Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Holistic Approach in Glaucoma and Dry Eye: ONLINE WEBINAR - SATURDAY JUNE 26 2021 - 14:00 - 16:00 PM (WIB)Document1 pageHolistic Approach in Glaucoma and Dry Eye: ONLINE WEBINAR - SATURDAY JUNE 26 2021 - 14:00 - 16:00 PM (WIB)Dian Rahma RidwansyahPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Secondary GlaucomaDocument19 pagesSecondary GlaucomaRakhmad TriharsadiPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
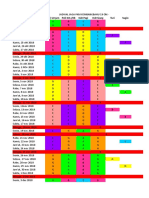
- Hari Tanggal Poli Umum Poli KIA /KB IGD Pagi IGD Siang Turi SugioDocument6 pagesHari Tanggal Poli Umum Poli KIA /KB IGD Pagi IGD Siang Turi SugioDian Rahma RidwansyahPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Bus Kartar Alisha TransDocument1 pageBus Kartar Alisha TransDian Rahma RidwansyahPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- PTSDDocument38 pagesPTSDDian Rahma RidwansyahPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Poster EWS & CB Malang Agustus 2018Document2 pagesPoster EWS & CB Malang Agustus 2018Dian Rahma RidwansyahPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Parasitic Disease (Pheumoystis Jirovecii Pheomonia)Document15 pagesParasitic Disease (Pheumoystis Jirovecii Pheomonia)Brijesh Singh YadavPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- KOMPLIKASIDocument3 pagesKOMPLIKASIDian Rahma RidwansyahPas encore d'évaluation
- InesshhgDocument13 pagesInesshhgDian Rahma RidwansyahPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Phacomorphic Glaucoma: Case and Review: Joseph Sowka, O.DDocument4 pagesPhacomorphic Glaucoma: Case and Review: Joseph Sowka, O.DDian Rahma RidwansyahPas encore d'évaluation
- Bacterial VaginosisDocument3 pagesBacterial VaginosisDian Rahma RidwansyahPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- IPA Assignment Analyzes New Public AdministrationDocument8 pagesIPA Assignment Analyzes New Public AdministrationKumaran ViswanathanPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- (Math 6 WK 5 L9) - Problems Involving Addition and or Subtraction of DecimalsDocument43 pages(Math 6 WK 5 L9) - Problems Involving Addition and or Subtraction of DecimalsRhea OcitePas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- A Sample of Directory or Instruction:: World Temperatures February 16Document1 pageA Sample of Directory or Instruction:: World Temperatures February 16eksaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Investigation of Twilight Using Sky Quality Meter For Isha' Prayer TimeDocument1 pageInvestigation of Twilight Using Sky Quality Meter For Isha' Prayer Timeresurgam52Pas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Sulzer MC EquipmentDocument12 pagesSulzer MC EquipmentsnthmlgtPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- DrdoDocument2 pagesDrdoAvneet SinghPas encore d'évaluation
- The Truth of Extinction: 7.1 Nietzsche's FableDocument2 pagesThe Truth of Extinction: 7.1 Nietzsche's FableGraciela Barón GuiñazúPas encore d'évaluation
- Designers' Guide To Eurocode 7 Geothechnical DesignDocument213 pagesDesigners' Guide To Eurocode 7 Geothechnical DesignJoão Gamboias100% (9)
- Manufacturing Processes (ME361) Lecture 13: Instructor: Shantanu BhattacharyaDocument28 pagesManufacturing Processes (ME361) Lecture 13: Instructor: Shantanu BhattacharyaSahil SundaPas encore d'évaluation
- CD1 ISO/IEC 17000 Conformity Assessment - Vocabulary and General PrinciplesDocument26 pagesCD1 ISO/IEC 17000 Conformity Assessment - Vocabulary and General PrinciplesMAC CONSULTORESPas encore d'évaluation
- Main Sulci & Fissures: Cerebral FissureDocument17 pagesMain Sulci & Fissures: Cerebral FissureNagbhushan BmPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- ECE Laws and Ethics NotesDocument29 pagesECE Laws and Ethics Notesmars100% (1)
- Reflecting on UPHSD's Mission, Vision, and Core ValuesDocument3 pagesReflecting on UPHSD's Mission, Vision, and Core ValuesBia N Cz100% (1)
- History of Computer AnimationDocument39 pagesHistory of Computer AnimationRanzelle UrsalPas encore d'évaluation
- 3.1-Pile Design Calculation For Boundary (p1 To p50)Document24 pages3.1-Pile Design Calculation For Boundary (p1 To p50)layaljamal2Pas encore d'évaluation
- Test Unit 7 m.2Document6 pagesTest Unit 7 m.2Petchara SridakunPas encore d'évaluation
- CROCI Focus Intellectual CapitalDocument35 pagesCROCI Focus Intellectual CapitalcarminatPas encore d'évaluation
- TM500 Design Overview (Complete ArchitectureDocument3 pagesTM500 Design Overview (Complete ArchitectureppghoshinPas encore d'évaluation
- Kuliah 1 - Konservasi GeologiDocument5 pagesKuliah 1 - Konservasi GeologiFerdianPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Inventory ManagementDocument60 pagesInventory Managementdrashti0% (1)
- Campbell Soup Case-StudyDocument3 pagesCampbell Soup Case-StudyraghudeepaPas encore d'évaluation
- Hackathon Statements V1Document10 pagesHackathon Statements V1AayushPas encore d'évaluation
- Proposed - TIA - 1392 - NFPA - 221Document2 pagesProposed - TIA - 1392 - NFPA - 221Junior TorrejónPas encore d'évaluation
- Penomoran Bantex - K64&COMPDocument8 pagesPenomoran Bantex - K64&COMPVigour Rizko MurdynePas encore d'évaluation
- CFLM1 Chapter 1Document24 pagesCFLM1 Chapter 1Jonathan TawagPas encore d'évaluation
- Exhaust Brake PDFDocument2 pagesExhaust Brake PDFFeliciaPas encore d'évaluation
- CA Module Franklin Gari RDocument28 pagesCA Module Franklin Gari RFranklin GariPas encore d'évaluation
- E Requisition SystemDocument8 pagesE Requisition SystemWaNi AbidPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Language Culture and ThoughtDocument24 pagesLanguage Culture and ThoughtLý Hiển NhiênPas encore d'évaluation
- Limits, Fits and Tolerances: Prof. S. S. PandeDocument31 pagesLimits, Fits and Tolerances: Prof. S. S. PandeM PankajPas encore d'évaluation