator-11: Degree of Access to Information.
This indicator deals with the quality, relevance, ease of access and comprehensiveness of
information on the public procurement system.
Sub-indicator 11(a) Information is published and distributed through available media with
support from information technology when feasible.
Despite limited access allowed by Rule-31 (c to g) of the NWFP Procurement Rules 2003 for
providing information to general public, the Health Department publicly disseminates the information
relating to the participating bidders on their qualification or non-submission of qualification,
comparative evaluation Summary, and grounds of their rejection under Rule-32 and Rule-8(2).
Specific procurement activities are advertised through IFBs and on DHIS website but Technical
Evaluation reports are not published.
As earlier discussed in Sub-indicator 1(a), NWFP Procurement of Works, Goods & Services Rules
2003, while having been published in NWFP Local Government Planning Manual in 2003, are not
publicly accessible on any web-portal of Health Department KP, or as a matter of fact on the
Government of Khyber Pakhtunkhwa website which displays only North-West Frontier Province
Procurement of Goods, Works, Services and Consulting Services Ordinance, 2002 but hosts more
than 900 different public rules, regulations, acts & laws since 1798 till 2008 spanning over two
hundred years. This may lead to transparency issues as there are no means available for finding
any public information on procurement regulations through a user-friendly point of access. Though
some of the information relating to the technical aspects of the product may contain proprietary,
85
commercial, personal or financial information, the timely public disclosure of information on
completion of the tendering process with respect to the above said Rules 31 & 32 of the NWFP
Rules 2003, need a dedicated web-portal for easy public access. Necessary SOPs for achieving the
said purpose could not be found in this regard.
Scoring Criteria Score
Information on procurement is easily accessible in media of wide circulation and
availability. The information provided is centralized at a common place.
Information is relevant and complete. Information is helpful to interested parties
to understand the procurement processes and requirements and to monitor
outcomes, results and performance.
3
Information is posted in media not readily and widely accessible or not user
friendly for the public at large OR is difficult to understand to the average user
OR essential information is lacking.
2
Information is difficult to get and very limited in content and availability. 1
There is no public information system as such and it is generally up the
procuring entity to publish information.
0
Indicator 12. The Province has ethics and anticorruption measures in place.
This indicator assesses the nature and scope of the anticorruption provisions in the procurement
system. There are seven sub indicators (a-g) contributing to this indicator.
Sub-indicator 12(a) The legal and regulatory framework for procurement, including tender
and contract documents, includes provisions addressing corruption, fraud, conflict of
interest, and unethical behaviour and sets out (either directly or by reference to other laws)
the actions that can be taken with regard to such behavior.
This sub indicator assesses the extent to which the law and the regulations compel procuring
agencies to include fraud and corruption, conflict of interest and unethical behavior references in the
tendering documentation.
The Health Department Khyber Pakhtunkhwa has made part of the earlier bidding documents the
provisions addressing corruption, fraud, conflict of interest, and unethical behaviour which remain
integral part of the revised Standard Bidding Documents as well. The said provisions also set out
that the punitive damages ten times the amount of contract price can be imposed with regard to
such behavior. The revised Standard Bidding Documents include the definitions of what is
considered fraud and corruption and the consequences of committing such acts. This sub indicator
is related to sub indicator-2(b) on content for model bidding documents but is not directly addressed
in that sub indicator.
National Accountability Bureau has set the threshold of Rs 50 million or above for intimating all the
proceedings of a procurement activity and has made it enforceable through its regulatory
framework. Whereas all accountability focus seems to be on the public officials, there is a need for
bringing in an anti-corruption legislation for unscrupulous suppliers as well who try to bribe the
86
government officials. The US Foreign Corrupt Practices Act (FCPA) levies fines & penalties on the
foreign sellers for bribing US public sector procurement officials acquiring goods and services under
the US Federal Acquisition Regulations. Inference can be drawn from the said Act in creating a
similar legislation at home.
Scoring Criteria Score
The procurement law or the regulations specify this mandatory requirement and
give precise instructions on how to incorporate the matter in tendering
documents. Tender documents include adequate provisions on fraud and
corruption
3
The procurement law or the regulations specify this mandatory requirement but
leaves no precise instruction on how to incorporate the matter in tendering
documents leaving this up to the procuring agencies. Tender documents
generally cover this but without consistency.
2
The legal/regulatory framework does not establish a clear requirement to include
language in documents but makes fraud and corruption punishable acts under
the law.
Few tendering documents include appropriate language dealing with fraud and
corruption
1
The legal framework does not directly address fraud, corruption or unethical
behavior and its consequences. Tender documents generally do not cover the
matter.
0
Sub-indicator 12(b) The legal system defines responsibilities, accountabilities, and
penalties for individuals and firms found to have engaged in fraudulent or corrupt practices.
NWFP Procurement of Goods, Works & Services Rules 2003 do not expressly define
responsibilities, accountability and penalties for individuals and firms found to have engaged in
fraudulent or corrupt practices. However, Provincial Anti-Corruption Department and National
Accountability Bureaus Provincial arm address the sanctions for such actions by the public
servants. The provisions regarding conflict of interest express action against the concerned officials
but do not spell out the ways and means by which such conflict of interest arises. Anti-corruption
laws contain provisions to stop intervention in procurement matters by any active or formal public
officials for a reasonable period of time after leaving office, in ways that benefit them, their relatives,
and business or political associates financially or otherwise. But the said provisions seem to be
disconnected with the infirmities of the procurement processes and need to be re-aligned with
revised business processes contained in the Provincial procurement rules whenever notified, for
vindication of the innocent.
Scoring Criteria Score
The legal/regulatory framework explicitly deals with the matter. It defines fraud
and corruption in procurement and spells out the individual responsibilities and
consequences for government employees and private firms or individuals found
guilty of fraud or corruption in procurement, without prejudice of other provisions
in the criminal law.
3
87
The legal/regulatory framework includes reference to other laws that specifically
deal with the matter (e.g. anti corruption legislation in general). The same
treatment is given to the consequences.
2
The legal/regulatory framework has general anti corruption and fraud provisions
but does not detail the individual responsibilities and consequences which are
left to the general relevant legislation of the country.
Few tendering documents include appropriate language dealing with fraud and
corruption
1
The legal/regulatory framework does not deal with the matter. 0
Sub-indicator 12(c) Evidence of enforcement of rulings and penalties exists.
This indicator is about the enforcement of the law and the ability to demonstrate this by actions
taken.
Perusal of the record of the contravention cases and subsequent disqualifications of the retailers
and manufacturers of the pharmaceutical products has revealed Khyber Pakhtunkhwa Health
Departments resolve to eradicate spurious drugs and to ban unscrupulous drug suppliers and
manufacturers by stringent pre-qualification proceedings and frequent surprise raids on sale and
manufacturing outlets. Though not an easy indicator to score in terms of contravention cases made
and percentage of them prosecuted owing to the political influence exerted on the Department, the
said figures however indicate that a significant portion of cases get treated for suspension of drug
licenses and disqualification during pre-qualification proceedings in the wake of a big challenge
posed by spurious drugs flooding the local market.
Scoring Criteria Score
There is ample evidence that the laws on corrupt practices are being enforced in
the country by application of stated penalties.
3
There is evidence available on a few cases where laws on corrupt practices
have been enforced.
2
Laws exist, but evidence of enforcement is weak. 1
There is no evidence of enforcement. 0
Sub-indicator 12(d) Special measures exist to prevent and detect fraud and corruption in
public procurement.
This sub indicator looks to verify the existence of an anticorruption program and its extent and
nature or other special measures which can help prevent and/or detect fraud and corruption
specifically associated with public procurement.
There is no special anti-corruption program to prevent and detect fraud and corruption in public
procurement except for inviting Provincial NAB authorities in the T&E Committee meetings which is
a self-defeating approach to make the external reviewers part of the internal process. Transparency
88
International has yet to make an impact in the Province for monitoring a transparent and efficient
procurement system and for providing public information to promote accountability and
transparency. There are no public seminars conducted by the Provincial Government in general or
Health Department in particular on exposing collusive practices in procurement, or any awareness
campaigns, focusing on public sector purchasers and private sector suppliers, as part of efforts to
change social behavior in respect to corrupt practices and creating zero tolerance towards the
same.
Scoring Criteria Score
The government has in place a comprehensive anticorruption program to
prevent, detect and penalize corruption in government that involves the
appropriate agencies of government with a level of responsibility and capacity to
enable its responsibilities to be carried out. Special measures are in place for
detection and prevention of corruption associated with procurement,
3
The government has in place an anticorruption program but it requires better
coordination or authority at a higher level to be effective. No special measures
exist for public procurement.
2
The government has isolated anti-corruption activities not properly coordinated
to be an effective integrated program.
1
The government does not have an anticorruption program 0
Sub-indicator 12(e) Stakeholders (private sector, civil society, and ultimate beneficiaries of
procurement/end-users) support the creation of a procurement market known for its integrity
and ethical behaviors.
This indicator assesses the strength of the public in maintaining a sound procurement environment.
Health Department Khyber Pakhtunkhwa has demonstrated its resolve to fight corruption in the
procurement processes. Vigilance Committees composed of government officials from different
offices and civil society entities for all the 25 Districts have been formed by the Department in
compliance with the orders of the Honourable Peshawar High Court, Peshawar passed in Suo Moto
Writ Petition No. 3129/dated 28-02-2012, 27-06-2012 & 12-09-2012, for providing oversight to
exercise any social control by some respected or credible civil society groups. A typical Vigilance
Committee for a District is composed of:
Sr.No. Designation
1 District Coordination Officer Chairman
2 Executive District Officer (Health) Secretary/Member
3 Executive District Officer Agriculture Member
4 Medical Superintendent DHQ: Hospital Member
5 All Sub Divisional Magistrates in the District Member
6 Tehsil Municipal Officer in the District Member
7 District Food Controller Member
89
8 President District Bar Member
9 President Bazaar Union Member
10 President District Press Club Member
Functions:
1. The Vigilance Committee would make surprise raids specially at night time on all district, tehsil
and jail hospitals to check the services provided, the presence of the medical officers, the
paramedical staff and all allied facilities and deficiencies or absence from duty shall be
reported to the DG Health Services/Secretary Health in the prescribed manner and one copy
should be faxed to the Registrar Peshawar High Court, Peshawar directly.
2. The committee would check particularly in the night-shift any un-authorized staff, personating
as a medical officer and if found so, to be proceeded against under the law immediately and be
given punishment which he deserves.
3. The Committee would furnish fortnightly report of its activities regularly to the Secretary
Health/DG Health Services with copy to the Registrar, Peshawar High Court, Peshawar
besides report as mentioned in No.1 & 2 of its TORs.
The Honourable Peshawar High Court is very active for establishing and reinforcing social audit and
control through the joint effort of the Provincial Government and civil society groups. However, the
Government still lacks on its own at a larger scale, initiatives on welcoming such groups to generate
quality debates towards creating an environment where integrity and ethical behavior is expected
and deviations are not tolerated. Public seminars on aspects related to transparency and open
competition in public procurement are rarely seen by the Health Department.
Scoring Criteria Score
(a) There are strong and credible civil society organizations that exercise
social audit and control.
"
(b) Organizations have government guarantees to function and cooperation
for their operation and are generally promoted and respected by the
public.
(c) There is evidence that civil society contributes to shape and improve
integrity of public procurement.
There are several civil society organizations working on the matter and the
dialogue with the government is frequent but it has limited impact on improving
the system.
2
There are only a few organizations involved in the matter, the dialogue with the
government is difficult and the contributions from the public to promote
improvements are taken in an insignificant way.
1
There is no evidence of public involvement in the system OR the government
does not want to engage the public organizations in the matter.
0
90
Sub-criteria 12(f) The Province should have in place a secure mechanism for reporting
fraudulent, corrupt, or unethical behavior.
The Health Department Khyber Pakhtunkhwa provides information on all procurements exceeding
Rs 50 million to NAB through a system for reporting fraudulent, corrupt or unethical behavior that
provides for confidentiality. However, the Department itself reacts quickly to reports as verified by
subsequent actions taken to address the issues reported by any other agency through traditional
ways. A probable automated ERP Contract Management System seems to be the need of the hour
to be installed at the level of the Procurement Cell, DGHS to provide real-time access to the flow of
acquisition processes, their completion timings and personnel involved in disposing of the related
contract actions.
Scoring Criteria Score
There is a secure, accessible and confidential system for the public reporting of
cases of fraud, unethical behavior and corruption.
3
There is a mechanism in place but accessibility and reliability of the system
undermine and limit its use by the public.
2
There is a mechanism in place but security or confidentiality cannot be
guaranteed.
1
There is no secure mechanism for reporting fraud, unethical behavior and
corruption cases.
0
Sub-criteria 12(g) Existence of Codes of Conduct/Codes of Ethics for participants that are
involved in aspects of the public financial management systems that also provide for
disclosure for those in decision making positions.
Submission of Annual Confidential Reports (ACRs) is a regular feature of the reporting mechanism
for a Code of Conduct/Ethics that applies to all gazetted provincial public officials meeting financial
disclosure requirements. However, no separate requirements for officials involved in public
procurement are in place to deter them from committing any financial improprietary.
Scoring Criteria Score
(a) There is a code of conduct or ethics for government officials with particular
provisions for those involved in public financial management, including
procurement
"
(b) The code defines accountabilities for decision making and subjects
decision makers to specific financial disclosure requirements.
(c) The code is of obligatory compliance and consequences are
administrative or criminal
The system meets requirements (a) and (b) but is only a recommended good
practice code with no consequences for violations unless covered by criminal
codes.
2
There is a code of conduct but determination of accountabilities is unclear. 1
There is no code of conduct. 0
91
6. Section: II Pharmaceutical Supply Chain of Health Department,
Khyber Pakhtunkhwa
The Supply Chain of pharmaceutical products and bio-medical equipment to the procurement
entities of the Health Department, Khyber Pakhtunkhwa was studied through visits to the selected
sites e.g., Pharmaceutical warehouses of EDO (Health) Abbottabad, Mansehra and Peshawar,
Medicine Store of District Headquarters Hospital Abbottabad, MNCH Vertical Programs, Peshawar,
Warehouses of Lady Reading Hospital (LRH) Peshawar, Hayatabad Medical Complex Peshawar,
Khyber Teaching Hospital (KTH) Peshawar, IRNUM Peshawar, Khyber Medical College Peshawar
and Khyber College of Dentistry Peshawar. Apart from physical observation on-site, a
questionnaire, based on the international best practices by the WHO was provided to the Stores
management for filling up. The information so received, reveals that that most of the said practices
regarding storage and inventory are not being carried out as per internationally recognized
guidelines laid out by the WHO. The rest of the warehouses in other districts in the Province could
not be visited due to the travel advisory. However, the concerned EDOs (Health) were conveyed
the said questionnaire for their feedback telephonically and through email. Various EDOs (Health)
were interviewed who were present during the monthly capacity building and training sessions on
procurement.
As observed, the supply chain of the bio-medical equipment is of not much an issue compared to
the pharmaceutical products which require specific storage environments and distribution protocols
and therefore will be the focus of ensuing discussion. By looking at the representative inventory in-
practice samples mentioned above, the following observations on the storage & warehousing,
inventory management, product requisition, distribution and physical verification of the
pharmaceutical goods were made:
Receipt of Goods:
EDO (Health), being the administrative head and the Drawing & Disbursing Officer (DDO) of the
District, issues the Purchase Orders for the medicines whose unit rates have been selected by the
Govt-MCC at DGHS, Peshawar. The purchases made by the EDO (Health) are normally based not
on the requirements conveyed by the primary health facilities like BHUs and RHCs etc in his district
but on a drive to consume the budget allocated for the purchase of medicines and surgical
disposables. The medicines are supplied by the supplier selected by the Govt-MCC to the EDO
Healths warehouse from where these are distributed to the said primary health facilities, civil
hospitals, BHUs and RHCs etc..
Medical Superintendent (MS) of a District Headquarter Hospital is under administrative supervision
of the EDO (Health) but remains Incharge/Drawing & Disbursing Officer (DDO) of the DHQ at the
District and separately issues Purchase Orders for the medicines of the firms selected by the Govt-
MCC at DGHS. The medicines are supplied by the supplier to the DHQs Medicine Store from
where these are provided to the Hospital wards. The requirement of the DHQ is based on the
indents received from the Hospital wards which are prepared by the Incharge nurse. The indents,
after getting checked by the Registrar and counter-verified by the MS, go to the Hospital Medicine
store and the medicine stock is issued thereof to the wards.
92
The Autonomous Medical Institutions (AMIs) also receive their medical supplies from the Govt-MCC
approved suppliers and use procedures similar to the DHQs. The Medical colleges, on the other
hand, usually do not purchase pharmaceutical products except for chemicals used in laboratories
and mostly focus on procurement of bio-medical equipment. These have their dedicated equipment
warehouses from where the same are distributed to the concerned sections for installation.
Storage & Stacking of Medicines:
Pallets for storing the medicines were observed to be in acute shortage in the warehouses of all the
health facilities like AMIs, EDO (Health) Stores, Vertical Programs and to some extent in DHQs. The
stacking of the all medicines was not done on dedicated pallets and mostly were placed on the floor
without any consideration of the humidity. The pharmaceutical warehouses/Medicine Stores of the
EDO (Health), DHQ Abbottabad and AMIs were air-conditioned and contained deep freezers for
storing vaccines and biological drugs. However, the purpose-built specialized deep-freezers with
temperature display could only be found at the HMC, Peshawar. The pharmaceutical warehouse of
MNCH at Peshawar was in a deplorable condition with all the medicines placed open on dirty floor
in a non-air-conditioned room and did not employ any dedicated person for checking the dosage,
strength and packaging of the goods received.
Due to lack of any dedicated space in AMIs, the medicines are also stacked there on each other
adjacent to walls and without any clear therapeutic classification in the corridors which have been
annexed to the warehouses before transferring them into the stores. LRH has its analgesics
(narcotics) in lock & key and maintains strict protocols on their issuance.
Inventory Management: Abbottabad and Mansehra Districts contains a good inventory management
system and their pharmaceutical warehouses at the District and DHQ level are well-maintained but
the record keeping is manual. However, distribution of pharmaceutical products in reefer containers
to primary health facilities in the outer reaches of the districts is not done by the EDOs (Health).
Distribution is not an issue for the DHQs and AMIs as the said medicines need to be consumed
within the facility where they are received.
Except for the warehouses of EDO Abbottabad and EDO Mansehra, no specific quarantine area
designated for receipt of goods, their segregation and inspection was observed in the stores of
other districts, AMIs, DHQs and Vertical Programs due to lack of space. However, staff is there to
receive the goods and place the goods in the warehouse after reconciling the batch number of the
medicine, its name, strength, quantity, expiry date and date of receipt with the details mentioned in
the Purchase Order. The ledger system is maintained by keeping the order, delivery challan and
receipt invoice details. Though the record showed the date of dispatch to primary health facilities in
districts, it did not show the documentation of the date of actual delivery of the medicines to the
intended facilities by the EDOs (Health) and Vertical Programs.
The AMIs and DHQs keep an estimate of the average working stock for each product with a fixed
amount of safety (buffer) stock. SOPs for stock Management were made available by the AMIs only
based on quarterly re-ordering frequency. No such arrangement is available with EDOs (Health).
93
Hayatabad Medical Complex, Peshawar runs a computer-based inventory management systems on
Oracle platform for its main pharmacy attached to five other satellite pharmacies within the facility
premises. The said program displays the following information with options to generate reports:
Medicines Monthly Balance Sheet (Summary)
Medicines Monthly Balance Sheet (Detail)
Daily Unit Indent Page
Main Pharmacy Monthly Consumption
Main Pharmacy Indent Detail
Satellite Pharmacy Monthly Consumption
Satellite Pharmacy Indent Detail
Main Pharmacy Unit Ledger
Satellite Pharmacy Unit Ledger
Short Expiry Summary (Financial Year-wise / Financial Year-wise + Source-wise)
Main Pharmacy Stock-Receiving Challan
In HMC, the stocks from the regular pharmacy are exchanged with the Emergency Relief Package
(ERP) pharmacy when the need arises.
Requisition of Stock:
There is no appropriate procedure for a primary health facility for requisitioning medicines from the
pharmaceutical warehouses of EDOs (Health) and Vertical Programs. The Store Incharge usually
guides the primary facility supervisors to place orders and then pushes the stock to the said facilities
on estimations based on earlier consumptions without considering any current variation in disease
burden in their areas. As informed by Dr. Zafeer Ahmad, EDO (Health) Abbottabad, a computerized
consumption and evidence based inventory management system, created by him in 2002 was not
followed after his transfer from the said post, and upon his return, nothing remains of the said
system. However, the AMIs hold an adequate procedure for consumption-based requisitioning of
medicines through indents of the ward incharge duly verified by Registrar and counter-verified by
Chief Pharmacist. Indent requisitions from wards are initially based on generic names or INNs
(International Nonproprietary Names) till the time the Ward incharges get acquainted to the brand
names selected for the particular year.
Consumption Reporting of Medicines:
Except for the AMIs and DHQs, no daily, weekly or monthly consumption reporting of the medicines
by the subsequent health facility/end-user was observed in any of the EDOs (Health) or Vertical
Programs. AMIs & DHQs have an appreciable mechanism of reporting back to the wards the
inventory of dead items (pharmaceutical products not requisitioned since long by wards and liable to
get expired) at their regular Stores.
Physical Verification of Stocks:
Physical stock is verified internally on need-basis or on quarterly basis. AMIs like LRH and KTH
have different stores e.g., Regular Store (for receipt of medicines etc), Issue Store (for issuing
medicines to wards), Local Purchase Store (for purchasing non-Govt MCC medicines or short-
94
stock), General Store (for receipt and issue of general items/linen/surgical disposables etc.), A&E
Store (for purchasing accidents and emergency medicines) and C&W Store (for maintenance items
etc). The blank carton / packing of the medicines is later reconciled with those issued to the wards.
The Indent register kept by the chief Pharmacist is therefore reconciled with the Expense Register
kept by the Ward Incharge Nurse. Annual external audit is also conducted with observations usually
on non-prescribed methods of stacking the medicines. As informed by the AMIs, the pilferage of
medicines may take place at the level of wards as the patient is not available to participate in any
reconciliation exercise, or may take place at the level of the distributer who in the garb of supplier,
gets the stock from the manufacturer and sells the expensive medicines in the open market at half
of the Govt-MCC controlled rate.
95
7. Section: III Assessment of Identified Risks & Their Mitigation Strategies:
The assessment of the procurement system of the Health Department by using the above stated
BLIs, has revealed the following risks which are assessed here with suggestions on their mitigation.
The assessment also includes some risks identified by the Fiduciary Risk Assessment (FRA) of
health sector of Khyber Pakhtunkhwa PK earlier this year. Risks are categorized accordingly as
High, medium and low risks in terms of their impact on the procurement system, organizational
responsibility and probability of occurrence.
7.1 Regulatory Risks
1. Risk: Absence of Regulatory Framework for the Provincial Procurement System
There is no overseeing Public Procurement Authority in the Province and the existing NWFP
Procurement of Goods, Works & Services Rules 2003 are not comprehensive enough to address
all competitive procurement methods like Single Envelop Single Stage Bidding and Two Stage
Two Envelop Bidding methods.
Impact: High Probability of Occurrence: Low
Mitigation strategy: The Khyber Pakhtunkhwa Public Procurement Regulatory Authority 2012 has
been enacted by the Provincial Assembly but the Public Procurement Rules are pending
notification by the Provincial Government. Establishment of a KP Public Procurement Regulatory
Authority (PPRA) will lead to strengthening of a competitive Provincial procurement rgime. In this
regard, a Health Sector Procurement Supplement containing supporting regulations, sector-specific
Bid Evaluation Guidelines, User Notes and Standard contract templates etc on public procurement
customized to the specific health-sector requirements may be prepared and appended to the
expected Khyber Pakhtunkhwa PPRA Rules 2012 and named as Health Sector Supplement to
Khyber Pakhtunkhwa Public Procurement Rules 2012 (HSKP PPRA) to be read in line with the
allied laws and Sector-driven specifications for procurement of Drugs, Medicines and Bio-Medical
Equipment. TRF may contribute towards preparing a Health Sector Procurement Supplement for
DGHS KP if desired.
2. Risk: Weak Grievance Redressal mechanism leading to lack of oversight
As observed from the prevalent practice in DGHS KP, no specified Grievance Redressal
mechanism exists. Furthermore, the aggrieved parties do not find the environment conducive for
lodging any complaint perceiving possible backlash from the Department. This has seriously
compromised the monitoring capacity of the Department to address such issues.
Impact: High Probability of Occurrence: High
Mitigation strategy: Weak Grievance Redressal mechanism is being replaced by the Khyber
Pakhtunkhwa Public Procurement Regulatory Authority Bill 2012 containing a robust Grievance
Redressal mechanism. This mechanism seems independent of DoH KP to ensure transparency and
has two tiers of grievance redressal, one at the level of Procuring Entity (as earlier existed) and the
other at the level of KP Public Procurement Regulatory Authority. Counter-review in the form of an
appellate tribunal is still a missing goal for the Department.
96
3. Risk: Inadequate Need Assessment by Districts for Budgetary Allocations for the Bio-
medical equipment & pharmaceutical products.
Yearly centralized procurement of bio-medical equipment is done in order to utilize the ADP
Schemes for various Health facilities in the Province but Departmental inspection of the said
equipment is not conducted for months to check installation and subsequent operationalization.
This shows unnecessary purchases and results in stacking of packed equipment collecting dust in
the health facilities. The payments to the suppliers are therefore considerably delayed. Selection
of drugs on unit rates by the Govt-MCC is also to be completed from 31
st
July to 30
th
June for
District Health entities including DHQs, THQs and RHQs where less expensive drugs are bought
but more volume is involved. In the absence of any Annual Procurement Plan, quarterly purchase
lists are consolidated by the EDOs (Health) and instead of buying in each quarter due to small or
variable amount of funds disbursed for basic medicines, purchasing is done by them on bi-yearly
or three-quarterly basis to make the lumpsum purchases with more funds. This sometimes leads
to shortage of medicines at Districts at a particular time. The same exercise is carried out at
Teaching Hospitals and becomes an acute problem where lives saving drugs are required.
Historical pattern of a medicines purchase cycle is not being followed
Impact: High Probability of Occurrence: High
Mitigation Strategy: DGHS needs to call for estimates of yearly requirements in advance based on
previous years trends for pharmaceutical products, Bio-medical equipment and medical supplies
from all the EDOs (Health) to formalize the total annual estimates against the budgetary allocations.
The Procurement Cell at DGHS in collaboration with Govt-MCC may continue centralized
acquisition of bio-medical equipment and selection of drugs on unit rates for all the District procuring
entities, based on yearly estimates provided by the EDOs (Health).
4. Risk: Absence of Sector-specific Guidelines
It was observed that any Sector-specific guidelines read in conjunction with NWFP Procurement
Rules 2003 and Drug Act 1976 were not available. The current procurement practices are being
carried out in the Province without identifying the Sector Specialists for the Bio-Medical
equipment, Drugs (General & Specialized), Surgical Disposables and medical furniture.
Consequently, they are not involved in framing the relevant technical specifications, acquisition
guidelines and the above stated regulations.
Impact: High Probability of Occurrence: Moderate
Mitigation Strategy: Health Sector specific guidelines in conjunction with relevant procurement
rules and Drug Act 1976 may be developed in consultation with the available Sector Specialists at
DGHS KP which may become a part of expected PPRA Rules 2012 through a Supplement
suggested above.
97
5. Risk: Unauthorized Extension in Drug Pricing by DGHS
Whereas the medicine prices are valid from 31
st
July to 30
th
June in a financial year as acquired
through centralized rate contracting via open competition at Govt-MCC, often without getting prior
permission from the selected suppliers the Directorate General Health Services extends the
prices of drugs and surgical disposables upto another three to six months as has been done till
30
th
November 2012. Though it may be beneficial to the Department to acquire products at old
rates, in anticipation to such events the pharmaceutical manufacturers may load their prices at
the outset thereby creating an undesirable price increase.
Impact: Low Probability of Occurrence: Moderate
Mitigation Strategy: Regulations regarding limitation on extension in purchasing time should be
enacted by the DGHS through administrative notification & and future procurements may be
planned well ahead of the annual milestones.
6. Risk: Internal Audit not available
Internal Audit mechanism for procurement activities is totally lacking. This has also jeopardized
the potential of the Health Department to evaluate the existing procurement procedures. Further,
repair, maintenance and POL heads utilized by the District procuring entities are not being
properly audited. Donor transferred equipment including vehicles, furniture and other assets are
also not being recorded against any Departmental inventory list. As there is no internal audit
mechanism to monitor the procured assets during the Project Closure phase, adherence to
internal controls for safeguarding such assets is not possible.
Impact: High Probability of Occurrence: High
Mitigation Strategy: Internal Audit functions need to be established in DoH KP as an inherently
governmental function and has to be carried by the state functionaries from within the DoH KP. A
short training/capacity building on Procurement Audit is intended to be conducted by TRF as
indicated in the Training Calendar annexed herewith for the procurement officials of DGHS KP and
Health Secretariat, KP.
Districts visits may be needed to gauge the magnitude of such asset transfers and related inventory
management. Similarly, internal audit mechanisms need to be introduced for the repair,
maintenance and POL. Inventory management system may also be designed. TRF has submitted
draft TORs for a proposed TA to Director General Health Services in this regard. To build capacity
on Assets Management for audit verification purposes, a formal training on Inventory &
Warehousing Management is intended to be carried out as indicated in the Training Calendar for
DGHS KP for the procurement officials of DGHS, AMIs & Vertical Programs.
7. Risk: Consultant Guidelines & Consultancy requirements not available
It was also observed that no definite guidelines for consultants were available with the Health
Department. There was also no governing law which required or created the need for hiring a
consultant. Any need analysis in this regard by the Department was also missing.
Impact: Moderate Probability of Occurrence: Low
98
Mitigation Strategy: TRF has provided its Manual on Hiring of Consultancy Services to the Health
Department. An Interdepartmental Consultants Selection Committee (IDCSC) exists at the
Provincial Secretariat level for hiring engineering and design consultants. Related SOPs may be
obtained from them. Federal PPRA Consultancy Guidelines and SOPs may also be introduced for
customizing them to project specific needs at Directorate General Health Services. Consultant Need
Analysis may be done within the policy framework mutually agreed by the DGHS KP and TRF
owing to Departments needs based on various Situational Analyses conducted by TRF thereof.
Health sector specific guidelines for hiring of consultants may therefore be prepared in light of the
above. HSRU has recently adopted World Bank Guidelines on hiring of Consultants which may also
be utilized by the DGHS if required.
TRF Islamabad has conducted a short one-day training on hiring of consultancy services in the
Health Sector for the Health Department, KP on 6
th
November 2012.
8. Conflict in the Governing Law Vs the Federal Law
The NWFP Procurement of Works, Goods & Services Rules 2003 are in conflict with the Federal
PPRA Rules 2004 in many aspects, especially in negotiations on financial bids, which cause
major deviations from standard national and international procurement practices and open the
venue for misuse of public funds.
Impact: High Probability of Occurrence: Moderate
Mitigation Strategy: Khyber Pakhtunkhwa Public Procurement regulatory Authority (PPRA) Act
2012 has been notified vice Provincial Assembly notification on 20.09.2012. The said Authority is
supposed to draft Public Procurement Rules under this Act. The World Bank has already got the
said Public Procurement Rules drafted by a management consultancy firm in 2008 which are in line
with the Federal Public Procurement Rules 2004. The Provincial Government has to notify the said
draft Rules to replace the existing NWFP Procurement of Goods, Works & Services Rules 2003.
Subsequent to it any substantial conflict between Federal and Provincial procurement practices is
expected to be reduced. In the meanwhile, international best practices on procurement under NCB
may be adhered to while executing procurements at DGHS KP and avoiding the conflicting
procurement provisions by DoH KP. The international best practices on procurement under NCB
are now being followed in the revised Standard Bidding Documents for procurement of Drugs.
7.2 Process Risks
Risk 1: Outdated Bidding Documents are still being used
Revised Standard Bidding Documents for the purchase of Bio-Medical Equipment, drugs and
Surgical Disposables at DGHS KP have been introduced under NWFP Procurement of Works,
Goods and Services Rules 2003 but the earlier three-paged traditional Bidding Documents are
still being utilized for procurement of non-drug Surgical Disposables which has created distortion
in the purchasing business processes at the Departmental level.
Impact: High Probability of Occurrence: Moderate
99
Mitigation Strategy: Revised Standard Bidding Documents (SBDs) have been introduced by the
TRF for procurement of Bio-Medical equipment and drugs. Any exclusion in this regard by any
procuring entity of the Health Department may be eliminated to ensure standardization of the
business processes and to bring transparency to the system.
Risk 2: Committee Members are repeated in Subsequent Committees leading to Conflict
of Interest
It was observed that members nominated in the preliminary scrutiny committees for initial profiling
of the technical bids were repeated in the subsequent committees like Comparative Statement
Committee, T&E Committee and Purchase Committee etc. for the same activity. The inherent risk
in such business practices has the potential to amplify the bias of a committee member thereby
vitiating and jeopardizing the integrity of the procurement cycle. The high impact of this risk leads
to a potential conflict of interest.
Impact: High Probability of Occurrence: High
Mitigation Strategy: Members once nominated in a procurement committee may not be nominated
in another procurement committee designated for a subsequent operation in the same procurement
cycle. Any such nominations eventually do not hold validity in the eye of law when challenged owing
to the probability of perpetuation of bias against a particular bidder and thus leading to conflict of
interest. Though the NWFP Procurement Rules 2003 are silent on the issue, Section 11-A of the
Drug Act 1976 provides an inference to avoid such practices. However, members of a procurement
committee may be included in the inspection committee to inspect the supplied bio-medical
equipment or to conduct post-qualification visit to a pharmaceutical manufacturer.
Risk 3: Different Purchase Committees exist for purchase of Bio-Medical equipment &
Chemicals for provincial Hospitals
Different Provincial hospitals have constituted their own Purchase Committees for procuring bio-
medical equipment and laboratory chemicals instead of getting it procured from the DGHS
Procurement Cell which is doing the same exercise for Districts with some expertise available in
procurement functions. This poses a risk of duplication of functions in processes and may lead to
wastage of resources.
Impact: High Probability of Occurrence: Moderate
Mitigation Strategy: All such purchases of bio-medical equipment may be done at DGHS
Procurement Cells level and hospitals purchase committees may be done away with.
7.3 Institutional & Professional Capacity Building Risks
Risk: Restricted application of Revised Standard Bidding Documents due to lack of
expertise
Though revised Standard Bidding Documents (SBDs) have been prepared for the procurement of
medicines and bio-medical equipment, their application may be restricted owing to lack of
professional capacity in terms of development of specifications and evaluation process and
internal resistance from the Department in adopting the new format. The bidders may pose
100
another challenge in accepting the said SBDs out of fear of unknown if frequent awareness
sessions and Pre-Bid Meetings are not conducted to expose them to the new system.
Impact: High Probability of Occurrence: High
Mitigation Strategy: Training not only on PPRA Rules but also on Technical specifications may be
conducted. It may need experts for making agreed benchmarks. Technical Evaluation Guidelines
developed during the evaluation of bids at DGHS KP are being refined to include them in the
proposed Health Sector Procurement Supplement for the Department. Such a document may be
very helpful in the capacity enhancement of the related procurement officials.
Exposure to new Procurement Rules 2012 has already been provided vide the training on the draft
KP PP Rules 2012. An ongoing training program aiming at the capacity enhancement of the
procurement officials of the Health Department KP has been initiated and is expected to be
consisted of 8-10 such trainings till June 2013. Draft PPRA Rules are awaiting notification of the
Provincial Government. Updation of standard procurement documents have already been achieved
through introduction of the revised Standard Bidding Documents for procurement of Drugs and bio-
medical equipment at the DGHS level.
Regular coaching, mentoring and on-job knowledge sharing is being done by the TRF at the
Departmental, District and Program levels in Khyber Pakhtunkhwa while giving procurement support
by guiding on procurement planning, designing of the Standard Bidding Documents, on
participation in Pre-Bid, bid submission and financial bid opening meetings and providing technical
and legal support during bid evaluation.
The following three major areas seek intervention of TRF in the capacity building area for the Health
department KP. In this regard, a Training Calendar addressing the following disciplines has been
prepared for the Health Department.
a) Public Procurement Rules Comparison of international best practices
b) Designing of Standard Bidding Documents and Bid evaluation.
c) Supply Chain of pharmaceutical products including cold chain for biological drugs.
Keeping in view the above capacity needs, the following tentative training modules will therefore be
followed (but not limited to) by TRF KP in consultation with TRF Islamabad:
1) Comparative Assessment of NWFP Procurement Rules 2003 with Federal PPRA
Rules2004 / draft KP PP Rules 2012
2) Procurement Life Cycle
3) Bidding Document Design & Evaluation of pharmaceutical products/bio-medical
equipment
4) Inventory & Warehousing Management
5) Customs Clearance procedures and carrier pricing for Multi-modal Transportation
(Supply Chain) of pharmaceutical products
6) Procurement Audit
7) Contract Management in the Health Sector
101
8) Comparative Contracting Practices in Donor-funded Projects
9) Procurement of Consultancy Services, RFP design and Consultant Evaluation
Involvement of PHSA, Peshawar in Procurement Training: The Provincial Health Services
Academy, located in Peshawar can be made a stakeholder in training on procurement topics as a
part of the health management courses for the health managers. TRF, in collaboration with the
Procurement Cell of Directorate General Health Services, may arrange courses on public
procurement at the PHSA venue by developing master trainers from PHSA to subsequently make
this training stream an integral part of the Health Departments managerial capacity building by the
said Academy.
7.4 Safeguards and Residual risks w.r.t procurement monitoring
Risk: Procurement Monitoring largely remains unattended in the Department
There is no monitoring of the procurement processes to appraise them for their impact on the
efficiency of the Department in the said area.
Impact: High Probability of Occurrence: High
Mitigation Strategy: TRF Islamabad has got approved TORs from DGHS KP for a relevant
consulting exercise on procurement monitoring tools which may address certain aspects of the
residual risks. Initiation of this exercise is expected soon.
7.5 Operational Risks
1. Risk: Expiry of medicines due to absence of dedicated list for life-saving drugs in
Autonomous Medical Institutions (AMIs) / Tertiary Health Institutions:
Though the NWFP Procurement Rules 2003 mention generic names for the goods to be
procured, in case of life saving drugs, it is hardly applicable. It was observed from the record and
feedback of the officials and medical staff of the tertiary Health Institutions e.g., Teaching
hospitals in Peshawar that in instances of severe medical emergencies, locally purchased drugs
were found in-effective and the patients had to be recommended imported medicines from
internationally reputed brands. Both the local and imported brands use the Active Pharmaceutical
Ingredient (API) of the same percentage which may have been ratified during the pre-qualification
process, but the grade of the Pharmaceutical raw material and its source of origin are the
deciding factors for determining a medicines efficacy during treatment and for a life saving drug it
all the more becomes important in the case of a severe medical emergency. This could be
illustrated by an observation by a hospital pharmacist in an AMI in Peshawar that a 10 mg of
Valium from Roche, Switzerland using an A-Grade API immediately relieves the squeaking
patient of his suffering where a local medicine with similar API fails to respond adequately. The
price plays an important role here as the medicine with the same API having lowest price gets
selected as per the prevailing procurement practices. The multi-national drug manufacturers
therefore do not compete due to much low prices offered by the local companies and are thus
restricted by the competition. The local medicines procured in this regard remain unused and
expire thus leading to wastage of public resources.
Impact: High Probability of Occurrence: High
102
Mitigation Strategy: In the case of life saving drugs, open competition may be invited to bring all
the local and multi-national pharmaceutical manufacturers who manufacture the above stated drugs
with the certified A-Grade API raw material imported from OECD countries and certified by Drug
Regulatory Authorities like USFDA, EMA (Western Europe), MHRA UK, TGA Australia and
Swissmedic Switzerland etc. and verification regarding their Certificate of Analysis (COAs), DRA
attestation and import origin to be carried out at the time of post-qualification visits of the firms by
the Department. Open competitive bidding based on Merit Point Evaluation with raw material source
from the above said restricted origins for health-saving medicines is expected to bring desired
product efficacy.
2. Risk: Procurement Planning not available
As no centralized procurement planning is done at DGHS KP level, the related health budget is
usually overstated and duplicated for medicines/bio-medical equipment by various health entities
in the Province. Any supplementary grant thus requested reduces the credibility of the budget.
This creates problems for the release of funding as it is based on creation of commitments
obligated through the budget at a time when public funds are not available.
Impact: High Probability of Occurrence: Moderate
Mitigation Strategy: Quarterly procurement and financial planning may be introduced. An
extensive meeting with the CPO Health Secretariat with the Financial consultant may be required.
3. Risk: Sub-standard Supply Chain
There is no existing standard mechanism for receipt & storage of medicines & bio-medical
equipment at District level. No Just-In-Time (JIT) delivery was observed. Cold chain for supply of
biological products though projected by respective suppliers but is not visible. No healthcare
procurement guidelines are available on procedures for installing, commissioning and handing
over of equipment and their subsequent inspections/quality assurance through after-sales service
& maintenance. Guidelines on storage, inventory management and distribution of medicines are
also not specifically prepared. Traditional supply methods are being used for supply of medicines
to AMIs and Districts which tend to compromise their quality in terms of non-observance of
temperature and movement protocols set by the WHO.
Impact: High Probability of Occurrence: High
Mitigation Strategy: A situational analysis may help in sorting out the weaknesses and suggesting
improvements. This may also recommend introduction of a supply chain management system for
the health sector in KP which involves inventory management also In case the testing of the drugs
or inspection of bio-medical equipment is delayed, the security mechanism for inventory, return &
warranty claims may be introduced as the case may be. The current supply chain consisting of
distribution, storage and inventory management at various health entities has been looked into in
this Report and probable measures have been suggested. TRF has already initiated related TORs
for a Technical Assistance for a detailed Supply Chain Management initiative which has been
approved by the DGHS KP. Activity in this regard is expected to be initiated by TRF Islamabad
soon. Cold chain for supply of biological products has been made mandatory for the suppliers of
specialized products in the revised Standard Bidding Documents for drugs. Related short-term
trainings are being launched for the DGHS, AMIs, Vertical Programs and the Districts by the TRF on
business processes involved in the supply chain.
103
4. Risk: Non-existence of Engineering Estimates or Base-line Price Estimates
Rates are not based on arm-length basis as there are no Engineering Estimates or Baseline Price
estimates for pharmaceutical products or bio-medical equipment. This may become a serious
contractual issue in the wake of lack of pricing for after-sale services where foreign technicians or
similar technical support is involved. From the official documentation, it is not clear that in the
annual budgetary estimates allocations are made and if made where are these amounts spent.
Impact: Moderate Probability of Occurrence: Low
Mitigation Strategy: The Govt-MCC does not conduct any year-wise comprehensive exercise of
constituting Base-line Price Estimates for the purchase of Drugs and Medicines which could be
used while evaluating the prices of drugs and surgical disposables. The Procurement Cell at DGHS
has recently been created and not much was expected from it in conducting any similar exercise for
bio-medical equipment. In the presence of a wide range of price fluctuation for a particular medicine,
there is a probability of selection of an ineffective medicine with more margin of profit, thereby
leading to prospects of corruption in the process. Base-line estimation of drugs and surgical
Disposables may be done before initiation of every procurement activity. Product sampling can be
accompanied with at this stage to check the quality of the drug. Market survey may be done for the
said equipment. This year DGHS intends to conduct market price analysis of the products selected
for Govt-MCC before announcing the centralized unit rates to avoid procurement of any surgical
disposable/medicine at a rate higher than prevalent in the market to avoid audit observation.
5. Risk: No Intimation to companies regarding their failure to Pre-Qualification
Directorate General Health Services does not intimate the pharmaceutical companies which were
not pre-qualified, of the reasons of non-qualifications. The companies get to know about it only at
the moment the list of pre-qualification is released by the Govt-MCC DGHS. This procedure may
lead to exclusion of companies which become victims of personal dislike thereby reducing the
competition.
Impact: High Probability of Occurrence: Moderate
Mitigation Strategy: Policy Guidelines for indicating the firm for reason of its non-qualification in
the Pre-Qualification Process may be prepared by the Department to dispel any such impression.
6. Risk: Exclusion of Pharmaceutical Companies on the basis of annual Pre-Qualification
Pre-Qualification Proforma as developed by the DGHS is an exhaustive Checklist looking at
every aspect of the pharmaceutical manufacturer and supplier. A full-time pre-qualification of a
pharmaceutical manufacturer requires 2-3 hours upon site visit and not more than three such
manufacturers located at different places is possible per day during office hours alongwith one to
two authorized pharmaceutical suppliers in the after-office hours in the evening, thus making it a
maximum of 5 to six such entities per day. However, the record of the DoH KP reflects a pre-
qualification of around 18-25 pharmaceutical units per day which makes this vital exercise
redundant in terms of quality assurance and subsequently the procurement of efficient drugs.
Impact: High Probability of Occurrence: High
104
Mitigation Strategy: If done properly and rigorously, the pre-qualification exercise for bio-medical
suppliers minimizes the need to be conducted annually and the pre-qualification status of the
successful firm may be renewed for three years. The Department was of the view that the
pharmaceutical manufacturing process may require continuous vigilance coupled with surprise visits
to check the production process and quality control of processes and cannot be left unattended for
more than a year. However, it was observed that much time was consumed in the technical
evaluation of a pre-qualified manufacturer of drugs who was eventually disqualified on the basis of a
sub-standard product sample during the technical evaluation of bids for procurement of drugs for
Govt-MCC for the year 2012-13. The Department may do a soul searching in this regard and weigh
the merits of annual pre-qualification of pharmaceutical firm either against their or scheduled post-
qualification visits to their business premises. Un-announced surprise inspections by the Health
Department may also be conducted for all such manufacturers whose product samples have been
rejected on the basis of non-compliance of prescribed physical sampling standards during the
technical bid evaluation for Govt-MCC for the year 2012-13. This may help them improve their
product quality for further participation in the competition. However, regulatory complications may
also be looked into before gaining access to the said business premises.
7. Risk: Illegal Supply Channel by the pharmaceutical companies
As the Peshawar High Court has restricted the Pharmaceutical manufacturers vide Writ Petition
No. 2478/2010 (Daily Mashriq Vs Secretary Health & Others) to supply directly to the DGHS, the
distributors still supply on behalf of the Companies but without any legal cover. The Sales Invoice
is in the name of the companies and the delivery is done by the distributor, thereby leading to a
procurement risk of an undocumented supply chain.
Impact: High Probability of Occurrence: High
Mitigation Strategy: The Department may hold stakeholders meeting with the manufacturers to
solve the issue. In future, pharmaceutical firms regular employees with valid company identification
or salary slips may be allowed to participate in the bidding process.
8. Risk: Program specific Inventory and related specifications were not created
It could not be determined that the technical specifications for the medical equipment mentioned
in the Specifications Inventory available with the Health Department were current and not based
on the earlier equipment purchased a long time ago. Program-specific technical specifications for
medical equipment were also not very visible in the Departments Inventory e.g., a syringe
specified therein for a particular purpose in a specific health program should be categorized
accordingly alongwith its other supplements to make its procurement more program-specific.
Similarly, for drugs and medicines, trend analysis based on disease burden and drug
consumption could have provided region-wise benchmarks for specific medicines inventories.
Some synergy could be developed between DGHS KP and Combined Military Hospital (CMH) for
sharing standards on average patient costs per disease treatment and ancillary costs which could
help in procurement planning.
Impact: High Probability of Occurrence: Moderate
Mitigation Strategy: Although the technical and operational levels of RHQs, THQs and DHQs vary
with respect to the concentration of urban population and exact two counterpart entities do not
match in functionality owing to different geographical locations & disease burdens, three sample
105
lists for the medical equipment and medicines could be categorized for formalizing Inventories of
Technical specifications to become more program-specific for a typical BHQ, THQ and DHQ etc.
These three sample list containing inventories of technical specifications may have a sample Bill of
Quantities (BOQs) for each Heath facility whose details can be modified keeping in view particular
District's requirements. This may make the procurement planning process less time consuming with
the procurement staff when such sample lists are readily available. This can also lead to design the
Bill Of Quantities (BOQs) more comfortably for inclusion in the Standard Bidding Documents.
9. Risk: Absence of End-User Feedback to Gauge Procurement Efficiency
As observed, no customer or end-user feedback from the Health Districts was acquired on regular
basis to assess the supplier performance in terms of product efficacy, timely delivery and
replacement of batches of medicines. This may pose a serious threat in terms of supplier
profiling, lack of which has the potential of compromising the procurement process. The Clinical
Efficacy Form, developed for such type of feedback or reporting from a Departmental whistle-
blower was rarely observed.
Impact: High Probability of Occurrence: High
Mitigation Strategy: Proper mechanism for receipt of Clinical Efficacy Form depicting supplier
performance or lack of performance may be framed to get regular feedback from Procuring entities.
10. Risk: Purchase of lowest Price Bio-Medical Goods with little availability of Spare Parts
and Service Facility
The specifications of the Bio-Medical Equipment are designed in such a way that many vendors
with hardly any service/maintenance facility in Pakistan also become eligible to compete on low
prices and may pose risk of product obsolescence after purchase. The evaluation criteria in the
existing bidding documents for procurement of bio-medical equipment reflect the strength of the
firms technical and financial capabilities but do not emphasize on after-sales services. If the
technical specifications are closely scrutinized, it is revealed that certain items with narrow
specifications have been included to benefit specific suppliers with prearranged incentives.
Impact: High Probability of Occurrence: Moderate
Mitigation Strategy: Marking/weightage for past performance and prolonged Market presence of
the supplier in the Evaluation Criteria may be Included.
11. Risk: Lack of Dedicated Resources to Assess the technical Capabilities of the
Equipment:
The Technical & Evaluation Committee does not assign any dedicated resource during the
technical evaluation for assessing the technical capabilities of a bio-medical equipment, especially
where meta software components are also an integral part of the machinery.
Impact: Moderate Probability of Occurrence: Moderate
Mitigation Strategy: TRF Islamabad may be requested to arrange a similar workshop on
assessment of technical capabilities of bio-medical equipment for bid evaluation purposes as earlier
done commendably on pharmaceutical product specifications.
106
12. Risk: Lack of Ownership of the Procurement Activity conducted by the HSRU, KP:
The DGHS objects to the ongoing outsourcing of integrated health service to management
consulting firms by the HSRU for the six crises-affected districts on the basis of Public Private
Partnership (PPP). Directorate General Health Services is of the view that any such activity has
to be conducted by the Directorate General and not by the HSRU which is a policy & reforms
wing of the Health Department. Lack of ownership by DGHS KP towards such activity may lead
to issues of acquisition of such model, its monitoring and its subsequent roll-out in other health
districts of KP.
Impact: High Probability of Occurrence: High
Mitigation Strategy: Inter-Departmental communication needs to be improved. A communication
strategy may be mutually formulated among the donors, HSRU and DGHS for chalking out the
responsibility of initiating such development components in future.
13. Risk: Absence of Mechanism of Consolidation of Bid Securities issued by the EDO
(Health):
DGHS is not in the knowledge of the receipt of all the Bid Securities furnished by the suppliers to
the Health Districts against individual supplies. This may pose a risk of unaccounted or missing
bid securities, thus leading to a process risk in procurement.
Impact: High Probability of Occurrence: High
Mitigation Strategy: TRF has included in the revised Standard Bidding Documents for
procurement of Drugs & Surgical Disposables the submission and consolidation of all the Bid
Securities and Performance Guarantees at Govt-MCC level at DGHS Peshawar.
14. Risk: Re-Evaluation of Pre-Qualification Criteria during Bid Evaluation consuming
considerable time:
It was observed during the preliminary examination of the technical bids received for procurement
of drugs for Govt-MCC that almost all the business practices relating to characteristics pre-
qualification process were re-assessed consuming lot of precious time. Rule 40 of the NWFP
Procurement of Goods, Works & Services Rules 2003 provides for Two Envelop Tendering in
case of the post-qualification procedure wherein only those aspects of bids need to be evaluated
which could not be assessed earlier. Re-evaluation of Pre-Qualification Criteria during Bid
Evaluation may pose a process risk in procurement cycle.
Impact: Moderate Probability of Occurrence: Low
Mitigation Strategy: Instead of a generalized pre-qualification of pharmaceutical firms, their
technical bids may be evaluated as per specifically designed evaluation criteria relating to raw
material source gradation, API/FPP stability analyses, Quality Control equipment calibration reports,
past performance regarding supply of quoted items, product share and its market presence,
publication of detailed clinical trials in indexed journals of international repute. The Departmental
Inspection committees may then visit the firms rendered technically qualified in the technical
evaluation to inspect the aspects relating to the GMP, Cold Chain, warehousing procedures and
pharmaco-vigilance mechanisms.
107
15. Risk: Reasonable Time not provided to bidders after Pre-Bid Meetings:
It was observed that majority of the bidders in the procurement activity for Govt-MCC for the year
2012-13 submitted irrelevant/unnecessary documents in bulk quantity which, on one hand, shows
the irresponsible and negligent behavior of the bidders and on the other hand, reflects that the
Department did not educate the bidders how to properly fill up the bidding documents and what
documentation should have accompanied their bids. The scrutiny of the said documentation and
sifting out the relevant one consumed considerable time of the Examiners/Evaluators. In this
regard, feedback was received from the majority of the bidders regarding non-communication of
the second Pre-Bid meetings date and time by the Department for amendments and therefore
inadequate time given to them for incorporating the said changes in their bidding documents. As a
result this led to submission of many bids which were not in conformance to the Clients
requirements and the bidders claimed to have no idea what documents were exactly required to
be submitted. This may pose a serious process risk in terms of transparency and procedural non-
compliance.
Impact: High Probability of Occurrence: High
Mitigation Strategy: Sufficient time of atleast five to seven days may be given to the participating
bidders after any Pre-Bid or subsequent Pre-Bid meeting for communicating the said amendments
to bidders through public advertisement so that the bidders may properly incorporate the said
changes in their bidding documents to make them fully responsive to Clients requirements.
16. Risk: Lack of Detailed Evaluation of Technical Bids by the T&E Committee:
It was observed that due to lack of timelines given by the Competent Authority, the T&E
Committee had to briefly peruse the corporate and product snapshots (resulting out of the
preliminary screening of the technically qualified bidders) submitted by the Preliminary Scrutiny
Committee on the same day when the financial bids were being opened. Not giving enough time
for detailed evaluation of the technical bids may lead to inadequate processing by the T&E
Committees technical experts/professionals, of the technical aspects indicated by the Preliminary
Scrutiny Committee and may lead to subsequent process infirmities and omissions related to
product quality assurance.
Impact: High Probability of Occurrence: High
Mitigation Strategy: The unresolved technical aspects indicated by the Preliminary Scrutiny
Committee always need to be carefully examined in detail by the technical experts included in the
T&E Committee for taking concrete and informed decisions on them. The technical experts included
in the T&E Committee are senior surgeons who can assess the quality of sutures/catguts/surgical
disposables, hepatologists who can assess the SVR Studies for Interferon Therapy for Hepatitis
B&C & other biological vaccines, professors of medicines and senior pharmacists who can assess
the pharmaceutical product efficacy and its impact on patients, and bio-medical engineers to gauge
the performance of an equipment against its functional and conformance specifications. Leaving
the areas indicated by the Preliminary Scrutiny Committee unaddressed by the T&E Committee due
to paucity of time may compromise the quality of evaluation. The planning of the procurement life
cycle may be done in such a way that T&E Committee gets enough time to conduct the detailed
examination of the technical bids. The administrative SOPs issued by the Department may
108
determine the minimum number of days required by the T&E Committee to perform its specialized
functions accordingly.
17. Risk: Amendments in the Standard Bidding Documents by Competent Authority:
It was observed that amendment in the Standard Bidding Documents were usually not done by
the Competent Authority as per the Standard Operating Procedures.
Impact: High Probability of Occurrence: High
Mitigation Strategy: The administrative SOPs may be followed so that proper procedures
regarding transparency and fair practices in procurement may be executed by the Department.
109
8. Section:IV Spend Analysis of Health-Sector Procurement:
Review of past years of Health procurement statistics and the new fiscal environment reveals
greater volumes of responsibility and load that will be placed on the healthcare procurements of in
years to come.
The statistics of the last three years in Table 8.1 reveals that the final grants could not be fully
utilized by the Health Department, either due to squeezed timelines or less than accurate estimation
of the budgetary appropriations. However, the most important trend seen here is the significant two-
fold increase from 2009-10 to 2-11-12 in the health budget for procurements which shows a greater
responsibility for the Health Department.
Table:8.1
Comparison of Current Budget spending with Development Budget for the Years 2009-12
Table 8.2 shows that the pharmaceutical products including drugs and surgical disposables keep on
getting the biggest share in procurement spending during the last three years and require more
transparency in procedures to bring best value for money.
2009-10 (Rs in Million) 2010-11 (Rs in Million) 2011-12 (Rs in Million)
Total
Budget of
the KP
Province
Health
Departmen
t Budget
%Age
Share
Total
Budget of
the KP
Province
Health
Departmen
t Budget
%Age
Share
Total
Budget
of the KP
Province
Health
Department
Budget
%Age
Share
A - Current
Revenue
Budget
80,000 4,024.8 5.03 127,958 5,940.7 4.64 149,000 7,837.25 5.26
B -
Development
Budget
49,815.22 6,167.05 12.38 67,783.68 7,364.79 10.87 83,621 7,825.11 9.36
Provincial
ADP
32,546.412 4,333.87 13.32 58,500.00 6,571.24 11.23 71,542.4 6,467 9.04
Special
Program
/PSDP
10,624.48 1,586.68 14.93 0.000 0.000 0.00 0.000 0.000 0.00
Foreign
Project
Assistance
6,644.32 246.50 3.71 9,283.68 793.54 8.55 12,078.6 1,358.11 11.24
TOTAL
A + B
129,815.22 10,191.8 7.85 195,741.7 13,305.5 6.80 232,62 15,662.36 6.73
110
The estimated and actual expenditures, mentioned in Table 8.3, on account of medicines and
other stores indicate that the districts get separate funding for the pharmaceutical products and
bio-medical equipment apart from the Provincial funding the current budget.
Table 8.2
Budgets allocated for the Purchase of Drugs & Bio-Medical Equipment for the Years 2009-
12 for all District Governments and the Provincial Government.
Expenditure Heads 2009-10 2010-11 2011-12
All District Governments 244,525,407 368,877,723 349,059,040
A03927-purchase of drug and medicines 110,554,182 100,423,840 99,350,800
A03942-Cost of other stores 126,116,002 201,791,583 191,559,690
A03970-Others 7,412,273 65,969,270 57,547,820
A09404-Medical and laboratory equipment 187,200 315,010 246,010
A09409-Medical stocks 62,150 87,010 95,710
A09410-Life saving medical supplies 0 0
A09411-General utility chemicals 65,200 108,010 91,010
A09412-Specific utility chemicals 60,200 100,000 85,000
A09413-Drapery, fabrics, clothing and allied 55,200 65,000 65,000
A09470-Others 13,000 18,000 18,000
Provincial government 280,949,240 379,145,400 481,855,920
A03927-Purchase of drug and medicines 27,633,100 118,293,000 132,003,000
A03942-Cost of other stores 50,204,270 52,622,600 34,962,960
A03970-Others 203,111,870 208,229,800 314,889,960
A09470-Others 0
Grand Total 525,474,647 748,023,123 830,914,960
111
Table 8.3:
Provincial vs District Budget Estimates & Actual Expenditure for the Year 2012-13
Object Head
2012-13
Provincial Districts TOTAL
Budget
Estimates
Actuals
Budget
Estimates
Actuals
Budget
Estimates.
Actuals
A03927
PURCHASE OF
DRUG AND
MEDICINES
113,730,900 34,417,285 176,192,710 100,813,063 214,543,963 135,230,348
A03942 COST OF
OTHER STORES
866,267,000 35,286,474 222,437,120 20,897,456 887,164,456 56,183,930
TOTAL 979,997,900 69,703,759 398,629,830 121,710,519 1,101,708,419 191,414,278
112
9. Section: V Recommendations on Institutional Measures
The subject Procurement System Assessment has helped in identifying various types of risks
emerging out of the Procurement System of the Health Department Khyber Pakhtunkhwa. These
risks may have the potential to compromise the quality and integrity of the System with varied
strengths and probability of occurrence. The following actions as suggested, may lead to mitigate
the said risks if adopted through institutional mechanisms:
9.1: Formulation of a Health Sector Procurement Manual as a Supplement to Khyber
Pakhtunkhwa Public Procurement Rules 2012:
The expected Khyber Pakhtunkhwa PPRA Rules 2012 give broad outlines of public procurement
processes and do not give much detail of the processes. The Mitigation Strategies for the
regulatory, operational and process risks can therefore be incorporated in the proposed Manual
which may supplement and support the administrative regulations, and may contain operational
procedures based on revised business processes, revised time-thresholds for payments, Standard
Bidding Documents evaluation guidelines, benchmarks for technical specifications of the products,
and User Notes on various stages of the public procurement lifecycle customized to the specific
health-sector requirements and to be read in conjunction with the expected Khyber Pakhtunkhwa
PPRA Rules 2012.
Though such a Manual requires another significant effort from the Health Department for its
notification and implementation from the Government, its benefits may outweigh the level of effort
involved. The document may provide the customized environment for the Health sector-specific
procurements and benchmarks for utilizing them in drafting evaluation criteria for the Standard
Bidding Documents.
The proposed Procurement Manual may provide for inviting to the open competition all the local and
multi-national pharmaceutical manufacturers/importers to offer quotes for life-saving drugs prepared
with the A-Grade raw materials (API/Excepients) obtained or imported from OECD countries and
duly certified by the WHO, USFDA and EU-EMA quality assurance standards. In the light of the
Drugs Act 1976 and any recent technological advancements, the drugs may also be defined and
specified in more detail and made part of the proposed Manual alongwith the Formulary. The
Manual may further contain conformance benchmarks based on industrial quality assurance
standards for bio-medical equipment by USFDA, EUs CE-EMA or Japans JIS Industrial Standards,
performance benchmarks set by global certification bodies like Association for the Advancement of
Medical Instrumentation (AAMI), International Certification Commission (ICC), the United States
Certification Commission (USCC), the ISO and international training and certification benchmarks
for Bio-Medical Equipment Technicians (BMETs) e.g., CCE, CBET, CRES and CLES Certifications
etc.
The expected Khyber Pakhtunkhwa Public Procurement Rules 2013 apparently do not have any
provision for central rate contracting for pharmaceutical products as currently being practiced by the
Health Department. The Health Department may therefore need to devise a workable purchasing
strategy by incorporating in the proposed Manual the provisions for Single Stage Two Envelop
Bidding method with a specified year-long fixed price contracting period. For bio-medical equipment,
the Single Stage Two Envelop Bidding method can easily be the one-time purchasing method. The
113
said bidding method will conduct merit point scoring on technical and financial bids with specified
percentages for price and non-price factors for both pharmaceutical products and bio-medical
equipments.
The proposed Procurement Manual may further contain provisions relating to the integrity pact,
code of ethics and potential conflict of interest to prevent Departmental committee members to get
repeatedly nominated in subsequent committees in the preceding related assignment or same
procurement activity. Apart from the institutional measures indicated above, the Health Department
may propose more measures to fill certain process gaps it feels are required in the smooth running
of a transparent and fair mechanism for the purchasing functions. A Model Procurement
Supplement for Health Sector may be prepared by the TRF if the Department desires so.
9.2: Strengthening of Procurement Cell at Directorate General Health Services:
The Health Department has already established a Procurement Cell in the building of Directorate
General Health Services, Peshawar. Necessary administrative notification has also been done in
this regard. However, the staffing for the procurement functions is minimal and below the mark
showing negligence towards this very vital section which performs centralized procurements for the
bio-medical equipment on the basis of requirements sent by the districts. The Procurement Cell
may further be strengthened by merging into it both the Govt-MCC Section and the Pre-Qualification
Cell at the DGHS level. The Cell may be entrusted with the following functions:
i) Procurement of bio-medical equipment, pharmaceutical products, drug and non-drug
Surgical disposables on the fixed price annual central rate contracting basis using Single
Stage Two Envelop Bidding Method
ii) Initiation of the pre-qualification proceedings from a centralized location for central rate
contracting with the merger of the Govt-MCC Section and the Pre-Qualification Cell and
their subsequent association with the Procurement Cell in a more coordinated way.
iii) Planning and estimation functions for purchase of drugs by the Procurement Cell for
making annual Procurement Plan and designing the Standard Bidding documents
accordingly. Since the local governments after the devolution of powers have been
allowed to handle health care in the Districts, appropriation and disbursement of related
budgetary sums are sometimes not conveyed to the DGHS for their sanction by the
EDOs. The said sanction may be made obligatory for the Districts alongwith transmission
of consumption figures so that the Procurement Cell may use them for estimation and
planning.
iv) Development of technical, legal and commercial standards for health procurements for all
the health sector entities in the form of the Standard Bidding Documents (SBDs), Product
Vocabularies (PV) for bio-medical equipment based on conformance specifications
(relating to technological aspects ) and performance specifications (relating to functional
aspects).
v) Development of supply Chain/Cold Chain Guidelines for the medicines /biological drugs
/vaccines as per WHO standards and SOPs for their storage and distribution to various
desired locations.
114
vi) Training & Capacity Building of officials handling procurements in the DGHS, AMIs,
Vertical Programs and Districts on the specified topics on monthly basis through short-
term workshops and dedicated technical sessions. Awareness seminars for the
pharmaceutical firms and suppliers of bio-medical suppliers pre-qualified with DGHS
Khyber Pakhtunkhwa may also be arranged by the Procurement Cell for submitting
responsive bids in a reasonable way.
vii) To assist Director General Health Services in the matters relating to co-ordination and
liaison with other Provincial bodies/departments related to procurements and facilitation
of various policies and regulations that directly or indirectly effect procurement.
viii) Coordinate with Provincial Health Services Academy for arranging lectures on public
procurement for the purchasing officials of the DGHS.
ix) Conduct market survey for all the selected products which emerged as the lowest in the
CS Statement in order to check whether the suppliers have quoted them above the
market prices. Annual market survey of the tentative market prices may also be
conducted for helping the Planning Cell, Health Secretariat in the budgetary estimations.
9.3: Utilization of a dedicated web-portal for the Health Department:
Instead of using EPI Vertical Programs web-site, the Health Department Khyber Pakhtunkhwa may
utilize its own dedicated web-portal for not only posting of IFBs, SBDs or evaluation results but also
online verification of suppliers through their corporate profiles. Currently, there exists a Tenders
tab on the Health department website which has recently been used only for posting the Standard
Bidding Documents for procurement of cancer medicines for Begum Nusrat Bhutto Oncology
Services, Khyber Pakhtunkhwa. The said web-link can further be designed as per the Indian
Directorate General of Supplies and Disposals (DGS&D) (http://www.dgsnd.gov.in/). The Indian
DG&S conducts e-procurements through framework agreements and re-ordering of selected
products. Provincial Procurement regulations are silent on e-procurements or procurements
conducted through dedicated web-portals. However, it also does not bar this option as well. The
DGHS Khyber Pakhtunkhwa, as a start, through its dedicated web-portal may allow the bidders to
submit majority of his secondary documentation online to reduce paper work and submit product
and corporate data in the customized proformas available online. The Client then may score against
the same on the EDI online after perusal and verification of the said documentation and generating
the profile through content management. The in-built procurement monitoring tools may also gauge
the procedural compliance at all steps of the procurement life cycle. Subsequently, District
procuring entities may do on-line re-ordering of products selected by the DGHS through central rate
contracting. This may create logs of the Purchase Orders of all the procuring entities which may
help the DGHS to calculate the total annual quantity of pharmaceuticals purchased during the year.
In future, the said function may be extended to an entire e-procurement based on framework
agreements scenario thereby reducing almost 70% paper work and creating automated record of
purchases. In this regard, a contract lifecycle Management software can be acquired for creating a
customized environment through configuration of prevalent business processes on procurement
and contract management for the Health Department purchasing activities. The said mechanism
has been discussed in detail in the functions of the Technical Wing of the proposed Procurement
Cell later in the discussion.
115
9.4: Human Resource Management:
i) Regular Trainings on Procurement Management to Procurement Entities:
Professional capacity building of all the concerned EDOs (Health), MS DHQs, Chief
Executives of AMIs, Medical Superintendents of DHQs, Principals of Medical Colleges,
Program Coordinators of the Vertical Programs, Senior Hospital pharmacists, P&D
Department & Finance Department GoKP, and senior officials from Health Secretariat,
HSRU and FATA be carried out primarily on basic to intermediate level training modules
based on regulatory and conceptual frameworks with topics like overview of NWFP
Procurement Rules 2003, Khyber Pakhtunkhwa Public Procurement Rules 2012 and
Procurement Life Cycle and then extending the said capacity building towards advanced
and technical ones based on topics like bidding documents development/design, bid
evaluation for procurement of pharmaceutical products/bio-medical equipment and
consultant selection for hiring of management services etc. The related health officials
conducting or supervising procurement activities further be exposed to modules like
Procurement Audit so that they may safeguard their actions by avoiding the typical
mistakes usually committed during the execution of contract actions. A bi-monthly
Training Calendar for the Health Department is annexed which provides various training
modules and short-term workshops both for basic and advanced levels.
ii) Technical Soundness of Procurement Officials: The officials and the staff selected for
the Logistics & Procurement Cell may preferably may be from the existing HR strength
that has earlier been involved in procurement and has been trained on it or may be
outsourced as per the regulatory policy of the Health Department keeping in view the
reflected needs. However the officials hired should be technically sound in their
respective areas as they shall be consulted on technical matters by the Department and
other allied agencies in formulating procurement procedures & policies. Preferably,
certifications on respective contract management, technical and financial skills should be
sought from the candidates for these proposed posts.
ii) Projectized Remuneration: Prospects of a projectized remuneration to the officials of
the Procurement Cell may help in retaining them in the Cell for a longer period of time and
may help them in keeping their integrity intact. It was observed that during the current
evaluation of the technical bids for procurement of drugs for Govt-MCC, the Health
Department retained the Preliminary Scrutiny Committee members in the subsequent
Comparative Statement (CS) Committee for preparation of the Comparative Statement
(CS) in order to keep the evaluation process and resulting prices confidential. The
authorities seemed apprehensive to change the composition of the Committee members
and did not expand it by adding any dedicated KPO skilled in data entry operation. This
consumed considerable time of the Department as the nominated members did not have
enough data entry speed required to punch-in the names and prices of a large volume of
pharmaceutical entities. On one hand it led to conflict of interest by continuing same
members in consecutive committees and on the other side it exposed the issues relating
to integrity of the staff. World-over, projectized remuneration or honoraria in the form of
project allowance for particular projectized assignments are the norm of the day as
these attract skilled personnel and tend to preserve his integrity. DGHS Procurement Cell
116
may be geared towards conducting projectized activities regarding procurement of bio-
medical equipment and pharmaceutical products.
iii) Merit Point Evaluation under Single Stage Two Envelope bidding process;
The Health Department intends to conduct Single Stage Two Envelope bidding process
In the next round of bidding for the year 2013-14 for procurement of drugs for Govt-MCC.
The said contracting methodology involves cumulative scoring based on price and non-
price factors for both the quality and the price for the medicines & bio-medical equipment.
This methodology involves considerable amount of time in calculating the said scores for
around 700 medicines with varied dosages, strengths and formations extending to around
their 3000 pharmaceutical variants next year as well. It may therefore only be adopted if
the DGHS has a dedicated team of two to three pharmaceutical experts, each
accompanied by a skilled data entry operator with proficient typing speed, soft data is
obtained from the bidders to reduce data entry and that the bidding process is initiated
well in time.
9.5: Inventory & Warehousing Management:
The current situation of Inventory and Warehousing management is far below the required WHO
standards. Instead of re-inventing the wheel, the computerized Inventory Management software
currently utilized by the Hayatabad Medical Complex (HMC) Peshawar may be replicated in all
other medical institutions which may provide a streamlined platform for homogenized
interconnectivity among the health entities.
9.6: Proposed Mission of Procurement Cell
Keeping in view the above stated recommendations, the Mission of the DGHS Procurement Cell
may therefore focus on five key areas
Mission:
1. Advocacy: Procurement Cell shall work collaboratively with all legislative and regulatory
authorities to ensure fair and efficient procurement practices in an open and competitive
market within the health industry.
2. Education: Procurement Cell shall provide educational opportunities designed to improve
efficiencies in the purchase, sale and utilization of all goods and services within the health
industry.
3. Ethics: Procurement Cell shall uphold the ethical conduct of business practices within the
industry and the standards adopted by the Govt. of Khyber Pakhtunkhwa and other donor
agencies for Healthcare that are intended to strengthen the integrity of the health care
supply chain.
4. Information: Procurement Cell shall enhance the awareness to all procuring institutions
that fall under the Health Department Khyber Pakhtunkhwa to support the delivery of high-
quality, cost effective health care.
117
5. Liaison: Procurement Cell shall promote meaningful dialogue between health industry
organizations engaged in purchasing and other related industry entities on issues of mutual
interest of procurement
9.7: Proposed Administrative Structure of Procurement Cell, DGHS, Khyber Pakhtunkhwa:
The Procurement Cell in the Directorate General Health Services (DGHS) has already been created
vide DGHS Notification No. 10760-67/Personnel, dated 30.12.2011 and is supposed to purchase
bio-medical equipment and occasional non-Govt-MCC drugs on the basis of requirements sent by
the Health Districts and DHQs.
As per the said notification, the Cell is headed by a Deputy Director (Admn) and manned by an
Assistant Director (Admn), Superintendent Complaint / Coordination Cell DGHS Office,
Superintendent Accounts Section, DGHS and a Computer Operator. The absence of the two top
administrative tiers of the Cell lastly and all of the processing of bidding documents by an office
superintendent single-handedly after the creation of the Cell has rendered its potential significantly
underutilized keeping in view the sensitive functions like requirement-gathering for need
assessment and annual planning, preparation of the technical specifications, and acquisition of best
value for money in procurement of bio-medical equipment and hospital ancillaries etc.
Keeping in view the situational analysis conducted till December 2012, it is proposed that the
Procurement Cell may have the following Wings to utilize its full potential for filling the process gaps:
Pre/Post-Qualification Wing
Technical Wing
Tendering & Coordination Wing
Budget & Planning Wing
The Cell is proposed to be headed by a Director Procurement who will be directly reporting to the
Director General Health Services Khyber Pakhtunkhwa. The Director Procurement should be the
Secretary to the Technical & Evaluation (T&E) Committee of the DGHS and he should have the full
support of the Administration Wing in running the Procurement Cell. For technical matters, the
Director Procurement will be independent and may have appropriate authorization for making
technical decisions with respect to tender evaluation. However the administrative powers may rest
with the Principal Accounting officer of the Department i.e. Secretary Health.
The Procurement Cell may also be expected to ultimately house the procurement officials of the
HSRU who are currently engaged in the hiring of a management consulting firm for outsourcing the
health service delivery to the six crises affected districts of Khyber Pakhtunkhwa and can
subsequently be aligned to work under the Director Procurement, Procurement Cell, DGHS to
increase stakeholders acceptance threshold by the Directorate General Health Services towards
reforms carried out by the HSRU and to add to Procurement Cells professional capacity. Creation
of procurement skills at HSRU and at DGHS may lead to need-based exchange of procurement
personnel within the Department.
Director Procurement will manage the cases of mis-procurements or erroneous bid evaluations and
may refer such cases to the Director General Health Services for sending the same to Secretary
118
Health for administrative decisions. The organizational hierarchy of the Procurement cell is as
under:
Figure-9.7.1: Organizational hierarchy of the Procurement Cell
119
Following is the functional scheme of the Various Wings of Procurement Cell:
Figure-9.7.2: Details of the functions of the Wings in Procurement Cell
The Procurement cell would therefore assist Director General Health Services in the following
matters:
a) Provide technical support to Health Department in carrying out specific procurements
b) Standardize public procurement procedures & SOPs for all provincial health entities
c) Coordination & liaison with other Provincial bodies related to facilitation in procurement
and various policies / regulations affecting procurements.
120
Pre-Qualification Wing:
The organogram of the Pre/Post-Qualification Wing is as under:
Figure-9.7.3: Hierarchy of Pre/Post-Qualification Wing:
This Wing is proposed to come into being as a result of the merger of the Govt-MCC Section and
Pre-Qualification Section currently existing in the Directorate General Health Services (DGHS), and
will be solely responsible for qualifying reliable suppliers (Drug as well as Medical Equipment) who
may then participate in tenders invited by Health Department, Khyber Pakhtunkhwa. The Wing will
also keep a close liaison with the Drug Regulatory Authority of Pakistan (DRAP), Islamabad and
other organizations dealing with Supplier registrations and Quality control.
The officers of this Wing are required to be experienced in administrative as well as technical aspect
of pre/post-qualification of suppliers/manufacturers. It is proposed that at least three officers are
delegated this responsibility and one of these may also head as In-charge Pre/Post-qualification
Wing. These officers may be dedicated to qualitative assessment of suppliers of Pharmaceutical
items, Bio-medical equipment and non-drug surgical instruments/disposables/insecticide/general
items/equipment (eg. Medical/office furniture, Medical gases, Waste management, and spares etc.)
respectively.
121
The area of function of this Wing will be as follows:
The Wing may be aided by all the Pre/Post-Qualification teams who may have visited the firms
applying for Pre/Post-qualification / registration or its renewal.
Following task will be carried out in this aspect:
Maintain Database of Suppliers: All suppliers, manufacturers or importers etc interested in
carrying out business with the Health Department Khyber Pakhtunkhwa will be registered
with this Wing which will maintain complete details of the suppliers in a database. This
database will be frequently distributed among all the procuring entities of the Health
Department, Khyber Pakhtunkhwa.
Conduct Pre -Qualifications: The Wing will use the already well-defined Pre-qualification
procedure to ensure the Good Manufacturing Practices (GMP) either before the tendering
process or may conduct Post-qualification after the opening of technical bids to ascertain the
same so that only quality products from reliable suppliers are considered for selection.
Conduct Post Qualifications: The Wing may maintain all record of the suppliers performance
in terms of their successful contract executions. The Wing may also periodically check on the
pre-qualified / registered suppliers to ensure that they have maintained their quality
standards as were approved at the time of their pre-qualification.
Blacklisting of Suppliers: Any non-compliance or fraud committed by the suppliers at any of
the health entities may be centrally maintained and notified to all concerned, especially to
Registrar Companies or Security Exchange Commission of Pakistan (ESCP). The Wing may
also ensure that any supplier who has been requested for blacklisting/debarred from the
Health Department is judicially investigated and if required, be blacklisted for a minimum of
three years from participating in the DoH tenders. The Wing may also ensure that such
suppliers do not apply for pre-qualification under any new name or organization.
Suppliers Defaults: The Wing may be responsible for investigating any non-compliance of
contract terms once purchase order has been issued to a supplier. The Wing may ensure
that the allegations made are fair and that the supplier is given a fair opportunity to justify the
allegations of default and appropriate action taken. The Wing may also intervene on the
issue and try to resolve it amicably.
Suppliers Grievances: The Wing may be responsible to attend to any of the Suppliers
grievances and to ensure provision of right of audienceto the aggrieved and appropriate
actions recommended that may be formally carried out as per DoH regulations.
Maintenance of Database of Suppliers: The Wing may install and maintain database of the
Health-sector suppliers all-across Pakistan and their products. This information may be used
for monitoring suppliers after-sales services and their product performance for future
reference and to guide any one requiring feedback. The Wing may further liaise with DHIS at
DGHS for through any probable dedicated e-portal offering complete end-to-end Contract
Management automated solution for re-ordering medicines and equipment etc online from
the uppliers selected by the Health Department procuring entities for central rate contracting.
122
Technical Wing:
The organogram of the Pre/Post-Qualification Wing is as under:
Figure-9.7.4: Hierarchy of Technical Wing
This Wing may be responsible for all the technical matters of the product/services. It may comprise
a minimum of two technical persons. The officers of this unit may be professional pharmacists and
biomedical engineer/technicians with appropriate qualification and experience in Hospitals.
The functions of this Wing may be as follows:
Standardization of Products: The Wing may define the products in various categories and
accordingly may establish guidelines for their procurement. Certain regularly-used products
may be standardized for the specific health-entities and formularies may be developed for
each level of health care/programmes and criteria for estimating quantity be set as per
patient loads and seasonal/area disease prevalence.
Technical Specifications: The Wing may formulate, standardize and update technical
specifications of the products for respective categories for medicines as well equipment.
Maintenance of Database of products: The Wing may maintain a comprehensive data of all
products available in the market with particular reference to the ones available in Pakistan
and their suppliers. This may help assist procuring entities to obtain reference of the
possible options available. The said database may be uploaded on the dedicated e-portal for
the automated Contract Management Solution
123
Dedicated Contract Lifecycle Management e-Portal at DGHS: A Contract Lifecycle
Management (CLM) software developed locally and running on a dedicated networking
server at the Procurement Cell, may help the Department to create combined online
purchasing, procedure compliance and procurement monitoring scenario. Any such
enterprise-grade Contract Lifecycle Management (CLM) software may be customized to
meet the requirements of the Procurement Cell, district Procurement Entities (PEs) and
HSRU for:
Customized Drop-down Templates for Assets & Inventory data completion and reporting from
Districts
Assets Management of Bio-Medical Equipment
Inventory Control Management of drugs
Procurement Management of all Health-sector goods & services
Intelligent Contract Management Workflows for contract approval routing, legal terms and
conditions control
Customized Templates for evaluation of bids submitted online to reduce burden of paper-
based tender documentation to 70%
Contract Administration of suppliers & Health-Service Delivery Management firms
Procurement Monitoring Tools embedded in the software for Health Managers to gauge
procedural compliance to the prevalent Provincial Public Procurement Rules
Searchable Contract Database e.g., ECRI-Select Plus & IMS Health for products and their
suppliers and linked to all contract data
Ability to capture images of the primary and secondary documentation submitted alongwith
the bid and subsequent contract
Creation of Vendor Interface on the CLM e-Portal wherein drop-down menus in the Bid
Content Submission Forms customized to the Technical Evaluation Criteria will be provided
so that suppliers may key-in the contents of their documentation bids and upload the
scanned documentation
Creation of Evaluator Interface on the CLM e-Portal wherein evaluators may scrutinize the
data in the Bid Content Submission Forms & attached documentation submitted by the
suppliers/vendors/manufacturers, and subsequent calculation of the highest ranking firm /
Most Economically Advantageous Tender
Generation of Business Intelligence Data Reports for trend-analysis, planning and estimation
of future procurement needs
Technical Comparisons: The Wing may maintain information of the technical comparison and
performance of the products. It may be responsible for developing technical evaluation criteria for
products and carrying out technical evaluations of the bids. The above can be maintained by
acquiring membership of both the ECRI-Select Plus, data base for suppliers / products for bio-
medical equipment and IMS Health, data base for suppliers / products for pharmaceutical products
124
which are international nonprofit global organizations providing access to all medical devices /
technologies and pharmaceutical items respectively along with their manufacturers details,
specifications, unbiased technical comparisons and other relevant details that are very beneficial for
procurement analysis. The proposed Procurement Cell, after getting membership of the said
databases, may utilize the said information, services and technology to facilitate the Departments
evaluators to analyze sales data of Pakistan Pharmaceutical market and to develop future
procurement business strategies.
Installed Base: The Wing may maintain a Health Facility-wise comprehensive installed base
of all the major bio-medical equipment earlier supplied to the Health Department and may
maintain an updated status of the performance of such equipment on periodic basis.
Project Management: The Wing may be the key contact point to coordinate with all Hospital
projects in terms of design, construction and medical equipment planning & procurements.
Tendering & Coordination Wing:
This Wing may have three main functions:
i) Being responsible for carrying out the administrative aspect of the tendering process based
on the Procurement Life Cycle carried out by the DoH.
ii) It may also be the coordination Wing for all Districts, AMI and Programs.
iii) Carry out internal audits of procurement procedures all over Khyber Pakhtunkhwa.
iv) Monitor procedural compliance and oversight as well as to intervene in case of mis-
procurement or any system flaws.
125
Organogram of Technical Wing:
Figure-9.7.5: Tendering & Coordination Wing
It may comprise around three staff members who are appropriately qualified in procurement
procedures and related administrative functions.
The Wing may have 3 core functions which are as under:
a) Tender Administration & Contracts
b) Coordination with Districts
c) Coordination with AMIs and Programs
The Wing may be responsible for all the technical matters of the product/services. It may comprise
of 5-6 technical persons. The officers of this Wing may be professional Pharmacists, Biomedical
Engineers and technicians with appropriate qualification and experience in Hospitals.
126
Tender Administration Function: Following functions may be carried out related to Tender
Administration:
Standard Bidding Documents Preparation & Tendering Process: The Wing may be
responsible for standardizing the bidding documents for various categories of products
and services i.e.,
Pharmaceutical drugs and Surgical Disposables
Medical Equipment & Spare parts.
Ancillary Hospital equipment like medical furniture, CMW/LHV Kits, non-Drug Surgical
disposables, insecticides and other miscellaneous items etc.
Also to prepare guidelines for standard procedures for whole tendering process from
advertisement till award of contract.
Consolidation of tender documents: The Wing may device a checklist for the whole
tendering procedure which may be used by all the procuring bodies as guidelines.
Advertisements: The Wing may be responsible for devising standard advertising format
for tendering to be used uniformly in all over the Province.
Tender Opening: The Wing may device a mechanism and standard procedure for tender
opening and its related regulations in accordance to the applicable regulatory rgime.
Technical Evaluations: The Wing may define procedure for technical evaluation and its
formats. May also coordinate with the technical Wing in obtaining technical evaluation
criteria and obtain technical evaluations from them.
Order Executions: The Wing may define system procedures for purchase order placing
and its execution and provide support to all procuring bodies and Districts in this regards.
Contracts Drafts & Management: The Wing may be responsible for standardization of
contract and guidance for use by other procuring bodies. All matters related to the contract
administration may also be defined, updated and carried out by this Wing for all healthcare
procurement entities in Khyber Pakhtunkhwa. It may also assist them whenever required.
Records: The Wing may maintain all record and documents of the procurement being
carried out in an organized and accessible manner for monitoring and transparency.
Coordination Function: The Wing would be the only point of contact for the Districts, AMIs and
Programs which require any assistance, guidance, clarifications or any other help regarding
procurement system, procedures or documentation issues. The staff in this Wing will coordinate
with the appropriate Wing of the Procurement Cell and obtain the required information and pass on
to the querying institution. The 25 Districts in Khyber Pakhtunkhwa may be divided in three zones or
regions , each having 8 districts and handled by one person.
127
The functional jurisdiction of the Wing would comprise provision of assistance on any of the
following issues:
Suppliers: The Wing would liaise for providing all information on various suppliers, their pre-
qualifications, blacklisting and other information of the suppliers including resolution of their
issues.
Tendering: All support related to tendering procedure, its documentation and contracts.
Technical: To provide all required technical information and support in terms of the technical
specifications and technical comparisons by coordinating with the Technical Wing.
Planning: The Coordination Wing would also assist the Districts and AMIs in proper planning
of their procurements by providing guidelines and support as and when required.
Logistics: To assist the logistics and supply chain.
Oversight Functions: The Wing would also provide oversight to the Health Departments procuring
entities at different stages of procurement lifecycle. It is recommended that the oversight may be
carried out maximum twice during the procurement process:
First oversight may be instituted when a procuring entity is about to issue Standard Bidding
Documents (SBDs), it should seek clearance from the Wing as to the correctness of the said
documents, confirm that the SBDs are being issued to pre-qualified/registered suppliers only
if required by the DGHS, and the Schedule of Requirements with technical specifications
conforms to the requirements of the Client as well as the evaluation criteria and their
application. The procuring entity can only then proceed after receiving an affirmation by the
Wing.
Second oversight may be instituted when the technical evaluation is completed by the
procuring entity and the same is submitted to the this Wing confirming that
This Wing would also act as a central repository of all contracts executed by the Health Department
procuring entities. Supplies should send a copy of their respective bids to this Wing as well, for
record and correlation purpose.
128
Budget & Planning Wing:
The organogram o the Budget & Planning Wing is as under:
Figure-9.7.6: The hierarchy of the Budget & Planning Wing
This Wing may have three main functions:
i) Guidance on procuring institutes with regard to their budgets.
ii) Provision of Guidelines for procurement planning with specific reference to availability of
the budgets.
iii) Management of budgets from procuring institutes for central purchases.
The Wing may comprise of minimum 1 staff member who should be appropriately qualified in
budgeting and finance and related financial management functions.
The Wing may provide following functions:
i) Procurement Planning: The Wing may provide guidelines for procurement planning in
accordance to the cash flow of the budget. These guidelines may be used by all the
procuring institutions.
ii) Budgeting: The Wing may define classifications of budgets for Health care procurements
and maintain these consolidated budgets from all districts, AMI and Programs.
iii) Commercial aspects of tendering: The Wing may formulate policies and guidelines for
various issues like imports, L/C opening and bank payments etc.
iv) Release of payments: The Wing may coordinate with Finance and Audit Department of
Government of Khyber Pakhtunkhwa to expedite timely payments for effective
procurements.
v) Logistics: The Wing may formulate logistic strategies for supplies and guide Districts,
AMIs and Vertical Programs.
129
9.8: Individual Job responsibilities:
It is evident that the staff of the Procurement Cell may be appropriately qualified and experienced in
the relevant areas of the procurement as defined in the Organogram with detailed functions.
Figure-9.8.1: Nature & Requirement of the Individual Job Function
It is recommended that the In-charge of the Procurement Cell may be an officer from the regular
cadres of the civil services with appropriate qualification and experience and well experienced in the
Government working procedures; or he may be outsourced keeping in view his technical
qualifications. However for the rest of the staff in a number of areas technical expertise is critical for
which no compromise should be made for any such position. The Organogram below is reproduced
with indication of Technical and administrative status of the staff that is being placed in the Wings
and sub-units of the Procurement Cell.
Following is the list of positions for which appropriate Job responsibilities have been individually
prepared and are attached under Annexure1 in section 8 of this report:
i. Director Procurement Cell
ii. Pre/Post-Qualification Wing: PQ
(a) In charge PQ
(b) Pre-Qualification Officer PQ-1 (Pharma)
(c) Pre-Qualification Officer PQ-2 (Bio-medical Equipment, Sterilization and ancillary
Hospital Equipment)
iii. Technical Wing: TW
(a) In charge TW
130
(b) Technical Officer TW -1 (Pharma)
(c) Technical Officer TW -2 (Bio-medical Equipment & Spare parts, General and ancillary
Hospital Equipment)
iv. Tendering & Coordination Wing: TC
(a) In charge TC
(b) Tendering Officer TC-1(Tender Administration & Contract Documentation)
(c) Coordination Officer TC-2 (25 districts, AMIs & Vertical Programs)
v. Budget & Finance BF
(a) In charge BF
(b) Planning Officer BF-1
Procurement Cell - Job Responsibilities.
Job Title: Director Procurement Cell
Qualifications: Graduation from an accredited four year college or university with a degree in
Strategic Procurement, Public Health (MPH), MBBS, Law, BPharma/M.Phil
(Pharma), Public Administration, Business Management or a closely related field is
strongly preferred. However, any equivalent combination of education and
experience sufficient to perform job duties may be considered.
May also have following:
CIPS, CFCM, CPPO, IACCM or any certified accreditation in Public Purchasing
required, or ability to obtain such or similar training within first year of
employment through procurement training.
Comprehensive knowledge of Provincial Procurement Rules / Federal PPRA
and other applicable government regulations is required. Knowledge of Donor
Procurement Guidelines would be preferred.
Experience: Minimum five years experience in the Procurement / Contract Management field is
preferred.
Grade: BPS 19 or equivalent
Recruitment: As per Govt Policy
Position type: Administrative / technical for Khyber Pakhtunkhwa Health Department
Jurisdiction: Complete Province
Reports to: For all matters to Director General Health Services, DoH, KP
Direct responsibilities:
1. To work under the direction of the Secretary Health, Govt. of Khyber Pakhtunkhwa
131
2. To be responsible for maintaining the goals, standards, and objectives of the
Procurement Cell in line with the Health care objectives of the Health Department, Govt of
Khyber Pakhtunkhwa.
3. To lead, direct, coordinate, and manage all administrative, technical, contractual and
operational aspects of the tendering process for health care procurements.
4. To train, motivate, coach, develop, and evaluate assigned professional, technical, and
clerical purchasing staff of the Cell for dedicated and best practice professional working.
5. To stay abreast of new processes, technologies, materials, purchasing methods, statutory
requirements and market conditions. Communicate with management on any significant
factors that could affect Provincial Health Procurements.
6. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees, Public officials of Health Department (Districts and
AMI & Programs) and other departments of the provincial Govt. Like Finance, PPRA,
Audit etc.
7. To approve requisitions, purchase orders, procurement expenditures and contracts for the
procurements carried out by the procurement Cell.
8. To manage and ensure timely completion of procurements within the fiscal year and
appropriated budgets.
9. To lead, manage and coach cross-functional teams through the information sharing &
strategic sourcing process.
10. To facilitate team meetings, prepare supporting documentation, conduct market research,
develop market analysis and assist with strategy development for effective and
transparent procurements.
11. To serve as a member of various cooperative and consortium procurement committees
for DoH Khyber Pakhtunkhwa.
12. To serve as lead negotiator for complex technical services/products, professional services
and Hospital projects.
13. To produce written determination for procurement transactions outside the fiduciary levels
(i.e. emergencies) for approval by the Health Department.
14. To ensure discipline and work ethics of all staff of the Procurement Cell and monitor their
performance and professionalism.
15. Attendance at work is an essential function of this position.
Responsibilities through the various Wings of the Procurement Cell:
1. To formulate, obtain, and maintain policies and procedures for the Purchasing System
and Guidelines for Health care procurement for the whole province and thereof to act as
guidance and monitoring of the same.
2. To monitor the budget for procurement and facilitate procurement planning.
132
3. To develop and facilitate training for DDOs of District, AMIs and Programs in purchasing
policies, procedures and system. Thereof to advise and assist other Districts, AMI and
Programs in management of health care purchasing and contract procedures.
4. To ensure that Quality products/service are standardized for effective health care
services.
5. To ensure that all suppliers/manufacturers are well scrutinized and appropriately pre-
qualified for participating in the tenders for Health care procurement in the province.
Thereof to ensure their post qualification status on periodic basis.
6. To direct, advise, and review specifications for projects requiring extensive technical or
professional services or for complex Hospital projects.
7. To manage projects with cross-functional team members, significant challenges with
information availability, technical requirements and financial complexity.
8. To make site visits to suppliers/manufacturers to ensure that their pre-qualification
statuses are maintain as per original submissions for pre-qualifications.
9. To make periodic visits at various sites of supplies to monitor and measure performance
of supplies throughout the province as and when required.
10. To ensure quality standards are met through administration of purchasing complaints and
resolutions provided by the procuring entities of health in the Province of Khyber
Pakhtunkhwa.
11. To manage large-scale centralized purchasing, contract functions and supplies that
require items with unique requirements as to manufacturing, supply, testing, durability, or
quality characteristics.
12. To review and respond to suppliers/manufacturers protests/grievances in a judicious
manner and resolve in timely manner.
13. To measure vendor performance, cancel contract, suspend or implement debarment
proceedings on vendors not meeting performance requirements.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to plan procurement strategies for large scale
acquisition programs or systems.
133
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Power Point, MS Access, electronic
document management, imaging and ability to use procurement software.
Extensive knowledge of contract law and its application to the purchasing process.
Ability to manage and supervise others as team.
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH personnel.
Pre-qualifications Wing - Job Responsibilities.
Job Title: In charge Pre/Post-Qualifications Wing
Qualifications: Graduation from an accredited four year college or university with any equivalent
combination of education and experience i.e., M.Phil (Pharma), BPharma + 5 years
experience, MBBS + MPH, or MBBS + 1 year experience is strongly preferred.
May also have following:
Knowledge of extensive regulatory framework of Drug Laws is required.
Comprehensive knowledge of Provincial Procurement Rules / Federal PPRA and
other applicable government regulations is required. Knowledge of Donor
Procurement Guidelines would be preferred.
Experience: Minimum seven years experience in the field of Drug Laws / public procurement
field with experience of pre/post-qualifications is preferred.
Grade: BPS 18 or equivalent
Recruitment: As per Govt. Policy
Position type: Administrative for Pre-qualification of Suppliers/Manufacturers for Health care
procurement in Khyber Pakhtunkhwa Health Department
Jurisdiction: Complete Province
Reports to: For all matters to In charge of Procurement Cell DoH Khyber Pakhtunkhwa.
Direct responsibilities:
1. To work under the direction of the In charge Procurement Cell DoH Khyber Pakhtunkhwa
2. To be responsible for maintaining the goals, standards, and objectives of the
Suppliers/manufacturers dealing with Procurement Cell in line with the Health care
objectives of the Health Department, Govt. of Khyber Pakhtunkhwa.
3. To lead, direct, coordinate, and manage all technical and operational aspects of the pre-
qualifying Suppliers/manufacturers for Health care procurements.
4. To train, motivate, coach, develop, and evaluate assigned professional, technical, and
clerical purchasing staff of the Procurement Cell for dedicated and best practice
professional working.
134
5. To stay abreast of new processes, technologies, products & materials, statutory
requirements and market conditions in context to suppliers/manufacturers and
communicate with In charge procurement on any significant factors that could affect
quality and reliability of suppliers/manufacturers in Provincial Health Procurements.
6. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the suppliers/manufacturers.
7. To approve Pre-qualifications, post qualifications, debarring/black listing of Suppliers/
manufacturers for the procurements being carried out by the Procurement Cell at
provincial level.
8. To lead, manage and coach cross-functional teams through the information sharing &
strategic sourcing process.
9. To facilitate team meetings, prepare supporting documentation, conduct market research,
develop market analysis and assist with Suppliers/Manufacturers strategy development
for effective procurements.
10. To ensure discipline and work ethics of all staff of the pre-Qualification Wing and monitor
their performance and professionalism.
11. Attendance at work is an essential function of this position.
Responsibilities through the team members of the PQ Wing:
1. To formulate, obtain, and maintain policies and procedures for pre-qualification of
suppliers/manufacturers for the standardized products services to be notified to all
procuring entities of the whole province and thereof to act as guidance and monitoring of
the same.
2. To appropriately pre-qualify quality suppliers/manufacturers after scrutinizing and
issuance of certification for participating in the tenders for Health care procurement in the
province.
3. To follow up of the post qualification status of the suppliers/manufacturers on periodic
basis.
4. To make site visits to suppliers/manufacturers to ensure that their pre-qualification
statuses are maintain as per original submissions for pre-qualifications.
5. To make periodic visits at various sites of supplies to monitor and measure performance
of supplies throughout the province as and when required.
6. To maintain centralized databank of all suppliers/manufacturers and their offered products
services that can be or is being offered for purchasing and supplies [e.g., IMS Data,
ECRI-SelectPlus, Sid4health for NHS, UK or Indian Directorate General of Supplies and
Disposals (DGS&D)]
7. To obtain market information on the Suppliers/manufacturers and their performance and
maintain complete record of the same in the databank.
135
8. To attend, review and respond to suppliers/manufacturers protests/grievances in a judicial
manner and resolve in timely manner.
9. To measure and monitor vendor performance, cancel contract, suspend or implement
debarment proceedings on vendors not meeting performance requirements and ensure
that health care procuring entities are immediately informed thru proper notifications.
10. To maintain install base of all suppliers/manufacturers equipment with updated
performance record and any noncompliance or quality issues.
11. To ensure that a regular updated list of pre-qualified suppliers/manufacturers is sent to all
Health care procuring entities in Khyber Pakhtunkhwa.
12. To have liaison with suppliers/manufacturers associations/bodies and keep updated on
the developments that may affect the pre-qualification criteria of Health Department or the
in general suppliers/manufacturers performance.
13. To assist the Health care procuring entities in issues related to pre-qualification or post
qualification of suppliers/manufacturers.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to evaluate the suppliers/manufacturers for pre-
qualification for procurements being carried out in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Powerpoint, MS Access & electronic
document management.
Extensive knowledge of contract law and its application to the purchasing process.
Ability to manage and supervise others as team.
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH personnel.
Pre-qualifications Wing - Job Responsibilities.
Pre-qualifications Wing - Job Responsibilities.
Job Title: Pre-Qualification Officer - PQ-1(Pharma)
Qualifications: Graduation from an accredited four year college or university in Pharmacy/
Pharmaceutical Sciences, MBBS with atleast one year experience. However, any
136
equivalent combination of education and relevant experience sufficient to perform
job duties may be considered.
Must also have following:
Technical Knowledge of Pharmaceutical manufacturing, processes and Raw
Materials.
Comprehensive knowledge of Pharmaceutical Industry and applicable
International Good Manufacturing Practices/regulations.
Experience: Minimum five years experience in the field of Pharmaceutical procurement or
Industry with experience of pre-qualifications is preferred; or
In case of no Degree in Pharmacy, minimum ten years of experience in the field of
Pharmaceutical procurement or Industry with experience of Pre-Qualifications is
required.
Grade: BPS 17 or above
Recruitment: As per Govt. Policy
Position type: Administrative for Pre/Post-qualification of Pharmaceutical product Suppliers/
Manufacturers for Health care procurement in Khyber Pakhtunkhwa Health
Department
Jurisdiction: Complete Province
Reports to: For all matters to In-charge of Pre-Qualification Wing of Procurement Cell of Khyber
Pakhtunkhwa Health Department.
Direct responsibilities:
1. To work under the direction of the In charge Pre/Post-Qualification Wing of Procurement
Cell Khyber Pakhtunkhwa Health Department.
2. To be responsible for maintaining the goals, standards, and objectives of the pre-
qualification standards of Pharmaceutical Product Suppliers/manufacturers dealing with
Procurement Cell in line with the Health care objectives of the Health Department, Govt.
of Khyber Pakhtunkhwa.
3. To stay abreast of new manufacturing & supply processes, technologies, products &
materials, statutory requirements and market conditions in context to Pharmaceutical
Product including Insecticides suppliers/manufacturers and communicate to the In charge
Pre-qualifications Wing of any significant factors that could affect quality and reliability of
Pharmaceutical Product suppliers/manufacturers in Provincial Health Procurements.
4. To formulate, obtain, and maintain policies and procedures for pre-qualification of
Pharmaceutical Product suppliers/manufacturers for the standardized products & services
137
to be notified to all procuring entities of the whole Province and thereof to act as guidance
and monitoring of the same.
5. To appropriately pre-qualify quality Pharmaceutical Product suppliers/manufacturers after
scrutinizing and issuance of certification for participating in the tenders for Health care
procurement in the province.
6. To follow up of the post qualification status of the suppliers/manufacturers on periodic
basis.
7. To make site visits to suppliers/manufacturers to ensure that their pre-qualification
statuses are maintain as per original submissions for pre-qualifications.
8. To make periodic visits at various sites of supplies to monitor and measure performance
of supplies throughout the province as and when required.
9. To maintain centralized databank of all suppliers/manufacturers and their offered
products services that can be or is being offered for purchasing and supplies. [e.g., IMS
Data, ECRI-SelectPlus, Sid4health for NHS, UK or Indian Directorate General of Supplies
and Disposals (DGS&D)]
10. To obtain market information on the National & International Suppliers/manufacturers of
Pharmaceutical Products operating in Pakistan with regards to their performance and
maintain complete record of the same in the databank.
11. To attend, review and respond to suppliers/manufacturers protests/grievances in a
judicious manner and resolve in timely manner.
12. To measure and monitor vendor performance, cancel contract, suspend or implement
debarment proceedings on vendors not meeting performance requirements and ensure
that health care procuring entities are immediately informed thru proper notifications.
13. To maintain install base of all suppliers/manufacturers equipment with updated
performance record and any noncompliance or quality issues.
14. To ensure that a regular updated list of pre-qualified Pharmaceutical suppliers
/manufacturers is sent to all Healthcare procuring entities in Khyber Pakhtunkhwa.
15. To have liaison with Pharmaceutical Product suppliers/manufacturers associations/bodies
and keep updated on the developments that may affect the pre-qualification criterias of
Health Department or the in general suppliers/manufacturers performance.
16. To assist the Health care procuring entities in issues related to pre-qualification or post
qualification of suppliers/manufacturers.
17. To apply excellent customer service skills, establish and maintain effective working
relationships with the suppliers/manufacturers.
18. To participate /represent Incharge Pre-qualification Wing in meetings, prepare supporting
documentation, conduct market research, develop market analysis and assist with
Pharmaceutical product Suppliers/Manufacturers strategy development for effective
procurements.
138
19. To train, motivate, coach, develop, and evaluate assigned professional, technical, and
clerical staff of the Cell for dedicated and best practice professional working.
20. Attendance at work is an essential function of this position.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to evaluate the suppliers/manufacturers for pre-
qualification for procurements being carried out in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Powerpoint, MS Access & electronic
document management.
Pre-qualifications Wing - Job Responsibilities.
Job Title: Pre-Qualification Officer - PQ-2 (Bio-medical Devices, Consumables & Ancillary
Hospital Equipment)
Qualifications: Graduation from an accredited four year college or university in Biomedical
Engineering, Electronics or physics. However, any equivalent combination of
education and relevant experience sufficient to perform job duties may be
considered.
Must also have following:
Technical Knowledge of Medical Equipment Technologies and their technical
Services issues.
Comprehensive knowledge of Medical Device standards and safety regulations
particularly in context to the Supply and manufacturing.
Experience: Minimum five years experience in the field of Biomedical Engineering Industry with
experience of procurements of Medical Devices is preferred; or
In case of no Degree in Biomedical or Electronics Engineering, Technical Diploma in
Biomedical or Electronics with minimum ten years of experience in the field of
Medical devices Industry and procurements is required.
Grade: BPS 17 or equivalent
Recruitment: As per Govt. Policy
139
Position type: Administrative for Pre-qualification of Medical Equipment Suppliers/ Manufacturers
for Health care procurement in Khyber Pakhtunkhwa Health Department
Jurisdiction: Complete Province
Reports to: For all matters to In-charge of Pre-Qualification Wing of Procurement Cell of
Khyber Pakhtunkhwa Health Department.
Direct responsibilities:
1. To work under the direction of the In charge Pre-Qualification Wing of Procurement Cell
Khyber Pakhtunkhwa Health Department.
2. To be responsible for maintaining the goals, standards, and objectives of the pre-
qualification standards of Medical equipment Suppliers/manufacturers dealing with
Procurement Cell in line with the Health care objectives of the Health Department, Govt.
of Khyber Pakhtunkhwa.
3. To stay abreast of new technologies, products & services, statutory requirements and
market conditions in context to Medical Equipment suppliers/manufacturers and
communicate to the In charge Pre-qualifications Wing of any significant factors that could
affect quality and reliability of medical equipment suppliers/manufacturers in Provincial
Health Procurements.
4. To formulate, obtain, and maintain policies and procedures for pre-qualification of Medical
equipment suppliers/manufacturers for the standardized products & services to be notified
to all procuring entities of the whole province and thereof to act as guidance and
monitoring of the same.
5. To appropriately pre-qualify quality Medical Equipment suppliers/manufacturers after
scrutinizing and issuance of certification for participating in the tenders for Health care
procurement in the province.
6. To follow up of the post qualification status of the suppliers/manufacturers on periodic
basis.
7. To make site visits to suppliers/manufacturers to ensure that their pre-qualification
statuses are maintain as per original submissions for pre-qualifications.
8. To make periodic visits at various sites of supplies to monitor and measure performance
of supplies throughout the province as and when required.
9. To maintain centralized databank of all Medical equipment suppliers/manufacturers and
their offered products services that can be or is being offered for purchasing and supplies.
[e.g., IMS Data, ECRI-SelectPlus, Sid4health for NHS, UK or Indian Directorate General
of Supplies and Disposals (DGS&D)].
10. To obtain market information on the National & International Suppliers/manufacturers of
Medical Equipment operating in Pakistan with regards to their performance and maintain
complete record of the same in the databank.
140
11. To attend, review and respond to suppliers/manufacturers protests/grievances in a judicial
manner and resolve in timely manner.
12. To measure and monitor vendor performance, cancel contract, suspend or implement
debarment proceedings on vendors not meeting performance requirements and ensure
that health care procuring entities are immediately informed thru proper notifications.
13. To maintain install base of all suppliers/manufacturers equipment with updated
performance record and any noncompliance or quality issues.
14. To ensure that a regular updated list of pre-qualified medical Equipment suppliers
/manufacturers is sent to all Healthcare procuring entities in Khyber Pakhtunkhwa.
15. To have liaison with Medical Equipment suppliers/manufacturers associations/ bodies and
keep updated on the developments that may affect the pre-qualification criteria of Health
Department or the in general suppliers/manufacturers performance.
16. To assist the Health care procuring entities in issues related to pre-qualification or post
qualification of suppliers/manufacturers.
17. To apply excellent customer service skills, establish and maintain effective working
relationships with the suppliers/manufacturers.
18. To participate /represent In charge Pre-qualification Wing in meetings, prepare supporting
documentation, conduct market research, develop market analysis and assist with
Medical Equipment Suppliers/Manufacturers strategy development for effective
procurements.
19. To train, motivate, coach, develop, and evaluate assigned professional, technical, and
clerical staff of the Cell for dedicated and best practice professional working.
20. Attendance at work is an essential function of this position.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to evaluate the suppliers/manufacturers for pre-
qualification for procurements being carried out in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Powerpoint, MS Access & electronic
document management.
141
Technical Wing - Job Responsibilities.
Job Title: In charge Technical Wing
Qualifications: Graduation from an accredited four year college or university with a degree in
relevant field (Pharmacy/Biomedical Engineering or Medical technology) or a closely
related field is strongly preferred. However, any equivalent combination of education
and experience sufficient to perform job duties may be considered.
Must also have following:
CIPS or any certified accreditation in Purchasing or Public Purchasing required,
or ability to obtain such within first year of employment.
Comprehensive knowledge of Pharmaceuticals and or Medical electronic devices
is required.
Experience: Minimum five years experience in the industry of Medical Engineering/
Pharmaceuticals with relevant experience of technical aspects of procurements is
preferred.
Grade: BPS 18 or equivalent or M3
Recruitment: As per Govt. Policy
Position type: Technical aspect of Health care Product and their technologies for Health care
procurement in Khyber Pakhtunkhwa Health Department
Jurisdiction: Complete Province
Reports to: For all matters to In charge of the Procurement Cell of Khyber Pakhtunkhwa Health
Deptt.
Direct responsibilities:
1. To work under the direction of the In charge of Procurement Cell Khyber Pakhtunkhwa
Health Deptt
2. To be responsible for maintaining the goals, standards, and objectives of the Products
and services being dealt within the Procurement Cell in line with the Health care
objectives of the Health Department, Govt. of Khyber Pakhtunkhwa.
3. To lead, direct, coordinate, and manage all technical aspects of the Products involved in
Health care procurements.
4. To train, motivate, coach, develop, and evaluate assigned professional, technical, and
clerical purchasing staff of the Cell for dedicated and best practice professional working.
5. To stay abreast of new technologies & materials, techniques and their market conditions
in to products and services and communicate with in charge procurement on any
significant factors that could affect quality and reliability of products/services in Provincial
Health Procurements.
142
6. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the suppliers/manufacturers.
7. To approve technical specification and other technical aspects of products/services for
standardization of products/services for all procurements being carried out by the
procurement entities at provincial level.
8. To lead, manage and coach cross-functional teams through the information sharing &
strategic sourcing process.
9. To facilitate team meetings, prepare supporting documentation, conduct market research,
develop market analysis related to products/services and assist in strategy development
for effective procurements.
10. To ensure discipline and work ethics of all staff of the technical Wing and monitor their
performance and professionalism.
11. Attendance at work is an essential function of this position.
Responsibilities through the team members of the Cell:
1. To formulate, obtain, and maintain policies and procedures for product/services
categorization and standardization in line with the provincial Health care delivery policy at
different level of health care facilities.
2. To notify the same to all procuring entities of the whole province and thereof to act as
guidance and monitoring of the same.
3. To appropriately review and evaluate products/services after scrutinizing and maintaining
a database of products and issuance of approvals for procurement by tenders for Health
care procurement in the province.
4. To follow up of the performance status of the products/services on periodic basis and
keeping record of the same.
5. To obtain market information on the products/services and their performance from all over
the province and maintain complete record of the same in the databank.
6. To manage Hospital Projects and coordinate the medical equipment supplies with the
design and construction of the hospital.
7. To attend, review and respond to suppliers/manufacturers protests/grievances related to
technical aspect of the product/services and in a judicial manner and resolve in timely
manner.
8. To ensure that a regular updated list of standardized products and any technical
advancements to all Health care procuring entities in Khyber Pakhtunkhwa.
9. To have liaison with suppliers/manufacturers associations/bodies and keep updated on
the developments that may affect the technical aspects of a product or development or its
performance.
10. To assist the Health care procuring entities in all issues related to technical specification
and comparisons for procurement.
143
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to understand and evaluate technical aspects of the
product/services and be able to evaluate its clinical applications and users requirements
for procurements being carried out in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Powerpoint, MS Access & electronic
document management.
Ability to use any software based program for use in technical aspects of medical devices
and drugs.
Ability to manage and supervise others as team.
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH personnel and Suppliers.
Technical Wing - Job Responsibilities.
Job Title: Technical Officer TW-1 (Pharma)
Qualifications: Graduation from an accredited four year college or university with a degree in
Pharmacy or Micro-Biology/Chemistry is preferred. However, any equivalent
combination of education and experience sufficient to perform job duties may be
considered.
Must also have following:
Comprehensive knowledge of Pharmaceutical Products and their clinical
applications is required.
Comprehensive knowledge of Pharmaceutical raw materials and their
Manufacturing is required.
Experience: Minimum five years experience in the industry of Pharmaceuticals with relevant
experience of technical aspects of procurements is preferred.
Grade: BPS 17 or equivalent or M3
Recruitment: As per Govt. Policy
Position.type: Technical aspect of Pharmaceutical Products and their technologies for Health care
procurement in Khyber Pakhtunkhwa Health Department
144
Jurisdiction: Complete Province
Reports to: For all matters to In charge of the Technical Wing of Procurement Cell of Khyber
Pakhtunkhwa Health Dept.
Direct responsibilities:
1. To work under the direction of the In charge of Technical wing of the Procurement Cell
Khyber Pakhtunkhwa Health dept.
2. To be responsible for maintaining the goals, standards, and objectives of all the
Pharmaceutical Products, Insecticides and services being dealt within the Procurement
Cell in line with the Health care objectives of the Health Department, Govt. of Khyber
Pakhtunkhwa.
3. To formulate, obtain, and maintain policies and procedures for Pharmaceutical
product/services categorization and standardization in line with the provincial Health care
delivery policy at different level of health care facilities.
4. To prepare technical specification and other technical aspects of Pharmaceutical
products/services for standardization of products/services for all procurements being
carried out by the Procurement Cell at provincial level.
5. To notify the same to all procuring entities of the whole province and thereof to act as
guidance and monitoring of the same.
6. To appropriately review and evaluate Pharmaceutical products/services after scrutinizing
and maintaining a database of products and issuance of approvals for procurement by
tenders for Health care procurement in the province.
7. To follow up of the performance status of the Pharmaceutical products/services on
periodic basis and keeping record of the same.
8. To obtain market information on the Pharmaceutical products/services and their
performance from all over the province and maintain complete record of the same in the
databank.
9. To ensure that a regular updated list of standardized Pharmaceutical products and any
technical advancements to all Health care procuring entities in Khyber Pakhtunkhwa.
10. To attend, review and respond to Pharmaceutical suppliers/manufacturers
protests/grievances related to technical aspect of the product/services and in a judicial
manner and resolve in timely manner.
11. To have liaison with Pharmaceutical suppliers/manufacturers associations/bodies and
keep updated on the developments that may affect the technical aspects of a product or
development or its performance.
12. To assist the Health care procuring entities in all issues related to technical specification
and comparisons for procurement of Pharmaceutical products
13. To stay abreast of new technologies & materials, techniques and their market conditions
in to products and services and communicate with in charge procurement on any
145
significant factors that could affect quality and reliability of Pharmaceutical
products/services in Provincial Health Procurements.
14. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the Pharmaceutical
suppliers/manufacturers.
15. To attend/represent Incharge Technical Wing and facilitate team meetings, prepare
supporting documentation, conduct market research, develop market analysis related to
Pharmaceutical products/services and assist in strategy development for effective
procurements.
16. Attendance at work is an essential function of this position.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to understand and evaluate technical aspects of the
product/services and be able to evaluate its clinical applications and users requirements
for procurements being carried out in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Powerpoint, MS Access & electronic
document management.
Ability to use any software based program for use in technical aspects of medical devices
and drugs.
Ability to manage and supervise others as team.
Technical Wing - Job Responsibilities.
Job Title: Technical Officer TW-2 (Bio-medical Devices, Consumables & Ancillary
Hospital Equipment)
Qualifications: Graduation from an accredited four year college or university with a degree in
Biomedical Engineering is strongly preferred. However, any equivalent combination
of education and experience sufficient to perform job duties may be considered.
Must also have following:
Comprehensive knowledge of Electro-medical Products/devices (and their
Technologies & after sales services is required.
Knowledge of Clinical Application and Standards of Medical devices is also
required.
146
Experience in procurement and management of Spare parts of Electro-medical
equipment.
Experience: Minimum seven years experience in the industry of Electro-medical
Products/Devices with relevant experience of technical aspects of procurements is
preferred.
Grade: BPS 17 or equivalent or M3
Recruitment: As per Govt. Policy
Position type: Technical aspect of Electro-Medical Products/Devices and their technologies for
Health care procurement in Khyber Pakhtunkhwa Health Department
Jurisdiction: Complete Province
Reports to: For all matters to In charge of the Technical wing of Procurement Cell of Khyber
Pakhtunkhwa Health Dept.
Direct responsibilities:
1. To work under the direction of the In charge of Technical Wing of the Procurement Cell
Khyber Pakhtunkhwa Health Department.
2. To be responsible for maintaining the goals, standards, and objectives of all the Electro-
Medical Products/Devices and related services being dealt within the Procurement Cell in
line with the Health care objectives of the Health Department, Govt. of Khyber
Pakhtunkhwa.
3. To formulate, obtain, and maintain policies and procedures for Electro-Medical
Products/Devices and related services categorization and standardization in line with the
provincial Health care delivery policy at different level of health care facilities.
4. To prepare technical specification and other technical aspects of Electro-Medical
Products/Devices and related services for standardization of products/services for all
procurements being carried out by the procurement entities at provincial level.
5. To notify the same to all procuring entities of the whole province and thereof to act as
guidance and monitoring of the same.
6. To appropriately review and evaluate Electro-Medical Products/Devices and related
services after scrutinizing and maintaining a database of products and issuance of
approvals for procurement by tenders for Health care procurement in the province.
7. To follow up of the performance status of the Electro-Medical Products/Devices and
related services on periodic basis and keeping record of the same.
8. To obtain market information on the Electro-Medical Products/Devices and related
services and their performance from all over the province and maintain complete record
of the same in the databank.
147
9. To ensure that a regular updated list of standardized Electro-Medical Products/Devices
and related services and any technical advancements to all Health care procuring entities
in Khyber Pakhtunkhwa.
10. To attend, review and respond to Electro-Medical Products/Devices
suppliers/manufacturers protests/grievances related to technical aspect of the
product/services and in a judicial manner and resolve in timely manner.
11. To have liaison with Electro-medical Products/Devices suppliers/manufacturers
associations/bodies and keep updated on the developments that may affect the technical
aspects of a product or development or its performance.
12. To assist the Health care procuring entities in all issues related to technical specification
and comparisons for procurement of Electro-medical Products/Devices.
13. To stay abreast of new technologies & materials, techniques and their market conditions
in to products and services and communicate with in charge procurement on any
significant factors that could affect quality and reliability of Electro-medical
Products/Devices and their services in Provincial Health Procurements.
14. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the Electro-medical Products/Devices
and their services.
15. To attend/represent In charge Technical Wing and facilitate team meetings, prepare
supporting documentation, conduct market research, develop market analysis related to
Electro-medical Products/Devices and services and assist in strategy development for
effective procurements.
16. Attendance at work is an essential function of this position.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to understand and evaluate technical aspects of the
product/services and be able to evaluate its clinical applications and users requirements
for procurements being carried out in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Powerpoint, MS Access & electronic
document management.
148
Ability to use any software based program for use in technical aspects of medical devices
and drugs.
Ability to manage and supervise others as team.
Tendering & Coordination Wing - Job Responsibilities.
Job Title: In charge Tendering & Coordination (T&C) Wing
Qualifications: Graduation from an accredited four year college or university with a Masters degree
in Project Management, Procurement & Contract Management, Business
Administration, Law or a closely related field is strongly preferred. However, any
equivalent combination of education and experience sufficient to perform job duties
may be considered.
Must also have following:
CIPS, CPCM, CPPO or any certified accreditation in Purchasing or Public
Purchasing required, or ability to obtain such within first year of employment.
Comprehensive knowledge of PPRA and other applicable government
regulations is required.
Experience: Minimum seven years experience in the Public Health sector with relevant
experience of administrative aspects of procurements is preferred.
Grade: BPS 18 or equivalent
Recruitment: As per Govt. Policy
Position type: Tender Administration & Coordination of procurements with health care pro-
curement entities of Khyber Pakhtunkhwa Health Department
Jurisdiction: Within the Health department
Reports to: For all matters to In charge of the Procurement Cell of Khyber Pakhtunkhwa Health
Deptt.
Direct responsibilities:
1. To work under the direction of the In charge of Procurement Cell Khyber Pakhtunkhwa
Health Deptt
2. To lead, direct, coordinate, and manage all tendering process for procurements &
Coordination with Health procuring Institutes within the Health Department.
3. To stay abreast of new developments in the Procurement Cell and be able to
communicate to the other procuring institutes of health to whom they are coordinating
4. With respect to Tendering process:
a. To be responsible for carrying out all tendering processes and concluding it in lines
with the PPRA regulations.
149
b. To facilitate team meetings, prepare supporting documentation, related to tendering
process and assist in strategy development for effective procurements.
5. With respect to Coordination Functions:
a. To be responsible for providing support to all Govt procuring agencies like the
Districts, AMIs and Program in their healthcare procurement and related issues. This
wing may be the may be the focal contact point for these organization for obtaining
any relevant information from the procurement department and same may be provided
by the concerned person by internal coordination within the department.
b. To lead, direct, coordinate, and manage all coordination aspects of the Procurements
with the procuring agencies.
6. To train, motivate, coach, develop, and evaluate assigned professional, technical, and
clerical staff of the wing for dedicated and best practice professional working.
7. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the coordinating institutes.
8. To lead, manage and coach cross-functional teams through the information sharing &
strategic sourcing process.
9. To facilitate team meetings, prepare supporting documentation, conduct market research,
develop market analysis related to products/services and assist in strategy development
for effective procurements.
10. To ensure discipline and work ethics of all staff of the coordination Wing and monitor their
performance and professionalism.
11. Attendance at work is an essential function of this position.
Responsibilities through the team members of the Procurement Cell:
1. To formulate, obtain, and maintain procedures for tendering and inter related activities &
to notify the same to all procuring entities of the whole province and thereof to act focus
contacts for providing guidance and support to them.
2. To manage all administrative aspect of tendering process and carry out procurements for
Health Department in and effective and timely manner.
3. To ensure that any development or new policy from the Govt. effecting tendering
procedure is duly informed to the Procurement Cell and updated information is timely
provided to all Health care procuring entities in Khyber Pakhtunkhwa.
4. To have liaison with suppliers/manufacturers associations/bodies and keep updated on
the developments that may affect the tendering process of procurement.
5. To formulate, obtain, and maintain procedures for coordination with the provincial Health
care procurement entities & to notify the same to all procuring entities of the whole
province and thereof to act focus contacts for providing guidance and support to them.
6. To attend, review and respond to requests made by the Districts, AMI and programs
procurement relate issues and resolve in timely manner.
150
7. To ensure that a regular updated information of the related wing is timely provided to all
Health care procuring entities in Khyber Pakhtunkhwa.
8. To assist the Health care procuring entities in all issues related to Pre-Qualifications,
technical specification, Tendering related quarries and any other procurement related
issue.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using technical terminology with technical
writing skills is required.
Extensive judgment and originality to understand the issues and be able to resolve them
for the quarrying body in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Powerpoint, MS Access & electronic
document management.
Ability to manage and supervise others as team.
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH personnel and Suppliers.
Tendering & Coordination Wing - Job Responsibilities.
Job Title: Tendering Officer TC-1 (Tender Administration & Contracts)
Qualifications: Graduation from an accredited four year college or university with a degree in
Project Management, Business Administration, Law or a closely related field is
strongly preferred. However, any equivalent combination of education and
experience sufficient to perform job duties may be considered.
Must also have following:
Knowledge of PPRA regulations and Public Procurements.
Contracts Management
Administrative function and systems of Provincial Govt.
Experience: Minimum five years experience in the Public Health sector with relevant experience
of administrative aspects of procurements is preferred. Or
In case the candidate is not a degree holder, Minimum requirement of Graduation
with minimum ten years of experience in Administrative and Coordination functions
preferably in Public Sector.
151
Grade: BPS 17 or equivalent
Recruitment: As per Govt. Policy
Position type: Tender processing function and contracts of procurements of Khyber Pakhtunkhwa
Health Department
Jurisdiction: Within Govt. of Khyber Pakhtunkhwa, Health department
Reports to: For all matters to In charge of the Tender & coordination Wing of the Procurement
Cell of Khyber Pakhtunkhwa Health dept.
Direct responsibilities:
1. To work under the directions of the In charge of the Tender & coordination Wing of
Procurement Cell Khyber Pakhtunkhwa Health dept.
2. To formulate, obtain, and maintain procedures for tendering and inter related activities of
Health Care procurement being carried out by the Health Dept of Khyber Pakhtunkhwa.
3. To formulate, obtain, and maintain various forms of contracts for tendering and contracts
management activities of Health Care procurement being carried out by the Health Dept
of Khyber Pakhtunkhwa.
4. To notify the same to all procuring entities of the Khyber Pakhtunkhwa Health Dept. and
thereof provide guidance and support to them.
5. To manage all administrative aspect of tendering process and carry out procurements for
Health Department as per PPRA regulations and in and effective and timely manner.
6. To provide advisory function for contracts and related issues of tendering and order
placing.
7. To ensure that any development or new policy from the Govt. effecting tendering
procedure is duly informed to the Procurement Cell and updated information is timely
provided to all Health care procuring entities in Khyber Pakhtunkhwa.
8. To have active liaison with various wings of the Procurement Cell in carrying out the
tender process and its documentations.
9. To have liaison with suppliers/manufacturers associations/bodies and keep updated on
the developments that may affect the tendering process of procurement.
10. To attend/facilitate and represent Incharge Tendering & Coordination in team meetings,
prepare supporting documentation, related to tendering process and assist in strategy
development for effective procurements.
11. To guide the Health care Procuring entities in all issues and Policies related to Public
tendering Process and its documentation in a timely and effect manner.
12. Attendance at work is an essential function of this position.
Note: 1.The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
152
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing skills is required.
Extensive judgment and originality to understand the issues and be able to resolve them
for the quarrying body in the whole province.
Comprehensive knowledge of personal computers, Internet & electronic document
management.
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH personnel.
Tendering & Coordination Wing - Job Responsibilities.
Job Title: Coordination Officer (25 districts, AMIs & Vertical Programs)
Qualifications: Graduation from an accredited four year college or university with a degree in Public
administration, Business management or a closely related field is strongly preferred.
However, any equivalent combination of education and experience sufficient to
perform job duties may be considered.
Must also have following:
Knowledge of PPRA regulations and Public Procurements.
Administrative function and systems of Provincial Govt.
Experience: Minimum five years experience in the Public Health sector with relevant experience
of administrative aspects of procurements is preferred. Or
Incase the candidate is not a degree holder, Minimum requirement of Graduation
with minimum ten years of experience in Administrative and Coordination functions
preferably in Public Sector.
Grade: BPS 16/17 or equivalent
Recruitment: As per Govt. Policy
Position type: Coordination function of procurements with the assigned Coordinating Insti-tution* of
Khyber Pakhtunkhwa Health Department
Jurisdiction: Within the assigned Coordinating Institution* of Health department
Reports to: For all matters to In charge of the Tender & coordination Wing of the Procurement
Cell of Khyber Pakhtunkhwa Health dept.
Direct responsibilities:
1. To work under the direction of the In charge of the Tender & coordination Wing of
Procurement Cell Khyber Pakhtunkhwa Health dept.
153
2. To formulate, obtain, and maintain procedures for coordination with the provincial Health
care procurement entities & to notify the same to all procuring entities of the whole
province and thereof to act focus contacts for providing guidance and support to them.
3. To attend, lead, direct, coordinate, and manage all quarries related to Procurement
received from the Assigned Coordinating Institutes & resolve the same in a timely manner
by coordination with relevant wings of the Procurement Cell of the Health Department.
4. To be responsible for providing support to all the assigned Govt procuring agencies in
their healthcare procurement and related issues. He/she may be the focal contact point
for these organizations for obtaining any relevant information from the procurement
department.
5. To stay abreast of new developments in the Procurement Cell and be able to
communicate to the assigned Coordinating Institutes to whom they are responsible.
6. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the coordinating institutes.
7. To ensure that a regular updated information of the related wing is timely provided to all
Health care procuring entities in Khyber Pakhtunkhwa.
8. To guide the Health care procuring entities in all issues related to Pre-Qualifications,
technical specification, Tendering related quarries and any other procurement related
issue.
9. To attend/facilitate and represent In charge Tender & Coordination in team meetings,
prepare supporting documentation, review issues of the assigned procuring institutions
and analysis the same and thereof assist in strategy development for effective
procurements.
10. Attendance at work is an essential function of this position.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
* Note 2: The coordinating Institution refers to the assigned districts or AMI/Programs.
Four posts are foreseen three number handling 12 districts each and the fourth one
dealing with AMIs and Programs.
Skills required in additional to qualifications:
Ability to communicate orally and in writing skills is required.
Extensive judgment and originality to understand the issues and be able to resolve them
for the quarrying body in the whole province.
Comprehensive knowledge of personal computers, Internet & electronic document
management.
154
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH personnel and Assigned coordinating Institutes.
Budget & Planning Wing - Job Responsibilities.
Job Title: In charge Budgets & Planning
Qualifications: Graduation from an accredited four year college or university with a degree in
Finance, Business Management or a closely related field is strongly preferred.
However, any equivalent combination of education and experience sufficient to
perform job duties may be considered.
Must also have following:
Knowledge of PPRA
Administrative knowledge of Khyber Pakhtunkhwa Govt Business and financial
regulations.
Knowledge of Khyber Pakhtunkhwa Govt. Financial Management system.
Experience: Minimum seven years experience in the Public Health sector with relevant
experience of Financial and administrative aspects of procurements is preferred.
Grade: BPS 18 or equivalent
Recruitment: As per Govt. Policy
Position type: Budget & Planning of procurements in Health care procuring entities of Khyber
Pakhtunkhwa Health Department
Jurisdiction: Complete Province
Reports to: For all matters to In charge of the Procurement Cell of Khyber Pakhtunkhwa Health
dept.
Direct responsibilities:
1. To work under the direction of the In charge of Procurement Cell Khyber Pakhtunkhwa
Health dept.
2. To lead, direct, coordinate, and manage all Budgetary and Planning aspects of the
Procurements within the DoH.
3. To train, motivate, coach, develop, and evaluate assigned professional, technical, and
clerical staff of the wing for dedicated and best practice professional working.
4. To stay abreast of new developments within the Provincial Finance Dept. and
communicate to the In charge Procurement Cell and the other procuring institutes of
health.
5. To have liaison with Finance Department and other depts. and keep updated on the
developments that may affect the financial aspects of a product or development or its
performance.
155
6. To lead, manage and coach cross-functional teams through the information sharing &
strategic sourcing process.
7. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the coordinating institutes.
8. To facilitate team meetings, prepare supporting documentation, conduct market research,
develop market analysis related to budget & planning of the procurements and assist in
strategy development for effective procurements.
9. To ensure discipline and work ethics of all staff of the coordination Wing and monitor their
performance and professionalism.
10. Attendance at work is an essential function of this position.
Responsibilities through the team members of the Procurement Cell:
1. To formulate, obtain, and maintain procedures for Budgeting & planning of procurement
of Health care products for Khyber Pakhtunkhwa Health Department.
2. To notify the same to all procuring entities of the whole province and thereof to provide
guidance and support to them with regards to Procurement budget and planning.
3. To attend, review and respond to requests made by the Districts, AMI and programs
related to procurement Budgets issues and resolve/guide them in timely manner.
4. To ensure that a regular updated information of the financial releases of the procurement
budgets is promptly provided to all Health care procuring entities in Khyber Pakhtunkhwa.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using financial terminology with appropriate
writing skills is required.
Extensive judgment and originality to understand the issues and be able to resolve them
for the quarrying body in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Access & electronic document
management.
Ability to manage and supervise others as team.
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH & Finance Department.
156
Budget & Planning Wing - Job Responsibilities.
Job Title: Planning Officer BF-1
Qualifications: Graduation from an accredited four year college or university with a degree in
Finance, Business Management or a closely related field is strongly preferred.
However, any equivalent combination of education and experience sufficient to
perform job duties may be considered.
Must also have following:
Knowledge of PPRA
Administrative knowledge of Khyber Pakhtunkhwa Govt Business and financial
regulations.
Knowledge of Khyber Pakhtunkhwa Govt. Financial Management system.
Experience: Minimum five years experience in the Public Health sector with relevant experience
of Financial and administrative aspects of procurements is preferred.
Grade: BPS 17 or equivalent
Recruitment: As per Govt. Policy
Position type: Budget & Planning of procurements in Health care procuring entities of Khyber
Pakhtunkhwa Health Department
Jurisdiction: Complete Province
Reports to: For all matters to In charge of the Procurement Cell of Khyber Pakhtunkhwa Health
dept.
Direct responsibilities:
1. To work under the direction of the In charge of Budget & Planning Wing of Procurement
Cell of Khyber Pakhtunkhwa Health dept.
2. To lead, direct, coordinate, and manage all Budgetary and Planning aspects of the
Procurements within the DoH.
3. To formulate, obtain, and maintain procedures for Budgeting & planning of procurement
of Health care products for Khyber Pakhtunkhwa Health Department.
4. To notify the same to all procuring entities of the whole province and thereof to provide
guidance and support to them with regards to Procurement budget and planning.
5. To monitor the planning of procurement and their actual schedules and to escalate any
issues of concerned to the Director Procurement Cell or the Procuring Institutes.
6. To attend, review and respond to requests made by the Districts, AMI and programs
related to procurement Budgets issues and resolve/guide them in timely manner.
7. To ensure that a regular updated information of the financial releases of the procurement
budgets is promptly provided to all Health care procuring entities in Khyber Pakhtunkhwa.
157
8. To have liaison with Finance Department and other depts. and keep updated on the
developments that may affect the financial aspects of a product or development or its
performance.
9. To apply excellent customer service skills, establish and maintain effective working
relationships with other employees of the Dept. and the coordinating institutes.
10. To attend/facilitate team meetings, prepare supporting documentation, conduct market
research, develop market analysis related to budget & planning of the procurements and
assist in strategy development for effective procurements.
11. Attendance at work is an essential function of this position.
Note: 1. The duties listed above are intended only as illustrations of the various types of
work that may be performed. The omission of specific statements of duties does not
exclude them from the position if the work is similar, related or a logical assignment to the
position.
Skills required in additional to qualifications:
Ability to communicate orally and in writing, using financial terminology with appropriate
writing skills is required.
Extensive judgment and originality to understand the issues and be able to resolve them
for the quarrying body in the whole province.
Comprehensive knowledge of personal computers and software packages, including
specific knowledge of MS Word, MS Excel, MS Access & electronic document
management.
Ability to manage and supervise others as team.
Ability to establish and maintain effective working relationships with co-workers,
supervisors, other DOH & Finance Department.
158
10. Annexures
10.1: List of Persons Interviewed Annex-1
S.No Department/Category Designation/Institute Name
Health Secretariat, KP
1. Health Secretariat, KP Secretary Health Mr. Ashfaq Ahmad Khan
2. Health Secretariat, KP Special Secretary Dr. Noor al Iman
3. Health Secretariat Additional Secretary
Development (M&E)
Mr. Zahir Alam Khan
4. Drug Section, Health
Secretariat
Deputy Director (Drugs) Mr. Ali Zahir Shah
5. Drug Section, Health
Secretariat
Section Officer (Drugs) Mr. Naseer Ahmad
6. Planning Cell, Health
Secretariat
Section Officer Planning Dr. Shaheen Afridi
7. Planning Cell, Health
Secretariat
Chief Planning Officer Mr. Sher Gul Safi
8. Planning Cell, Health
Secretariat
Senior Planning Officer Mr. Bahr Ullah Khan
Directorate General Health Services (DGHS), KP
9. Directorate General Health
Services
Director General Health
Services
Dr. Sharif Ahmad Khan
10. Directorate General Health
Services
Deputy Director (Admn) Dr. Muhammad Zafar
11. Directorate General Health
Services
Assistant Director
(Procurement Cell)
Dr. Muhammad Saleem
12. Directorate General Health
Services
Pharmacist Govt-MCC Mr. Welayat Shah
13. Directorate General Health
Services
Chief Drug Inspector Mr. Sabir Ali
14. Directorate General Health
Services
Deputy Director Pre-
Qualification Cell
Mr. Dil Nawaz Khan
15. Directorate General Health
Services
Senior Pharmacist Mr. Muhammad Saleem
16. Electro-Medical Workshop XEN Bio-Medical Mr. Muhammad Yaseen
Health Sector Reforms Unit (HSRU)
17. Health Sector Reforms Unit
(HSRU)
Chief HSRU Dr. Shabina Raza
159
18. Health Sector Reforms Unit
(HSRU)
Deputy Chief HSRU Dr. Siraj Khan
19. Health Sector Reforms Unit
(HSRU)
Coordinator (M&E) Dr. Shahid Yunus
20. Health Sector Reforms Unit
(HSRU)
Assistant Coordinator
HSRU
DR. Azmat Ullah
Finance Department, KP
21. Finance Department, KP Additional Secretary Mr. Nadeem Bashir
Vertical Programs
22. MNCH, KP Program Coordinator Dr. Khayal ur Rehman Afridi
23. MNCH (M&E) Dr. Abid Hussain
24. MNCH Director Finance Mr. Hamid Hussain
25. MNCH Incharge Stores Mr. Rangeen Khan
26. EPI Deputy Director EPI Dr. Janbaz Afridi
27. EPI Finance Manager Mr. Khizar Hayat
28. Roll Back Malaria Program Manager Dr. Khalid Iqbal
Districts
30. Districts EDO (Health)
Abbottabad
Dr. Zafeer Ahmad
31. Districts EDO (Health) Mardan Dr. Arshad Khan
32. District Hospital Pharmacist,
DHQ Kohat / Member
T&E Committee DGHS
Mr. Khalid Rehman
33. District Drug Inspector,
Peshawar
Mr. Aurangzeb Khan
Autonomous Medical Institutions (AMIs)
34. AMI- Hayatabad Medical
Complex (HMC), Peshawar
Associate Dean
(Oncology Department)
Prof. Abid Jameel
35. AMI- Lady Reading Hospital
(LRH), Peshawar
Chief Pharmacist Ms Syeda Tehniyat
36. AMI- Khyber Teaching Hospital Pharmacist KTH Mr. Zahid Ali Khan
Medical Colleges
37. Khyber College of Dentistry,
Peshawar
Associate Professor /
Member T&E Committee
(KMC, KTH, KCD)
Dr. Javed Qazi
160
38. Khyber Medical College,
Peshawar
Stores Incharge Mr. Khursheed Khan
Auditor General of Pakistan, Peshawar
39. Auditor General Peshawar Deputy Director Audit Mr. Bahadur Shah
40. Auditor General Peshawar
(PAC)
Deputy Director Audit Mr. Mutahir Rehman
Pharmaceutical Sector
41. BF Biosciences (Ferozsons
Labs)
Hepatology Manager Mr. Zia ur Rehman
42. Getz Pharma (Pvt) Ltd Institutional Business
Executive
Mr. Shahid Ali
43. A.Y Traders, Peshawar Chief Executive Mr. Shahbaz Khan
44. Leads Pharma (Pvt) Ltd National Sales Manager Mr. Shahnawaz Qureshi
161
Annex-2
10.2: Training Calendar for TA-52
Strengthening of Procurement Systems & Capacity Building of DoH Khyber Pakhtunkhwa
December 2012 Sequence Duration Level Participants Location Month/Year
Khyber Pakhtunkhwa
Public Procurement
Rules 2012
Day 1 2 days Basic Procurement
Officials to be
nominated by
DGHS &
HSRU
Abbottabad January 3-4 2013
Procurement Life
Cycle
Day 2 Intermediate
Khyber Pakhtunkhwa
Public Procurement
Rules 2012
Day 1 2 days Basic Procurement
Officials to be
nominated by
DGHS &
HSRU
Islamabad January
30-31 2013
Procurement Life
Cycle
Day 2 Intermediate
February 2013 Sequence Duration Level Participants Location Month/Year
Khyber Pakhtunkhwa
Public Procurement
Rules 2012
Day 1 2 days Basic Senior
Management
Health
Department
Murree February
3-4 2013
Procurement Life
Cycle
Day 2 Intermediate
Inventory Management
& Warehousing
Day 1 Advanced Inventory
/Storage
Managers of
Vertical
Programs/Pr
ojects//DHQs
/Districts
Islamabad February 21-22
2013
Multi-modal
Transportation
Management in Supply
Chain of
Pharmaceutical Goods
Day 2 Advanced
Procurement of
Consultancy Services
under QCBS Selection
Method; Bidding
Document Design and
Evaluation of Supplier
& Consultant: Contract
Management of
Management Services
Day 1 Advanced HSRU Peshawar 27 February 2013
March 2013 Sequence Duration Level Participants Location Month/Year
Development of PC-1
& Procurement Plan
Day 1 1 day Advanced Procurement
Officials to be
nominated by
Secretary
Health,
DGHS &
HSRU
Being
worked out
in
consultation
with DGHS
March 4 2013
Execution of Work
Packages through
Work Breakdown
Structure (WBS) and
Procurement Audit
Day 1 Advanced
Comparative
Contracting Practices
in Donor-funded
Projects
Day 1 1 day Advanced Procurement
Officials to be
nominated by
DGHS &
Being
worked out
in
consultation
March 26
162
Procurement of
Consultancy Services
under QCBS Selection
Method
Day 1 Advanced
HSRU with DGHS
April 2013 Sequence Duration Level Participants Location Month/Year
Khyber Pakhtunkhwa
Public Procurement
Rules 2012
Day 1 2 days Basic Procurement
Officials to be
nominated by
DGHS &
HSRU
Being
worked out
in
consultation
with DGHS
April 8-9 2013
Procurement Life
Cycle
Day 2 Intermediate
Contract Management
w.r.t Health Sector
Day 1 2 days Advanced Procurement
Officials to be
nominated by
DGHS &
HSRU
Being
worked out
in
consultation
with DGHS
April 22-23 2013
Bidding Document
Design and Evaluation
of Suppliers of
Pharmaceuticals and
Bio-Medical
Equipment
Day 2 Advanced
May 2013 Sequence Duration Level Participants Location Month/Year
Khyber Pakhtunkhwa
Public Procurement
Rules 2012
Day 1 2 days Basic Procurement
Officials to be
nominated by
DGHS &
HSRU
Being
worked out
in
consultation
with DGHS
May 6-7 2013
Procurement Life
Cycle
Day 2 Intermediate
Contract Management
w.r.t Health Sector
Day 1 2 days Advanced Procurement
Officials to be
nominated by
DGHS &
HSRU
Being
worked out
in
consultation
with DGHS
May 27-28 2013
Bidding Document
Design and Evaluation
of Suppliers of
Pharmaceuticals and
Bio-Medical
Equipment
Day 2 Advanced
June 2013 Sequence Duration Level Participants Location Month/Year
Inventory Management
& Warehousing
Day 1 2 days Advanced Procurement
Officials to be
nominated by
DGHS &
HSRU
Being
worked out
in
consultation
with DGHS
June 3-4 2013
Multi-modal
Transportation
Management in Supply
Chain of
Pharmaceutical Goods
Day 2 Advanced
Contract Management
w.r.t Health Sector
Day 1 2 days Advanced Procurement
Officials to be
nominated by
DGHS &
HSRU
Being
worked out
in
consultation
with DGHS
June 24-25 2013
Bidding Document
Design and Evaluation
of Suppliers of
Pharmaceuticals and
Bio-Medical
Equipment
Day 2 Advanced
163
Annex-3
10.3: Supply Chain Questionnaire:
1 Goods Clearance & Transportation Management
Is there any system in place that can expedite the receiving of Shipment?
No Yes If yes, please give details
At the import stage?
At the freight forwarding stage?
At the destination/Health Facility?
2 - Inventory Management
Is there any system in place that can verify whether the medicines supplied from the supplier are in
compliance with those that have been asked? If yes, please give details:
Yes No Details
Separate space for checking the arrived
medicine/ equipment
Is there a designated person for checking the
receipts against the list?
Is the invoice documented anywhere?
Is the dosage, strength and packaging of drugs
checked?
Are the medicine supplied are appropriately
labeled?
Are the samples from the batch of medicine
sent to drug testing laboratory to check their
potency and efficacy?
Are the medicines from the sampled batch
issued before the receipt of DTL Report?
If yes, is the said fact recorded in a DTL
Register somewhere?
1.3-Is there enough space available for the storage of received pharmaceutical drugs? If yes Please
answer the following?
Yes No Remarks
Classified Alphabetically?
Classified Therapeutically?
Classified by Dosage form?
164
Is the storage space enough to facilitate
movement?
Are the medicine placed directly on floor?
If pallets are used, are they in good conditions?
Is there any mechanism for the control of
temperature and humidity in the ware house?
Is there any bin card arrangement available
with the stock of individual item in the
warehouse?
1.4-How is the integrity of drugs protected from the effect of climate during transportation and
distribution to primary Health Facilities (For Districts)?
Yes No Remarks
Are reefer containers used in vans, maintaining
temperatures at 2-8C?
If not, are the drug cartons covered from
sunlight through canopy vans or parachute
tarpaulins?
2- Storage & Distribution Documentation:
2.1 - Is there any system (Bin Cards, Stock Cards etc.) that documents the storage of
pharmaceutical in the ware house?
Yes NO Remarks
Does it document the date of receiving of the
shipment?
Does it document the date of delivery of
medicine to the primary health facilities?
Does it document the batch number, name and
strength of the individual medicine?
Does it document the expiry date of each
receiving shipment/delivery?
Does it specify the quantity send to individual
Health Facility?
Does it specify the name of Health Facility to
which the medicine are sent?
165
3 Inventory Management:
3.1 - Is there an inventory management system at each level of the distribution system which
provides information as minimum on the following elements?
YES NO Remarks
The average working stock for each Product?
The amount of safety (buffer) stock for each
Product?
The frequency of reordering for each product?
The Quantity of re-ordering for each product?
The Lead Time before replenishment of stock?
The Expiry Date of the drug?
3.2 - Are there any Standard Operating Procedures (SOPs) for stock Management at each level of
the Distribution System ?
Yes NO Remarks
4 Internal Audit of Stocks:
4.1 - Is there any physical inventory verification conducted on the stocks and reconciled with the
records by the Health Facility?
Yes NO Remarks
Monthly
After every 3 months
After every 6 Months
Once a year
4.2 - If other verification exercise conducted, please specify? ______________________
4.3 - Are there independent audits of warehouse by external inspectors or auditors /AGPR?
Yes NO Remarks
Any observations by Audit?
If yes, please give detail
5 Distribution:
5.1 - Is there a system (computerized or manual) to track the movement of products from
pharmaceutical ware house to a health Facility/Ward, and which provides the following information
for medicine that have left the ware house?
166
Yes No Remarks
Types of medicine that have left the ware
house?
Quantity of medicine that have left the
warehouse?
The person who verified the amount?
The intended recipient of these medicine?
The time and date that medicine arrived at
appropriate facility?
Documentation of any regularities or problem
with the supplies received?
6 Requisition of Products:
6.1 - Does the health facility have any appropriate procedure for requesting medicine?
Yes No Remarks
Is the medicine requisitioned on the basis of its
generic / International Non-Proprietary name
(INN)?
Requisitioned on basis of Dosage form?
Requisitioned on basis of Strength?
Requisitioned on basis of Quantity?
Is the requisition checked by responsible
person with date and signatures?
7 Consumption Reporting of Drugs:
7.1 - Is the medicine consumption at the facility level reported back to the District/AMI?
Yes NO Remarks
Is it reported on daily basis?
Is it reported on weekly or bi-weekly
Is it reported on Monthly basis?
8 Pilferage Control:
8.1 - What are the possible means of pilferage of medicines and how to check it?
Yes NO Remarks
Is there any mechanism to detect pilferage?
If yes, please give detailed measures
Vous aimerez peut-être aussi
- C6 RS6 Engine Wiring DiagramsDocument30 pagesC6 RS6 Engine Wiring DiagramsArtur Arturowski100% (3)
- Procurement ManualDocument59 pagesProcurement ManualAshis Daskanungo100% (1)
- 1-SPS333 Part II Event Planning (Compatibility Mode)Document44 pages1-SPS333 Part II Event Planning (Compatibility Mode)Husna NazirahPas encore d'évaluation
- PROJ 598 Contract and Procurement ManagementDocument2 pagesPROJ 598 Contract and Procurement ManagementAlan MarkPas encore d'évaluation
- Swan Mundaring Reform Project Management Plan LGNSW Amalgamation ToolkitDocument140 pagesSwan Mundaring Reform Project Management Plan LGNSW Amalgamation ToolkitSyed Mujahid AliPas encore d'évaluation
- Procure SOP - CompressedDocument95 pagesProcure SOP - Compresseddrmohamed120Pas encore d'évaluation
- Spatial Characteristics of Transportation Hubs - Centrality and Intermediacy - Fleming (1994)Document16 pagesSpatial Characteristics of Transportation Hubs - Centrality and Intermediacy - Fleming (1994)Ali Raza HanjraPas encore d'évaluation
- Procurement PolicyDocument7 pagesProcurement Policytess100% (2)
- Secretariat Instructions 2004 - ContentsDocument6 pagesSecretariat Instructions 2004 - Contentsfaisal80Pas encore d'évaluation
- Standard Operating Procedure: ProjectsDocument1 pageStandard Operating Procedure: ProjectsShena BrittoPas encore d'évaluation
- Procurement ManualDocument49 pagesProcurement ManualDr. MadhusudhanaRao ThummalaPas encore d'évaluation
- Roles and Responsibilities of Key Stakeholders in The Procurement Process/CycleDocument27 pagesRoles and Responsibilities of Key Stakeholders in The Procurement Process/CycleSylvia Nabwire100% (1)
- IRR SPMS. Revised (2017)Document11 pagesIRR SPMS. Revised (2017)Jay FabiPas encore d'évaluation
- Evaluation Guide (Consultancy) PDFDocument50 pagesEvaluation Guide (Consultancy) PDFStefanos DiamantisPas encore d'évaluation
- Public Procurement ActDocument80 pagesPublic Procurement ActDixit AwasthiPas encore d'évaluation
- Using Procurement Performance Indicators To Strengthen The Procurement Process For Public Health CommoditiesDocument48 pagesUsing Procurement Performance Indicators To Strengthen The Procurement Process For Public Health Commoditiesmamica53Pas encore d'évaluation
- The Procurement Cycle: First ExampleDocument12 pagesThe Procurement Cycle: First ExampleAnamaria Popescu AnamariapopescuPas encore d'évaluation
- B02 - Procurement Planning - DLS 2022 PDFDocument54 pagesB02 - Procurement Planning - DLS 2022 PDFRoy Rex De VeyraPas encore d'évaluation
- Procurement ManagementDocument44 pagesProcurement ManagementGreatmanPas encore d'évaluation
- Purchasing Management Unit 1Document16 pagesPurchasing Management Unit 1DEREJEPas encore d'évaluation
- Ifp 23 Estimating Retirement Needs and How Much Do You Need On RetirementDocument9 pagesIfp 23 Estimating Retirement Needs and How Much Do You Need On Retirementsachin_chawlaPas encore d'évaluation
- Procurement Manual 2013 Rev7Document287 pagesProcurement Manual 2013 Rev7Faisal CoolPas encore d'évaluation
- Master of Business Administration-MBA Semester 2 MB0049 - PROJECT MANAGEMENT - 4 Credits (Book ID: B1632) Assignment Set - 1Document11 pagesMaster of Business Administration-MBA Semester 2 MB0049 - PROJECT MANAGEMENT - 4 Credits (Book ID: B1632) Assignment Set - 1Aman GuptaPas encore d'évaluation
- Procurement Function Final PDFDocument4 pagesProcurement Function Final PDFJuliet CastroPas encore d'évaluation
- Procurement ProcessDocument73 pagesProcurement ProcessShivaniSharma100% (1)
- Consulting Response For Training RequestDocument50 pagesConsulting Response For Training RequestmailstosjPas encore d'évaluation
- Procurement and Supply ManagementDocument36 pagesProcurement and Supply ManagementCipaidunkPas encore d'évaluation
- Procurement Manual PSMLDocument60 pagesProcurement Manual PSMLShaygan EjazPas encore d'évaluation
- Aligning Performance Plans With Organizational Goals: OPM's Eight-Step ProcessDocument6 pagesAligning Performance Plans With Organizational Goals: OPM's Eight-Step ProcessPaolo PetruccianiPas encore d'évaluation
- Project monitoring and evaluation guidelines - Keeping track of progress and resultsDocument41 pagesProject monitoring and evaluation guidelines - Keeping track of progress and resultsMaria Gabriela PopaPas encore d'évaluation
- Procurement ReportDocument13 pagesProcurement ReportNajwy Saifudin100% (1)
- Project Monitoring and Evaluation and Its Importance - Nandwa Muyuka - Pulse - LinkedinDocument3 pagesProject Monitoring and Evaluation and Its Importance - Nandwa Muyuka - Pulse - LinkedinShepherd NhangaPas encore d'évaluation
- Procurement Strategy Sample Template March 2013Document13 pagesProcurement Strategy Sample Template March 2013hasitha203252Pas encore d'évaluation
- Expression of Interest Pre Qualification of HR ConsultancyDocument12 pagesExpression of Interest Pre Qualification of HR ConsultancyFaisi GikianPas encore d'évaluation
- Procurement and Supplies Professionals A PDFDocument115 pagesProcurement and Supplies Professionals A PDFNyeko FrancisPas encore d'évaluation
- Guidelines On Non-Governmental Organization Participation in Public ProcurementDocument5 pagesGuidelines On Non-Governmental Organization Participation in Public ProcurementAnnamaAnnamaPas encore d'évaluation
- What Does Retirement Mean To YouDocument5 pagesWhat Does Retirement Mean To Youmaria gomezPas encore d'évaluation
- Procurement ProceduresDocument13 pagesProcurement ProceduresGILBERTO YOSHIDAPas encore d'évaluation
- Procurement MaturityDocument80 pagesProcurement MaturityWisnu Budi SunaryoPas encore d'évaluation
- D3 Sourcing in Procurement and SupplyDocument4 pagesD3 Sourcing in Procurement and SupplyAhmed HasanPas encore d'évaluation
- HRD EvaluationDocument11 pagesHRD EvaluationNisha ParwaniPas encore d'évaluation
- Company Profile & Office PicturesDocument15 pagesCompany Profile & Office PicturesAhad IncarnationPas encore d'évaluation
- Procurement ProcessDocument24 pagesProcurement ProcessCarlos Magtangob100% (1)
- ProcurementsDocument40 pagesProcurementssurenderPas encore d'évaluation
- Procurement Strategy ComponentsDocument2 pagesProcurement Strategy Componentsm_vasilyevaPas encore d'évaluation
- 3 Guide Performance Review-Evaluation 2013 - Mar13Document11 pages3 Guide Performance Review-Evaluation 2013 - Mar13Mark Joseph BajaPas encore d'évaluation
- ISO 9001 System Implementation ScheduleDocument2 pagesISO 9001 System Implementation Schedulefcleong69Pas encore d'évaluation
- Vendor 1Document142 pagesVendor 1aks2318Pas encore d'évaluation
- Procurement Training - Disposal of AssetsDocument44 pagesProcurement Training - Disposal of AssetsKintu MunabangogoPas encore d'évaluation
- Guidance Note 1 - REV - 0 - Tracked ChangesDocument75 pagesGuidance Note 1 - REV - 0 - Tracked ChangesIFC SustainabilityPas encore d'évaluation
- Budgeting and Budgetary ControlDocument38 pagesBudgeting and Budgetary Controlessien akpanukoPas encore d'évaluation
- Performance Appraisal Form Version 2Document5 pagesPerformance Appraisal Form Version 2asd dsaPas encore d'évaluation
- 137167312PMO Procurement Plan TemplateDocument12 pages137167312PMO Procurement Plan TemplateJulian Ho100% (1)
- Memorandum: Performance Management System For Leaders (SPMS), To Be Held OnDocument3 pagesMemorandum: Performance Management System For Leaders (SPMS), To Be Held OnMario Roldan Jr.100% (1)
- Project and Change Management Lecture 1Document34 pagesProject and Change Management Lecture 1tanto_deep_15Pas encore d'évaluation
- Implementation Toolkit 5 MonitoringDocument6 pagesImplementation Toolkit 5 MonitoringJoana Mae Tulauan BernardinoPas encore d'évaluation
- SOP 11-Conflict of Interest Rev 1Document3 pagesSOP 11-Conflict of Interest Rev 1Bang CacihPas encore d'évaluation
- PIA Pre-Qualification Document for Suppliers & VendorsDocument20 pagesPIA Pre-Qualification Document for Suppliers & VendorsImran Qadir100% (2)
- Faster Procurement Process Study ReportDocument24 pagesFaster Procurement Process Study ReportkeyspPas encore d'évaluation
- Procurement Planning & ActivityDocument18 pagesProcurement Planning & ActivityJohn Salolog100% (1)
- 655 Af 2 B 2189 B 71700459186Document56 pages655 Af 2 B 2189 B 71700459186Atish SwainPas encore d'évaluation
- The Referral System Revised: DisclaimerDocument33 pagesThe Referral System Revised: Disclaimervani reddyPas encore d'évaluation
- EoDB - PAK PDFDocument117 pagesEoDB - PAK PDFAli Raza HanjraPas encore d'évaluation
- Understanding Buyer and Supplier Power - A Framework For Procurement and Supply Competence-Cox2001Document8 pagesUnderstanding Buyer and Supplier Power - A Framework For Procurement and Supply Competence-Cox2001Ali Raza HanjraPas encore d'évaluation
- Pakistan - OECD Trade Facilitation IndicatorsDocument2 pagesPakistan - OECD Trade Facilitation IndicatorsAli Raza HanjraPas encore d'évaluation
- The Trade Facilitation Index (Rev2) PDFDocument114 pagesThe Trade Facilitation Index (Rev2) PDFAli Raza HanjraPas encore d'évaluation
- The Process of Business Relationship Ending - Its Stages and Actors - Thtinen-2000Document23 pagesThe Process of Business Relationship Ending - Its Stages and Actors - Thtinen-2000Ali Raza HanjraPas encore d'évaluation
- Corporate Responsibility and Value Creation in The Port Sector Michele Acciaro (2015)Document23 pagesCorporate Responsibility and Value Creation in The Port Sector Michele Acciaro (2015)Ali Raza HanjraPas encore d'évaluation
- G0-Touch Manual For Mac - ENDocument7 pagesG0-Touch Manual For Mac - ENAli Raza HanjraPas encore d'évaluation
- EoDB Reforms by FBR For Paying Taxes-EODBDocument33 pagesEoDB Reforms by FBR For Paying Taxes-EODBAli Raza HanjraPas encore d'évaluation
- Understanding Port Efficiency - A CPEC Perspective A. R. Hanjra, Omar K. Bhatti, Saadia NiaziDocument20 pagesUnderstanding Port Efficiency - A CPEC Perspective A. R. Hanjra, Omar K. Bhatti, Saadia NiaziAli Raza HanjraPas encore d'évaluation
- Concentration and Load Centre Development in The European Container Port System - Theo E Notteboom (1997)Document17 pagesConcentration and Load Centre Development in The European Container Port System - Theo E Notteboom (1997)Ali Raza HanjraPas encore d'évaluation
- Factors Affecting Trust in Market Research Relationships-Moorman-1993Document22 pagesFactors Affecting Trust in Market Research Relationships-Moorman-1993Ali Raza HanjraPas encore d'évaluation
- Efficiency Measurement of Major Container Terminals in AsiaDocument9 pagesEfficiency Measurement of Major Container Terminals in AsiaAli Raza HanjraPas encore d'évaluation
- Evaluating The Competitiveness of Container Ports in Korea and China - Yeo Et AlDocument12 pagesEvaluating The Competitiveness of Container Ports in Korea and China - Yeo Et AlAli Raza HanjraPas encore d'évaluation
- Competition Excess Capacity and The PriceDocument25 pagesCompetition Excess Capacity and The PriceAli Raza HanjraPas encore d'évaluation
- Sro 827Document6 pagesSro 827Benjamin PrattPas encore d'évaluation
- An Analytical Hierarchy Process Framework For Comparing The Overall Performance of Manufacturing Departments Andrea Rangone 1996Document17 pagesAn Analytical Hierarchy Process Framework For Comparing The Overall Performance of Manufacturing Departments Andrea Rangone 1996Ali Raza HanjraPas encore d'évaluation
- Towards A Methodology For Developing Evidence-Informed Management Knowledge by Means of Systematic Review David Tranfield-2003Document16 pagesTowards A Methodology For Developing Evidence-Informed Management Knowledge by Means of Systematic Review David Tranfield-2003Ali Raza HanjraPas encore d'évaluation
- The Philosophy of Science of Social ResearchDocument11 pagesThe Philosophy of Science of Social ResearchImronPongjiSamasajaPas encore d'évaluation
- Social Science and The Philosophy of ScienceDocument10 pagesSocial Science and The Philosophy of ScienceAli Raza HanjraPas encore d'évaluation
- Dyadic Business Relationships within Business NetworksDocument16 pagesDyadic Business Relationships within Business NetworksAli Raza HanjraPas encore d'évaluation
- Conflict and Conflict Management - Reflections and Update - Thomas-1992Document10 pagesConflict and Conflict Management - Reflections and Update - Thomas-1992Ali Raza HanjraPas encore d'évaluation
- Counterfeit SC - Stevenson 2015Document37 pagesCounterfeit SC - Stevenson 2015Ali Raza HanjraPas encore d'évaluation
- GSP Plus and Us - Why We Failed?Document4 pagesGSP Plus and Us - Why We Failed?Ali Raza HanjraPas encore d'évaluation
- Standard Bidding Documents (SBDS) For Procurement of Ophthalmology Equipment (December 2013)Document94 pagesStandard Bidding Documents (SBDS) For Procurement of Ophthalmology Equipment (December 2013)Ali Raza HanjraPas encore d'évaluation
- Final Exam Date Sheet Fall 2014Document1 pageFinal Exam Date Sheet Fall 2014Ali Raza HanjraPas encore d'évaluation
- Standard Bidding Documents (SBDS) For Procurement of Video Conferencing & Allied IT Equipment For KMC Peshawar Equipment (17.04.2013)Document213 pagesStandard Bidding Documents (SBDS) For Procurement of Video Conferencing & Allied IT Equipment For KMC Peshawar Equipment (17.04.2013)Ali Raza HanjraPas encore d'évaluation
- SPPRADocument108 pagesSPPRAAmir SangiPas encore d'évaluation
- Standard Bidding Documents (SBDS) For Procurement of DrugsDocument101 pagesStandard Bidding Documents (SBDS) For Procurement of DrugsAli Raza HanjraPas encore d'évaluation
- Pakistan Procurement Code Edition 3Document109 pagesPakistan Procurement Code Edition 3sbeg47Pas encore d'évaluation
- Agricultural Engineering Comprehensive Board Exam Reviewer: Agricultural Processing, Structures, and Allied SubjectsDocument84 pagesAgricultural Engineering Comprehensive Board Exam Reviewer: Agricultural Processing, Structures, and Allied SubjectsRachel vPas encore d'évaluation
- Instrumentation Positioner PresentationDocument43 pagesInstrumentation Positioner PresentationSangram Patnaik100% (1)
- Log File Records Startup Sequence and Rendering CallsDocument334 pagesLog File Records Startup Sequence and Rendering CallsKossay BelkhammarPas encore d'évaluation
- DNA Gel Electrophoresis Lab Solves MysteryDocument8 pagesDNA Gel Electrophoresis Lab Solves MysteryAmit KumarPas encore d'évaluation
- Bluetooth TutorialDocument349 pagesBluetooth Tutorialjohn bougsPas encore d'évaluation
- STAT455 Assignment 1 - Part ADocument2 pagesSTAT455 Assignment 1 - Part AAndyPas encore d'évaluation
- Leaked David Fry II Conversation Regarding Loopholes and Embezzlement at AFK Gamer LoungeDocument6 pagesLeaked David Fry II Conversation Regarding Loopholes and Embezzlement at AFK Gamer LoungeAnonymous iTNFz0a0Pas encore d'évaluation
- Electronics Ecommerce Website: 1) Background/ Problem StatementDocument7 pagesElectronics Ecommerce Website: 1) Background/ Problem StatementdesalegnPas encore d'évaluation
- AsiaSat 7 at 105Document14 pagesAsiaSat 7 at 105rahman200387Pas encore d'évaluation
- Customer Perceptions of Service: Mcgraw-Hill/IrwinDocument27 pagesCustomer Perceptions of Service: Mcgraw-Hill/IrwinKoshiha LalPas encore d'évaluation
- Radio Frequency Transmitter Type 1: System OperationDocument2 pagesRadio Frequency Transmitter Type 1: System OperationAnonymous qjoKrp0oPas encore d'évaluation
- Attributes and DialogsDocument29 pagesAttributes and DialogsErdenegombo MunkhbaatarPas encore d'évaluation
- Liebert PSP: Quick-Start Guide - 500VA/650VA, 230VDocument2 pagesLiebert PSP: Quick-Start Guide - 500VA/650VA, 230VsinoPas encore d'évaluation
- FX15Document32 pagesFX15Jeferson MarceloPas encore d'évaluation
- AATCC 100-2004 Assesment of Antibacterial Dinishes On Textile MaterialsDocument3 pagesAATCC 100-2004 Assesment of Antibacterial Dinishes On Textile MaterialsAdrian CPas encore d'évaluation
- Lifespan Development Canadian 6th Edition Boyd Test BankDocument57 pagesLifespan Development Canadian 6th Edition Boyd Test Bankshamekascoles2528zPas encore d'évaluation
- Iq TestDocument9 pagesIq TestAbu-Abdullah SameerPas encore d'évaluation
- 2023-Physics-Informed Radial Basis Network (PIRBN) A LocalDocument41 pages2023-Physics-Informed Radial Basis Network (PIRBN) A LocalmaycvcPas encore d'évaluation
- Three-D Failure Criteria Based on Hoek-BrownDocument5 pagesThree-D Failure Criteria Based on Hoek-BrownLuis Alonso SAPas encore d'évaluation
- تاااتتاااDocument14 pagesتاااتتاااMegdam Sameeh TarawnehPas encore d'évaluation
- Clark DietrichDocument110 pagesClark Dietrichikirby77Pas encore d'évaluation
- Briana SmithDocument3 pagesBriana SmithAbdul Rafay Ali KhanPas encore d'évaluation
- Oxford Digital Marketing Programme ProspectusDocument12 pagesOxford Digital Marketing Programme ProspectusLeonard AbellaPas encore d'évaluation
- Additional Help With OSCOLA Style GuidelinesDocument26 pagesAdditional Help With OSCOLA Style GuidelinesThabooPas encore d'évaluation
- 15 - 5 - IoT Based Smart HomeDocument6 pages15 - 5 - IoT Based Smart HomeBhaskar Rao PPas encore d'évaluation
- John Titor TIME MACHINEDocument21 pagesJohn Titor TIME MACHINEKevin Carey100% (1)
- Biology Mapping GuideDocument28 pagesBiology Mapping GuideGazar100% (1)
- Traffic LightDocument19 pagesTraffic LightDianne ParPas encore d'évaluation
- SEO-Optimized Title for Python Code Output QuestionsDocument2 pagesSEO-Optimized Title for Python Code Output QuestionsTaru GoelPas encore d'évaluation