Vous aimerez peut-être aussi
- IBM Maximo Asset Configuration Manager A Complete Guide - 2020 EditionD'EverandIBM Maximo Asset Configuration Manager A Complete Guide - 2020 EditionPas encore d'évaluation
- Failure AnalysisDocument23 pagesFailure AnalysisMaruan MuhammadPas encore d'évaluation
- Failure Mode Effects and Criticality Analysis PDFDocument2 pagesFailure Mode Effects and Criticality Analysis PDFMacPas encore d'évaluation
- Reporting and Analyzing Occurrences: The DOE StandardDocument123 pagesReporting and Analyzing Occurrences: The DOE StandardMarco RangelPas encore d'évaluation
- Fault Tree DiagramDocument7 pagesFault Tree DiagramSri NivasPas encore d'évaluation
- Subject: Production and Operations Management Unit 5: Maintenance and Waste ManagementDocument19 pagesSubject: Production and Operations Management Unit 5: Maintenance and Waste ManagementAnonymous yL88Jj100% (1)
- 23 Design Assurance PlanDocument2 pages23 Design Assurance PlanBau2NinePas encore d'évaluation
- IMM ManualDocument59 pagesIMM ManualeyoboldairPas encore d'évaluation
- Fmea PDFDocument36 pagesFmea PDFalsoraya00100% (1)
- OM Manuals TemplateDocument9 pagesOM Manuals TemplatejanempatricioPas encore d'évaluation
- Failure Mode and Effect Analysis (FMEA)Document23 pagesFailure Mode and Effect Analysis (FMEA)Parandhaman GRPas encore d'évaluation
- Criticality Analysis Maintenance ProceduresDocument4 pagesCriticality Analysis Maintenance ProceduresjfejfePas encore d'évaluation
- Fault Tree Analysis Template ExcelDocument5 pagesFault Tree Analysis Template Excelvbvis25Pas encore d'évaluation
- CPMS-AUT-EP-002 - Instrument and Controls Philosophy GuidelinesDocument18 pagesCPMS-AUT-EP-002 - Instrument and Controls Philosophy GuidelinesChrisPas encore d'évaluation
- Process Capability BaselineDocument19 pagesProcess Capability BaselinecamilaskishorePas encore d'évaluation
- Maintenance Management System Guideline For Maintenance Operating Procedures Maintenance Work ManagementDocument29 pagesMaintenance Management System Guideline For Maintenance Operating Procedures Maintenance Work ManagementGlad BlazPas encore d'évaluation
- Mod 5 01 Cause&Effect Mar 02Document20 pagesMod 5 01 Cause&Effect Mar 02drustagiPas encore d'évaluation
- FMECA: Failure Mode and Effect Criticality AnalysisDocument5 pagesFMECA: Failure Mode and Effect Criticality AnalysisGayathri Ragunathan0% (1)
- Welcome - Day 3: Failure Mode and Effects AnalysisDocument48 pagesWelcome - Day 3: Failure Mode and Effects AnalysisSanjeev SharmaPas encore d'évaluation
- Case Study - Sabic Shutdown Optimisation PDFDocument8 pagesCase Study - Sabic Shutdown Optimisation PDFArielPas encore d'évaluation
- 10 Steps To Asset CareDocument13 pages10 Steps To Asset CareDamianPas encore d'évaluation
- A Two-Stage Failure Mode and Effect Analysis of Offshore Wind Turbines - 2020Document24 pagesA Two-Stage Failure Mode and Effect Analysis of Offshore Wind Turbines - 2020johnPas encore d'évaluation
- Xfmea Report Sample - Machinery FMEA: in Addition To This Summary, This Report Includes The Following FormsDocument6 pagesXfmea Report Sample - Machinery FMEA: in Addition To This Summary, This Report Includes The Following FormsRoland JoldisPas encore d'évaluation
- Iso22000 2005Document48 pagesIso22000 2005STELLA MARISPas encore d'évaluation
- CMMSDocument9 pagesCMMSHanna Rizanti KartinaPas encore d'évaluation
- FMEADocument20 pagesFMEARonillo PormonPas encore d'évaluation
- FMEA Quality Audit Procedure PDFDocument5 pagesFMEA Quality Audit Procedure PDFsoft52Pas encore d'évaluation
- AIMS Training (July 31, 2024)Document4 pagesAIMS Training (July 31, 2024)Arianta RianPas encore d'évaluation
- RBI Assessment Recommended Work-Ing ProcessDocument1 pageRBI Assessment Recommended Work-Ing ProcessRicardoPas encore d'évaluation
- Efficient Material Flow Assembly LinesDocument161 pagesEfficient Material Flow Assembly LinesHoussem MoujahedPas encore d'évaluation
- Asset Data Management for Energy Sector Hose SafetyDocument2 pagesAsset Data Management for Energy Sector Hose Safetyjson_gabionPas encore d'évaluation
- Reliability Engineering Processes and Root Cause AnalysisDocument13 pagesReliability Engineering Processes and Root Cause AnalysisarslanhamidPas encore d'évaluation
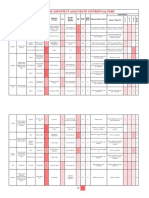
- Failure Mode and Effect Analysis of Centrifugal PumpDocument2 pagesFailure Mode and Effect Analysis of Centrifugal PumpHAFIZMUHAMMAD SAJIDPas encore d'évaluation
- CFUSA Supplier HandbookDocument24 pagesCFUSA Supplier HandbookBrenda GillPas encore d'évaluation
- 02-QGG CS Functional Location UATDocument8 pages02-QGG CS Functional Location UATAbd El Rhman MostafaPas encore d'évaluation
- Journal of Quality in Maintenance EngineeringDocument20 pagesJournal of Quality in Maintenance EngineeringJose100% (1)
- PFMEA Process Failure Mode and Effect Analysis for Distribution AssemblyDocument50 pagesPFMEA Process Failure Mode and Effect Analysis for Distribution AssemblySameer SaxenaPas encore d'évaluation
- Evaluating FMEA, FMECA and FMEDADocument6 pagesEvaluating FMEA, FMECA and FMEDAZakaria RadaPas encore d'évaluation
- Integrity Engineering - Wikipedia PDFDocument24 pagesIntegrity Engineering - Wikipedia PDFEndhy Wisnu NovindraPas encore d'évaluation
- Samples 033 ADocument33 pagesSamples 033 AWekesa CalebPas encore d'évaluation
- CMMS Technical Object and Preventative Maintenance FormDocument7 pagesCMMS Technical Object and Preventative Maintenance Formken1962Pas encore d'évaluation
- Engineering Design Review and ChecklistDocument40 pagesEngineering Design Review and ChecklistwnaciPas encore d'évaluation
- Failure Mode and Effect Criticality Analysis FMECADocument14 pagesFailure Mode and Effect Criticality Analysis FMECARaedyAnwarPas encore d'évaluation
- Total Motor Management in 40 CharactersDocument6 pagesTotal Motor Management in 40 CharactersWilson PinacatePas encore d'évaluation
- ECR ProcedureDocument9 pagesECR ProcedureJHBernardoPas encore d'évaluation
- Measuring Bearing Currents & Shaft Voltages in Electric MotorsDocument59 pagesMeasuring Bearing Currents & Shaft Voltages in Electric Motorselectrical100% (1)
- HAZOP Study Data RequirementsDocument5 pagesHAZOP Study Data RequirementsRonak MotaPas encore d'évaluation
- Fme (C) ADocument4 pagesFme (C) AMurat IslamPas encore d'évaluation
- A Review of RequirementsDocument7 pagesA Review of RequirementsPedroSotoPas encore d'évaluation
- QA Processes, Tools and Metrics: Group 1Document18 pagesQA Processes, Tools and Metrics: Group 1Rhea AgulayPas encore d'évaluation
- Article Failure AnalysisDocument25 pagesArticle Failure AnalysisMd KalamuddinPas encore d'évaluation
- 4.5 May2019-Repairable SystemDocument10 pages4.5 May2019-Repairable SystemAlexander GejetanusPas encore d'évaluation
- Maintainance ManagementDocument8 pagesMaintainance ManagementThomas P Vacha100% (1)
- FMEA MSETM 5291 2bDocument17 pagesFMEA MSETM 5291 2boualidhsePas encore d'évaluation
- Performance-based maintenance of concrete structuresDocument12 pagesPerformance-based maintenance of concrete structuresMuhammad AyyazPas encore d'évaluation
- Reference Documents IEC Standard 812 Procedure For Failure Mode andDocument5 pagesReference Documents IEC Standard 812 Procedure For Failure Mode andtopkayaPas encore d'évaluation
- Fundamentals of FMEA PDFDocument35 pagesFundamentals of FMEA PDFPriatna suheriPas encore d'évaluation
- Supplier QuestionnaireDocument5 pagesSupplier QuestionnaireNikhil Bhat InanjaiPas encore d'évaluation
- PETA-7.1 Step DescriptionDocument44 pagesPETA-7.1 Step DescriptionNack Abd RauofPas encore d'évaluation
- Template Assignment 2 2015Document7 pagesTemplate Assignment 2 2015yashar2500Pas encore d'évaluation
- Design ProcessesDocument13 pagesDesign Processesyashar2500Pas encore d'évaluation
- Sim.I.am - A Robot SimulatorDocument27 pagesSim.I.am - A Robot Simulatoryashar2500Pas encore d'évaluation
- Control of Mobile Robots: Glue Lectures: InstructorDocument9 pagesControl of Mobile Robots: Glue Lectures: Instructoryashar2500Pas encore d'évaluation
- Trig Cheat Sheet ReducedDocument2 pagesTrig Cheat Sheet ReducedMritunjay KumarPas encore d'évaluation
- Physical Computing101: Part 2: Control of Mobile Robots: Hardware Lecture #6Document7 pagesPhysical Computing101: Part 2: Control of Mobile Robots: Hardware Lecture #6yashar2500Pas encore d'évaluation
- Conrob-002 Wiki HardwareDocument6 pagesConrob-002 Wiki Hardwareyashar2500Pas encore d'évaluation
- Template Assignment 1Document4 pagesTemplate Assignment 1yashar2500Pas encore d'évaluation
- DDA MOOC Syllabus 2015.2Document18 pagesDDA MOOC Syllabus 2015.2yashar2500Pas encore d'évaluation
- Physical Computing101: Part 3: Control of Mobile Robots: Hardware Lecture #7Document8 pagesPhysical Computing101: Part 3: Control of Mobile Robots: Hardware Lecture #7yashar2500Pas encore d'évaluation
- Quiz 7 SolutionsDocument6 pagesQuiz 7 Solutionsyashar2500100% (2)
- Programming & Simulation Lecture 7 SlidesDocument11 pagesProgramming & Simulation Lecture 7 Slidesyashar2500Pas encore d'évaluation
- Sim.I.am - A Robot SimulatorDocument27 pagesSim.I.am - A Robot Simulatoryashar2500Pas encore d'évaluation
- Module 7 SlidesDocument54 pagesModule 7 Slidesyashar2500Pas encore d'évaluation
- GLUE LECTURE 6 - Vectors For Naviga8on: (This Will Be Helpful For Quiz 6!)Document37 pagesGLUE LECTURE 6 - Vectors For Naviga8on: (This Will Be Helpful For Quiz 6!)jcvoscribPas encore d'évaluation
- Quiz 6 SolutionsDocument3 pagesQuiz 6 Solutionsyashar2500100% (2)
- Module 6 SlidesDocument55 pagesModule 6 Slidesyashar2500Pas encore d'évaluation
- Conrob-Programming - assignmoents-MOOC Control of Mobile Robots Simulation Lecture 6Document10 pagesConrob-Programming - assignmoents-MOOC Control of Mobile Robots Simulation Lecture 6jcvoscribPas encore d'évaluation
- Physical Computing101: Part 1: Control of Mobile Robots: Hardware Lecture #5Document6 pagesPhysical Computing101: Part 1: Control of Mobile Robots: Hardware Lecture #5yashar2500Pas encore d'évaluation
- Sim.I.am - A Robot SimulatorDocument27 pagesSim.I.am - A Robot Simulatoryashar2500Pas encore d'évaluation
- Module 5 SlidesDocument53 pagesModule 5 Slidesyashar2500Pas encore d'évaluation
- Conrob-Programming - assignmentso-MOOC Control of Mobile Robots Simulation Lecture 5Document10 pagesConrob-Programming - assignmentso-MOOC Control of Mobile Robots Simulation Lecture 5jcvoscribPas encore d'évaluation
- Sim.I.am - A Robot SimulatorDocument27 pagesSim.I.am - A Robot Simulatoryashar2500Pas encore d'évaluation
- Quiz 5 SolutionsDocument5 pagesQuiz 5 Solutionsyashar250067% (6)
- Conrob-002 Wiki HardwareDocument6 pagesConrob-002 Wiki Hardwareyashar2500Pas encore d'évaluation
- Control of Mobile Robots: Glue Lectures: InstructorDocument23 pagesControl of Mobile Robots: Glue Lectures: Instructoryashar2500Pas encore d'évaluation
- Glue Lecture 5 SlidesDocument12 pagesGlue Lecture 5 Slidesyashar2500Pas encore d'évaluation
- Hardware Lecture 4 SlidesDocument16 pagesHardware Lecture 4 Slidesyashar2500Pas encore d'évaluation
- MOOC Control of Mobile Robots Simulation Lecture 4Document13 pagesMOOC Control of Mobile Robots Simulation Lecture 4jcvoscribPas encore d'évaluation
- Quiz 4 SolutionsDocument4 pagesQuiz 4 Solutionsjcvoscrib89% (9)
- Chapter 5 Thesis Sample QualitativeDocument8 pagesChapter 5 Thesis Sample Qualitativeqpftgehig100% (2)
- GATE-17 Online Test Series Mechanical Engineering - ACE Engineering AcademyDocument8 pagesGATE-17 Online Test Series Mechanical Engineering - ACE Engineering AcademykkkPas encore d'évaluation
- Karla Armbruster Is Assistant Professor of English at Webster UniversityDocument5 pagesKarla Armbruster Is Assistant Professor of English at Webster UniversityIoan DorinPas encore d'évaluation
- Convolution and CorrelationDocument11 pagesConvolution and CorrelationSHYAMPas encore d'évaluation
- Operation of SignalsDocument8 pagesOperation of SignalsBenjhon S. ElarcosaPas encore d'évaluation
- VHDL Code Examples for DAC Controller and Thyristor Pulse GeneratorDocument6 pagesVHDL Code Examples for DAC Controller and Thyristor Pulse Generatormrandres7Pas encore d'évaluation
- Yekatit 23 Math WorksheetDocument4 pagesYekatit 23 Math WorksheetAnwar AliPas encore d'évaluation
- Stem 11 10 GR 1 Acaso Arandid Aumentado BalindDocument7 pagesStem 11 10 GR 1 Acaso Arandid Aumentado BalindPsycho The GreatestPas encore d'évaluation
- Geostatistics article from American StatisticianDocument7 pagesGeostatistics article from American StatisticianDilson David Ramirez ForeroPas encore d'évaluation
- Assignment - I: AnswerDocument5 pagesAssignment - I: AnswerSweta UmraoPas encore d'évaluation
- Work SheetDocument1 pageWork SheetPeter HuaPas encore d'évaluation
- Course Outline Fall20232024Document2 pagesCourse Outline Fall20232024ibahtainePas encore d'évaluation
- Introduction To Case Studies - The Yin ApproachDocument20 pagesIntroduction To Case Studies - The Yin ApproachKim Francis TanayPas encore d'évaluation
- Operations Research Multiple Choice Questions: B. ScientificDocument25 pagesOperations Research Multiple Choice Questions: B. ScientificBilal AhmedPas encore d'évaluation
- Metric Tolerances ReferenceDocument11 pagesMetric Tolerances ReferenceGirish Khanna VeshalaPas encore d'évaluation
- Classification of Analytical Methods Not MineDocument20 pagesClassification of Analytical Methods Not MineMark Cliffton BadlonPas encore d'évaluation
- Understanding Bda PaperDocument9 pagesUnderstanding Bda PaperKennyPas encore d'évaluation
- MATLAB Examples - OptimizationDocument15 pagesMATLAB Examples - OptimizationClayssaNelPas encore d'évaluation
- Probability Theory and Stochastic ProcessDocument9 pagesProbability Theory and Stochastic Processms_aramanaPas encore d'évaluation
- Signal Theory Mid Term-I - MtechDocument2 pagesSignal Theory Mid Term-I - MtechihbrusansuharshPas encore d'évaluation
- 16.21 Techniques of Structural Analysis and Design Spring 2003 Unit #1Document4 pages16.21 Techniques of Structural Analysis and Design Spring 2003 Unit #1kbhattacPas encore d'évaluation
- AppliedStatistics PDFDocument401 pagesAppliedStatistics PDFJINSO VACAPas encore d'évaluation
- Mathematics IV SEMDocument3 pagesMathematics IV SEMram_somalaPas encore d'évaluation
- Department of Mathematics Anna University, Chennai Ma5252 Engineering Mathematics-Ii Unit - III Complex IntegrationDocument36 pagesDepartment of Mathematics Anna University, Chennai Ma5252 Engineering Mathematics-Ii Unit - III Complex IntegrationThushiyanth KPas encore d'évaluation
- Dhaka International University: Department of CSE (1 Shift)Document2 pagesDhaka International University: Department of CSE (1 Shift)SakilPas encore d'évaluation
- Number Theory SyllabusDocument77 pagesNumber Theory SyllabusKring RossePas encore d'évaluation
- Ode2 PDFDocument1 pageOde2 PDFVaibhavBhagatPas encore d'évaluation
- Outline of A New Approach To The Analysis of Complex Systems and Decision Processes Article RevisionDocument3 pagesOutline of A New Approach To The Analysis of Complex Systems and Decision Processes Article RevisionDamián Abalo MirónPas encore d'évaluation
- Design ControllerDocument34 pagesDesign ControllerMaezinha_MarinelaPas encore d'évaluation
- Surah Luqman ExolanationDocument101 pagesSurah Luqman ExolanationAtif Ali Anwar FastNUPas encore d'évaluation