Vous aimerez peut-être aussi
- Icd XDocument1 pageIcd XHerpika DianaPas encore d'évaluation
- Caffeine Bone CalciumDocument8 pagesCaffeine Bone CalciumHerpika DianaPas encore d'évaluation
- Stress and The Periodontium: Review Article 10.5005/jp-Journals-10031-1005Document3 pagesStress and The Periodontium: Review Article 10.5005/jp-Journals-10031-1005Herpika DianaPas encore d'évaluation
- Dr. Nikita AgrawalDocument4 pagesDr. Nikita AgrawalHerpika DianaPas encore d'évaluation
- Green Tea Extract For Periodontal Health: Review ArticleDocument5 pagesGreen Tea Extract For Periodontal Health: Review ArticleHerpika DianaPas encore d'évaluation
- Dr. Karam Abu Shakra 42-10Document8 pagesDr. Karam Abu Shakra 42-10Herpika DianaPas encore d'évaluation
- The Cariostatic Potential of Cheese: Cooked Cheese-Containing Meals Increase Plaque Calcium ConcentrationDocument4 pagesThe Cariostatic Potential of Cheese: Cooked Cheese-Containing Meals Increase Plaque Calcium ConcentrationHerpika DianaPas encore d'évaluation
- Effects of Self-Ligating and Conventional Brackets On Halitosis and Periodontal ConditionsDocument6 pagesEffects of Self-Ligating and Conventional Brackets On Halitosis and Periodontal ConditionsHerpika DianaPas encore d'évaluation
- A Comparative Study of Acidogenic Potential of Milk and Commonly Used Milk FormulaeDocument3 pagesA Comparative Study of Acidogenic Potential of Milk and Commonly Used Milk FormulaeHerpika DianaPas encore d'évaluation
- Understanding Stress and TMJ Dysfunction: What Causes TMJ Problems? How Can Physical Therapy Help TMJ Sufferers?Document2 pagesUnderstanding Stress and TMJ Dysfunction: What Causes TMJ Problems? How Can Physical Therapy Help TMJ Sufferers?Herpika DianaPas encore d'évaluation
- Jop 2005 03 s0189Document1 pageJop 2005 03 s0189Herpika DianaPas encore d'évaluation
- Effect of Mastication On Human Brain Activity: Kiwako Sakamoto, Hiroki Nakata, Masato Yumoto, Ryusuke KakigiDocument8 pagesEffect of Mastication On Human Brain Activity: Kiwako Sakamoto, Hiroki Nakata, Masato Yumoto, Ryusuke KakigiHerpika DianaPas encore d'évaluation
- Evaluation of Temporomandibular Joint in Stress-Free PatientsDocument5 pagesEvaluation of Temporomandibular Joint in Stress-Free PatientsHerpika DianaPas encore d'évaluation
- Investigation On Two-Body Abrasive Wear Behavior of Silicon Carbide Filled Glass Fabric-Epoxy CompositesDocument16 pagesInvestigation On Two-Body Abrasive Wear Behavior of Silicon Carbide Filled Glass Fabric-Epoxy CompositesHerpika DianaPas encore d'évaluation
- Osteoma 1Document3 pagesOsteoma 1Herpika DianaPas encore d'évaluation
- An Expanded Odontogenic Myxoma in MaxillaDocument7 pagesAn Expanded Odontogenic Myxoma in MaxillaHerpika DianaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Chap5-7 National Book Foundation 9th Class Conceptual QuestionsDocument7 pagesChap5-7 National Book Foundation 9th Class Conceptual QuestionsWaleed Nasir100% (1)
- Quantum PauseDocument5 pagesQuantum Pausesoulsearch67641100% (2)
- PWC Taxavvy 18 2020 Mco PDFDocument12 pagesPWC Taxavvy 18 2020 Mco PDFMichael YapPas encore d'évaluation
- 6 Cathay vs. VazquezDocument2 pages6 Cathay vs. VazquezErwin BernardinoPas encore d'évaluation
- Dolomite in Manila Bay A Big HitDocument3 pagesDolomite in Manila Bay A Big HitJoanaPauline FloresPas encore d'évaluation
- Look 4 - Unit 4Document14 pagesLook 4 - Unit 4Noura AdhamPas encore d'évaluation
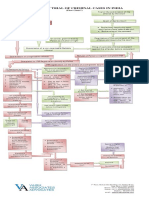
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Sara Lee: A Tale of Another Turnaround: Case Analysis - Strategic ManagementDocument6 pagesSara Lee: A Tale of Another Turnaround: Case Analysis - Strategic ManagementKeerthi PurushothamanPas encore d'évaluation
- Fig. 6.14 Circular WaveguideDocument16 pagesFig. 6.14 Circular WaveguideThiagu RajivPas encore d'évaluation
- Tolkien Essay-TreesDocument10 pagesTolkien Essay-Treesapi-657753727Pas encore d'évaluation
- Igice Cya Kabiri: 2.0. Intambwe Zitandukanye Z'Imikorere Ya Mariyamu KinyamaruraDocument7 pagesIgice Cya Kabiri: 2.0. Intambwe Zitandukanye Z'Imikorere Ya Mariyamu KinyamaruraJacques Abimanikunda BarahirwaPas encore d'évaluation
- Soal Dan Pembahasan Grammar Lat TOEP 1Document6 pagesSoal Dan Pembahasan Grammar Lat TOEP 1Abdur100% (2)
- Creative WritingDocument13 pagesCreative WritingBeberly Kim AmaroPas encore d'évaluation
- ORtHOGRAPHIC Plan FinalDocument8 pagesORtHOGRAPHIC Plan FinalKrizzie Jade CailingPas encore d'évaluation
- Big Game Guide: - Antelope - Bighorn Sheep - Deer - ElkDocument46 pagesBig Game Guide: - Antelope - Bighorn Sheep - Deer - ElkRoeHuntingResourcesPas encore d'évaluation
- Way of St. LouiseDocument18 pagesWay of St. LouiseMaryann GuevaradcPas encore d'évaluation
- Xi'an City Sports Park Landscape Improvement ProjectDocument3 pagesXi'an City Sports Park Landscape Improvement ProjectGirija Sankar SahuPas encore d'évaluation
- Biological Activity of Bone Morphogenetic ProteinsDocument4 pagesBiological Activity of Bone Morphogenetic Proteinsvanessa_werbickyPas encore d'évaluation
- Financial Fitness ChecklistDocument4 pagesFinancial Fitness Checklistcoach_22Pas encore d'évaluation
- Agricultural LocationDocument26 pagesAgricultural LocationPrince MpofuPas encore d'évaluation
- 3 - Accounting For Loans and ImpairmentDocument1 page3 - Accounting For Loans and ImpairmentReese AyessaPas encore d'évaluation
- Flex Li3 21 VAADocument1 pageFlex Li3 21 VAAAyman Al-YafeaiPas encore d'évaluation
- OsteomyelitisDocument10 pagesOsteomyelitismustafaPas encore d'évaluation
- Mca Lawsuit Details English From 2007 To Feb 2021Document2 pagesMca Lawsuit Details English From 2007 To Feb 2021api-463871923Pas encore d'évaluation
- Article ReviewDocument3 pagesArticle ReviewRAMADEVI A/P THANAGOPAL MoePas encore d'évaluation
- Introduction To Strategic Cost Management and Management AccountingDocument3 pagesIntroduction To Strategic Cost Management and Management AccountingnovyPas encore d'évaluation
- Cloud Native 5G Core Samsung 5G Core Volume 2Document16 pagesCloud Native 5G Core Samsung 5G Core Volume 2ALEXANDRE JOSE FIGUEIREDO LOUREIRO100% (1)
- Charging Station Location and Sizing For Electric Vehicles Under CongestionDocument20 pagesCharging Station Location and Sizing For Electric Vehicles Under CongestionJianli ShiPas encore d'évaluation
- New Microsoft Office Word DocumentDocument3 pagesNew Microsoft Office Word DocumentVince Vince100% (1)
- Resume Kantesh MundaragiDocument3 pagesResume Kantesh MundaragiKanteshPas encore d'évaluation