Vous aimerez peut-être aussi
- Regenerative Medicine Applications in Organ TransplantationD'EverandRegenerative Medicine Applications in Organ TransplantationPas encore d'évaluation
- Kidney Repair and Stem Cells: A Complex and Controversial ProcessDocument8 pagesKidney Repair and Stem Cells: A Complex and Controversial ProcessTara SanderPas encore d'évaluation
- 1 B. Teknologi Sel Punca Terapi HatiDocument12 pages1 B. Teknologi Sel Punca Terapi HatiarisPas encore d'évaluation
- Materials: Scaffold Characteristics For Functional Hollow Organ RegenerationDocument23 pagesMaterials: Scaffold Characteristics For Functional Hollow Organ RegenerationroyPas encore d'évaluation
- Liver RegenerationDocument262 pagesLiver RegenerationJosé Ramírez100% (1)
- Technical ReportsDocument8 pagesTechnical ReportsalecssterPas encore d'évaluation
- Tissue EngineeringDocument12 pagesTissue EngineeringDevanand GuptaPas encore d'évaluation
- Organ Reconstruction: Dream or Reality For The Future: J.-F. Stoltz, L. Zhang, J.S. Ye and N. de IslaDocument7 pagesOrgan Reconstruction: Dream or Reality For The Future: J.-F. Stoltz, L. Zhang, J.S. Ye and N. de IslaRuxandra BadiuPas encore d'évaluation
- Regen EndoDocument88 pagesRegen EndoJitender ReddyPas encore d'évaluation
- Tissue Engineering: From Wikipedia, The Free EncyclopediaDocument12 pagesTissue Engineering: From Wikipedia, The Free EncyclopediaAnonymous ytZsBOVPas encore d'évaluation
- Tissue EngineeringDocument9 pagesTissue EngineeringbogdanotiPas encore d'évaluation
- Tissue Engineering - Wikipedia, The Free EncyclopediaDocument10 pagesTissue Engineering - Wikipedia, The Free EncyclopediaBenni WewokPas encore d'évaluation
- Tissue Engineered Urinary ConduitsDocument9 pagesTissue Engineered Urinary ConduitsNajwa PortofPas encore d'évaluation
- Anatomy (2Document25 pagesAnatomy (2Zohaib AmjadPas encore d'évaluation
- HemodialysisDocument3 pagesHemodialysisgabxyzPas encore d'évaluation
- StocumDocument5 pagesStocumLucía Carolina VidalPas encore d'évaluation
- d6e449ece855f3bbdd4ac6b61cadd242Document12 pagesd6e449ece855f3bbdd4ac6b61cadd242B VeerendrasaiPas encore d'évaluation
- Sabetkish 2020Document9 pagesSabetkish 2020asparaginaaacPas encore d'évaluation
- (Re) Building A KidneyDocument9 pages(Re) Building A KidneyUlisesPas encore d'évaluation
- Comparing the Therapeutic Potential of Stem CellsDocument30 pagesComparing the Therapeutic Potential of Stem CellsAnaaya SinghaniaPas encore d'évaluation
- Tissue EngineeringDocument8 pagesTissue EngineeringJimsPas encore d'évaluation
- Advances in Tissue EngineeringDocument10 pagesAdvances in Tissue EngineeringarisPas encore d'évaluation
- Cell Transplantation-Based Regenerative Medicine in Liver DiseasesDocument18 pagesCell Transplantation-Based Regenerative Medicine in Liver DiseasesalumnogustaPas encore d'évaluation
- Application of Tissue EngineeringDocument3 pagesApplication of Tissue Engineeringtahomag44Pas encore d'évaluation
- 2016 - Zhou Et AlDocument14 pages2016 - Zhou Et AlAfranio Cogo DestefaniPas encore d'évaluation
- J Cellular Molecular Medi - 2014 - Liu - The Multiple Functional Roles of Mesenchymal Stem Cells in Participating inDocument10 pagesJ Cellular Molecular Medi - 2014 - Liu - The Multiple Functional Roles of Mesenchymal Stem Cells in Participating indr. RiyanPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author Manuscriptbdvd1007092Pas encore d'évaluation
- Liver Regeneration by Hematopoietic Stem Cells: Have We Reached The End of The Road?Document23 pagesLiver Regeneration by Hematopoietic Stem Cells: Have We Reached The End of The Road?Morana JaganjacPas encore d'évaluation
- Ryan Agsunod Undergraduate Honors ThesisDocument51 pagesRyan Agsunod Undergraduate Honors Thesisapi-496617876Pas encore d'évaluation
- Knee Stem CellsDocument25 pagesKnee Stem CellsKN TMPas encore d'évaluation
- 2017-Ozougwuj C 2017Document13 pages2017-Ozougwuj C 2017DebPas encore d'évaluation
- Ureteral ReconstructionDocument6 pagesUreteral ReconstructiongumPas encore d'évaluation
- Metabolic Status of Pluripotent Cells Andexploitation For Growth in Stirred SuspensionbioreactorsDocument8 pagesMetabolic Status of Pluripotent Cells Andexploitation For Growth in Stirred SuspensionbioreactorsArianna CastroPas encore d'évaluation
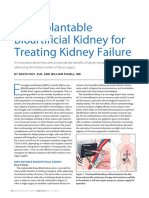
- An Implantable Bioartificial Kidney For Treating Kidney FailureDocument2 pagesAn Implantable Bioartificial Kidney For Treating Kidney FailureAnugrah Pangeran100% (1)
- CARDIOVASCULAR TISSUE ENGINEERINGDocument10 pagesCARDIOVASCULAR TISSUE ENGINEERINGArpit MaheshwariPas encore d'évaluation
- Research Article in Vitro and in VivoDocument14 pagesResearch Article in Vitro and in VivoVILEOLAGOLDPas encore d'évaluation
- Bio-artificial liver systems support acute liver failure patientsDocument8 pagesBio-artificial liver systems support acute liver failure patientsRijy LorancePas encore d'évaluation
- Basic PathologyDocument35 pagesBasic Pathologyshinichi kudoPas encore d'évaluation
- The Comprehensive Review On The Approach of Kidney Regeneration Using Stem CellsDocument10 pagesThe Comprehensive Review On The Approach of Kidney Regeneration Using Stem CellsIJRASETPublicationsPas encore d'évaluation
- 383 2018 Article 4373Document6 pages383 2018 Article 4373Anjas HappyprayogaPas encore d'évaluation
- Artículo Semana 03 InglesDocument12 pagesArtículo Semana 03 InglesSofia :DPas encore d'évaluation
- TMP AED3Document13 pagesTMP AED3FrontiersPas encore d'évaluation
- jurnal toxicDocument47 pagesjurnal toxicMuh ImranPas encore d'évaluation
- Regeneration Endodontics (1) - 1Document29 pagesRegeneration Endodontics (1) - 1شامخ شموخ الجبالPas encore d'évaluation
- J Tissue Eng Regen Med - 2016 - Stefani - A double chamber rotating bioreactor for enhanced tubular tissue generation fromDocument11 pagesJ Tissue Eng Regen Med - 2016 - Stefani - A double chamber rotating bioreactor for enhanced tubular tissue generation fromjielingPas encore d'évaluation
- @@@ Regenerating Tubular Epithelial Cells of The KidneyDocument8 pages@@@ Regenerating Tubular Epithelial Cells of The KidneyeullobaPas encore d'évaluation
- Gholobova Et Al. - Biofabrication - 2020 - Functional Evaluation of Prevascularization in One-Stage Versus Two-Stage Tissue EngineeriDocument19 pagesGholobova Et Al. - Biofabrication - 2020 - Functional Evaluation of Prevascularization in One-Stage Versus Two-Stage Tissue EngineeriLievenPas encore d'évaluation
- TherapeuticsDocument11 pagesTherapeuticsFilipa LagoaPas encore d'évaluation
- 04 Ijpscr 121 23Document7 pages04 Ijpscr 121 23BRNSS Publication Hub InfoPas encore d'évaluation
- Liver Regeneration (PDFDrive)Document261 pagesLiver Regeneration (PDFDrive)Kapetan AhavPas encore d'évaluation
- Bmri2014 473536Document10 pagesBmri2014 473536Lê HằngPas encore d'évaluation
- Tissue Engineering: Kavya Thilakan MSC Biotechnology - Semester IIIDocument23 pagesTissue Engineering: Kavya Thilakan MSC Biotechnology - Semester IIIRahul PillaiPas encore d'évaluation
- Technological Institute of The Philippines - Manila: 363 P. Casal ST., Quiapo, ManilaDocument4 pagesTechnological Institute of The Philippines - Manila: 363 P. Casal ST., Quiapo, ManilaZeny NaranjoPas encore d'évaluation
- Desenvolvimento Do FígadoDocument15 pagesDesenvolvimento Do Fígadocopiasmed semvirusPas encore d'évaluation
- Bio-Electrospraying and Cell Electrospinning: Progress and Opportunities For Basic Biology and Clinical SciencesDocument8 pagesBio-Electrospraying and Cell Electrospinning: Progress and Opportunities For Basic Biology and Clinical SciencesMarcos Vinicios Borges GaldinoPas encore d'évaluation
- The Kidneys Matter: Johannes Loffing Francois Verrey Carsten A. WagnerDocument3 pagesThe Kidneys Matter: Johannes Loffing Francois Verrey Carsten A. WagnerRania T. SabriPas encore d'évaluation
- Hemostatic factors promote liver regenerationDocument16 pagesHemostatic factors promote liver regenerationSiti Azra Khairiah LubisPas encore d'évaluation
- 74.burglary - Policy WordingDocument18 pages74.burglary - Policy WordingAyesha RalliyaPas encore d'évaluation
- AIG41313 - FINAL 3 (ENG-Single PG) - tcm4009-638392Document92 pagesAIG41313 - FINAL 3 (ENG-Single PG) - tcm4009-638392Ayesha RalliyaPas encore d'évaluation
- Administration of The Act: LegislationDocument6 pagesAdministration of The Act: LegislationAyesha RalliyaPas encore d'évaluation
- Artificial EngineeringDocument12 pagesArtificial EngineeringAyesha RalliyaPas encore d'évaluation
- SN P&P 2013 PDFDocument188 pagesSN P&P 2013 PDFMixxmixouPas encore d'évaluation
- Food Waste MalaysiaDocument4 pagesFood Waste MalaysiaAyesha RalliyaPas encore d'évaluation
- Cell Delivery Using Cell SheetDocument11 pagesCell Delivery Using Cell SheetAyesha RalliyaPas encore d'évaluation
- Presentation AyeshaDocument28 pagesPresentation AyeshaAyesha RalliyaPas encore d'évaluation
- Cell Disruption by Homogenization 3006 01-06-2008 USDocument20 pagesCell Disruption by Homogenization 3006 01-06-2008 USPrathi_Pal_8304Pas encore d'évaluation
- An Introduction To Takaful - An AlternativeDocument3 pagesAn Introduction To Takaful - An Alternativealvis2entPas encore d'évaluation
- Plant Location Factors Under 40 CharactersDocument16 pagesPlant Location Factors Under 40 CharactersAyesha RalliyaPas encore d'évaluation
- Course Outline: International Islamic University MalaysiaDocument5 pagesCourse Outline: International Islamic University MalaysiaAyesha RalliyaPas encore d'évaluation
- Safety and Loss PreventionDocument65 pagesSafety and Loss PreventionAyesha RalliyaPas encore d'évaluation
- Recycled Organic Waste As Animal Feed PFPDocument4 pagesRecycled Organic Waste As Animal Feed PFPAyesha RalliyaPas encore d'évaluation
- Animal FeedDocument106 pagesAnimal FeedAyesha Ralliya100% (2)
- Bioreactor Monitoring & Control GuideDocument51 pagesBioreactor Monitoring & Control GuideAyesha RalliyaPas encore d'évaluation
- Ideal Bioreactor EngineeringDocument60 pagesIdeal Bioreactor EngineeringAyesha RalliyaPas encore d'évaluation
- Course Outline: International Islamic University MalaysiaDocument5 pagesCourse Outline: International Islamic University MalaysiaAyesha RalliyaPas encore d'évaluation
- Eng Econ - Inv An N BEP - L9Document31 pagesEng Econ - Inv An N BEP - L9Ayesha RalliyaPas encore d'évaluation
- Eng Econ - Cash - Flow - L3 - MME 4272Document55 pagesEng Econ - Cash - Flow - L3 - MME 4272Ayesha RalliyaPas encore d'évaluation
- Eng Econ - Cash - Flow - L3 - MME 4272Document55 pagesEng Econ - Cash - Flow - L3 - MME 4272Ayesha RalliyaPas encore d'évaluation
- Eng Econ MGT Ratios L2 - MME 4272Document41 pagesEng Econ MGT Ratios L2 - MME 4272Ayesha RalliyaPas encore d'évaluation
- Organizational Structure: Ref. Contemporary Management, 3 Ed Gareth R. Jones Jennifer M. George Mcgraw-HillDocument39 pagesOrganizational Structure: Ref. Contemporary Management, 3 Ed Gareth R. Jones Jennifer M. George Mcgraw-HillAyesha RalliyaPas encore d'évaluation
- Eng Econ Deprec L10Document29 pagesEng Econ Deprec L10Ayesha RalliyaPas encore d'évaluation
- Eng Econ Deprec L10Document29 pagesEng Econ Deprec L10Ayesha RalliyaPas encore d'évaluation
- Eng Econ - Inv An N BEP - L9Document31 pagesEng Econ - Inv An N BEP - L9Ayesha RalliyaPas encore d'évaluation
- Chap 2 Polymer & CompositesDocument18 pagesChap 2 Polymer & CompositesAyesha RalliyaPas encore d'évaluation
- Revised Chemical KineticsDocument36 pagesRevised Chemical KineticsAyesha RalliyaPas encore d'évaluation
- Eng Econ Cash Flow L4 - MME 4272Document43 pagesEng Econ Cash Flow L4 - MME 4272Ayesha RalliyaPas encore d'évaluation
- National Mediclaim Policy: BrochureDocument3 pagesNational Mediclaim Policy: Brochureshukla8Pas encore d'évaluation
- Pressure Ulcers and Wound CareDocument52 pagesPressure Ulcers and Wound CareKarina Mega WPas encore d'évaluation
- Synergy CementlessDocument32 pagesSynergy CementlessSergiu Plesca100% (1)
- Minimally Invasive Shoulder and Elbow Surgery - W. Levine, Et Al., (Informa, 2007) WWDocument408 pagesMinimally Invasive Shoulder and Elbow Surgery - W. Levine, Et Al., (Informa, 2007) WWGeo SanchezPas encore d'évaluation
- Family Coping IndexDocument5 pagesFamily Coping IndexDarcey NicholePas encore d'évaluation
- Gram Negative RodsDocument23 pagesGram Negative RodsYasir KareemPas encore d'évaluation
- AntacidsDocument2 pagesAntacidsMa Corazon MelecioPas encore d'évaluation
- Pain47, 295Document4 pagesPain47, 295Ezel RitmoPas encore d'évaluation
- Bacillus Pumilus - MicrobewikiDocument4 pagesBacillus Pumilus - MicrobewikiAleivi PérezPas encore d'évaluation
- Safety and Efficacy of Vinyl Bags in Prevention of Hypothermia of Preterm Neonates at BirthDocument3 pagesSafety and Efficacy of Vinyl Bags in Prevention of Hypothermia of Preterm Neonates at BirthArgadia YuniriyadiPas encore d'évaluation
- 2.0 Classification of Mental DisordersDocument3 pages2.0 Classification of Mental DisordersJohnBenedictRazPas encore d'évaluation
- Neurofeedback ResearchDocument50 pagesNeurofeedback Researchdocs1234567Pas encore d'évaluation
- Research Proposal Power Point PresentationDocument24 pagesResearch Proposal Power Point PresentationSithara JayatungaPas encore d'évaluation
- 10 1097@CCM 0b013e31818b35f2Document7 pages10 1097@CCM 0b013e31818b35f2omarihuanoPas encore d'évaluation
- Peritoneum 2022Document86 pagesPeritoneum 2022Tayyib KhanPas encore d'évaluation
- PE.4 - BPEd2NUÑEZ, MYRADocument25 pagesPE.4 - BPEd2NUÑEZ, MYRANuñez MyraPas encore d'évaluation
- Paper For Enzyme ActivityDocument7 pagesPaper For Enzyme ActivityFar hatPas encore d'évaluation
- NCM 116 Course SyllabusDocument21 pagesNCM 116 Course SyllabusMagne CharliePas encore d'évaluation
- What Is Bronchitis 2Document3 pagesWhat Is Bronchitis 2lea jumawanPas encore d'évaluation
- FACTORS AFFECTING THE PUBLIC SPEAKING FA - OdtDocument16 pagesFACTORS AFFECTING THE PUBLIC SPEAKING FA - OdtKenneth BitunPas encore d'évaluation
- Antisense Oligonucleotide Biotechnology, Applications and FutureDocument29 pagesAntisense Oligonucleotide Biotechnology, Applications and FuturesurojitarpitaPas encore d'évaluation
- NLE 2015 Questions SampleDocument8 pagesNLE 2015 Questions SampleJona Suarez100% (4)
- 2004 2005 Magnetom Flash 2 2Document64 pages2004 2005 Magnetom Flash 2 2Herick SavionePas encore d'évaluation
- Salicylates Tca ToxicityDocument54 pagesSalicylates Tca Toxicityapi-298936498Pas encore d'évaluation
- Seminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Document34 pagesSeminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Meraol HusseinPas encore d'évaluation
- 21 Top Orthopedic Tests PDFDocument27 pages21 Top Orthopedic Tests PDFLaraib Mirza100% (1)
- 1577un 2026-01Document79 pages1577un 2026-01ngovantienPas encore d'évaluation
- Parents of Episcopal School of Jacksonville Students File Lawsuit Over Mask MandateDocument32 pagesParents of Episcopal School of Jacksonville Students File Lawsuit Over Mask MandateActionNewsJaxPas encore d'évaluation
- Module 8 - Diversity of Microbial World: Lecture 1-Microbial Taxonomy and PhylogenyDocument27 pagesModule 8 - Diversity of Microbial World: Lecture 1-Microbial Taxonomy and PhylogenyDr. P.V.Kamala KumariPas encore d'évaluation
- 3.blood Pressure and Its RegulationDocument44 pages3.blood Pressure and Its RegulationNatasha Grace NtembwaPas encore d'évaluation