Vous aimerez peut-être aussi
- Status Amputasi: I. Identity II. AnamnesisDocument2 pagesStatus Amputasi: I. Identity II. Anamnesisarya091193Pas encore d'évaluation
- Thuasne Practical Guide 2005Document23 pagesThuasne Practical Guide 2005arya091193Pas encore d'évaluation
- Pathophysiology of Septic ShockDocument19 pagesPathophysiology of Septic ShockRoberto López MataPas encore d'évaluation
- 3041 BrochureDocument5 pages3041 Brochurearya091193Pas encore d'évaluation
- Thuasne Practical Guide 2005Document23 pagesThuasne Practical Guide 2005arya091193Pas encore d'évaluation
- Thuasne Practical Guide 2005Document23 pagesThuasne Practical Guide 2005arya091193Pas encore d'évaluation
- GaghagahaghagahDocument1 pageGaghagahaghagaharya091193Pas encore d'évaluation
- GaghagahaghagahDocument1 pageGaghagahaghagaharya091193Pas encore d'évaluation
- GaghagahaghagahDocument1 pageGaghagahaghagaharya091193Pas encore d'évaluation
- GaghagahaghagahDocument1 pageGaghagahaghagaharya091193Pas encore d'évaluation
- Topicsheet KorsakoffDocument3 pagesTopicsheet Korsakoffarya091193Pas encore d'évaluation
- GaghagahaghagahDocument1 pageGaghagahaghagaharya091193Pas encore d'évaluation
- Mechan in 2012 Cmef ShenzhenDocument11 pagesMechan in 2012 Cmef Shenzhenarya091193Pas encore d'évaluation
- Dudonan Jero MangkuDocument1 pageDudonan Jero Mangkuarya091193Pas encore d'évaluation
- Clinical Study: Overjet and Overbite Influence On Cyclic Masticatory Movements: A CT StudyDocument7 pagesClinical Study: Overjet and Overbite Influence On Cyclic Masticatory Movements: A CT Studyarya091193Pas encore d'évaluation
- Karnofsky SkorDocument1 pageKarnofsky SkorEka LosPas encore d'évaluation
- 114 429 1 PBDocument5 pages114 429 1 PBarya091193Pas encore d'évaluation
- 04 JerolimovDocument25 pages04 Jerolimovarya091193Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Tammy Georgian GibsonDocument2 pagesTammy Georgian GibsonThe News-HeraldPas encore d'évaluation
- Student Services Strategic Planning Framework ReportDocument9 pagesStudent Services Strategic Planning Framework ReportManoj TI , KAUPas encore d'évaluation
- June 2015 QP - Unit 2 Edexcel Biology A-LevelDocument28 pagesJune 2015 QP - Unit 2 Edexcel Biology A-LevelSimonChanPas encore d'évaluation
- Fundamentals of Accounting 1 (Week 4) OnlineDocument14 pagesFundamentals of Accounting 1 (Week 4) OnlineElla Blanca BuyaPas encore d'évaluation
- 05 - Task - Performance (2) UtsDocument3 pages05 - Task - Performance (2) Utsaby mariePas encore d'évaluation
- PawsonDocument7 pagesPawsonozzy22Pas encore d'évaluation
- Take Off - Workbook PDFDocument108 pagesTake Off - Workbook PDFSam Love0% (1)
- GR 5 Term 1 2019 Ns T Lesson PlanDocument172 pagesGR 5 Term 1 2019 Ns T Lesson PlanLorraine NoloPas encore d'évaluation
- Nce Practice TestDocument58 pagesNce Practice Testdakotalake80% (10)
- P Process BrochureDocument20 pagesP Process BrochureHilda NuruzzamanPas encore d'évaluation
- Block Syllabus S. ST Grade 5 FIRST TERM 2024Document4 pagesBlock Syllabus S. ST Grade 5 FIRST TERM 2024fatimaijaz928Pas encore d'évaluation
- Research ProposalDocument16 pagesResearch ProposalNathanPas encore d'évaluation
- Visual Literacy MatrixDocument2 pagesVisual Literacy MatrixernsteinsPas encore d'évaluation
- Mark Scheme Summer 2008: IGCSE Mathematics (4400)Document46 pagesMark Scheme Summer 2008: IGCSE Mathematics (4400)Tammachat DumrongjakPas encore d'évaluation
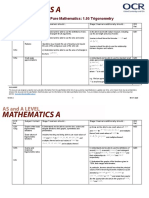
- Teacher Delivery Guide Pure Mathematics: 1.05 TrigonometryDocument16 pagesTeacher Delivery Guide Pure Mathematics: 1.05 TrigonometryHubert SelormeyPas encore d'évaluation
- Activity Learning Sheets in Oral - Com - TYPES OF SPEECH CONTEXT - Guinsaugon High SchoolDocument5 pagesActivity Learning Sheets in Oral - Com - TYPES OF SPEECH CONTEXT - Guinsaugon High SchoolCatzMacedaMeekPas encore d'évaluation
- Cricitical Journal Review 'Educational Psychology': Lecture: Prof. Dr. Ibnu Hajar, M.Si. Rizki Ramadhan S.PD, M.PDDocument21 pagesCricitical Journal Review 'Educational Psychology': Lecture: Prof. Dr. Ibnu Hajar, M.Si. Rizki Ramadhan S.PD, M.PDRahma disaPas encore d'évaluation
- Sing A Joyful Song - PREVIEWDocument5 pagesSing A Joyful Song - PREVIEWRonilo, Jr. CalunodPas encore d'évaluation
- How To Use Batch Normalization With TensorFlow and TF - Keras To Train Deep Neural Networks FasterDocument11 pagesHow To Use Batch Normalization With TensorFlow and TF - Keras To Train Deep Neural Networks FastersusanPas encore d'évaluation
- Orphanage ThesisDocument15 pagesOrphanage Thesishannah marvilla0% (1)
- Ten Health Benefits of Getting A Good Nights SleepDocument5 pagesTen Health Benefits of Getting A Good Nights SleepAngelica CiubalPas encore d'évaluation
- A Study On Operational and Financial Performance of Canara BankDocument11 pagesA Study On Operational and Financial Performance of Canara Bankshrivathsa upadhyayaPas encore d'évaluation
- Godrej Interio Education Range Dossier 2023-24 - v1 WebDocument138 pagesGodrej Interio Education Range Dossier 2023-24 - v1 WebSingareni power training Institute (SPTI)Pas encore d'évaluation
- Sword of The Spirit at Franciscan UniversityDocument11 pagesSword of The Spirit at Franciscan UniversityJohn Flaherty100% (1)
- Artificial IntelligenceDocument2 pagesArtificial IntelligenceBarodianbikerniPas encore d'évaluation
- 1 Ms Exam Myself and My FamilyDocument2 pages1 Ms Exam Myself and My Familyasma sakoraPas encore d'évaluation
- 2022-2023 ENGLISH Elementary HandbookDocument128 pages2022-2023 ENGLISH Elementary HandbookMike M JFPas encore d'évaluation
- Interview Schedule For MothersDocument5 pagesInterview Schedule For MothersArun Kumar SinghPas encore d'évaluation
- Impact of Emotional Intelligence and Work Life Integration On Job StressDocument10 pagesImpact of Emotional Intelligence and Work Life Integration On Job StressDr.Ramar VeluchamyPas encore d'évaluation
- IC3e Book3 To GIU-BGIU-WorkbooksDocument7 pagesIC3e Book3 To GIU-BGIU-WorkbooksTâm XinhPas encore d'évaluation