Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
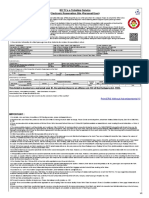
- Irctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Document2 pagesIrctcs E-Ticketing Service Electronic Reservation Slip (Personal User)RupKamalKutum100% (3)
- Managemnet Arterial UlcersDocument24 pagesManagemnet Arterial UlcersMohamad Zulfikar100% (1)
- The Back Book PDFDocument14 pagesThe Back Book PDFfoldsnholdsPas encore d'évaluation
- Irjet V5i9174Document7 pagesIrjet V5i9174madhujayarajPas encore d'évaluation
- B RoucheDocument3 pagesB RouchemadhujayarajPas encore d'évaluation
- FSSAI Regulations PDFDocument573 pagesFSSAI Regulations PDFkristokunsPas encore d'évaluation
- Contoh Proposal Bisnis PlanDocument31 pagesContoh Proposal Bisnis PlanHadianto Nugroho100% (4)
- 0 - RENTAL AGREEMENT YallapaDocument3 pages0 - RENTAL AGREEMENT YallapamadhujayarajPas encore d'évaluation
- Project TemplatesDocument66 pagesProject TemplatesfouzunPas encore d'évaluation
- Irctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Document3 pagesIrctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Akhilesh Kumar SinghPas encore d'évaluation
- Detail P&L Jan Feb Mar Apr May: To ControlDocument33 pagesDetail P&L Jan Feb Mar Apr May: To ControlmadhujayarajPas encore d'évaluation
- Irjet V5i9174Document7 pagesIrjet V5i9174madhujayarajPas encore d'évaluation
- Ever Green Bioenergy PVT LTDDocument9 pagesEver Green Bioenergy PVT LTDmadhujayarajPas encore d'évaluation
- Click To Edit Master Title StyleDocument5 pagesClick To Edit Master Title StyleNisa Widiya Wardani FaisalPas encore d'évaluation
- Projectto Dolist1Document2 pagesProjectto Dolist1madhujayarajPas encore d'évaluation
- Financial Model 1Document59 pagesFinancial Model 1madhujayarajPas encore d'évaluation
- Digestible Indispensable Amino Acid ScoreDocument1 pageDigestible Indispensable Amino Acid ScoremadhujayarajPas encore d'évaluation
- Windows 8 - Notice PDFDocument1 pageWindows 8 - Notice PDFSanthosh KumarPas encore d'évaluation
- Covid19 Govt Employee08092020Document4 pagesCovid19 Govt Employee08092020madhujayarajPas encore d'évaluation
- Agri 31Document1 pageAgri 31madhujayarajPas encore d'évaluation
- Rental Agreement - 1Document2 pagesRental Agreement - 1madhujayarajPas encore d'évaluation
- Mixing Tank: Recycled Algal Oil Dry Alcohol Storage Vegetable OilsDocument1 pageMixing Tank: Recycled Algal Oil Dry Alcohol Storage Vegetable OilsmadhujayarajPas encore d'évaluation
- Biobaja Cecair Multifungsisebagai Inputagronomiinovatif Untuk Pertanian ModenDocument4 pagesBiobaja Cecair Multifungsisebagai Inputagronomiinovatif Untuk Pertanian ModenmadhujayarajPas encore d'évaluation
- Dealership Application FormDocument2 pagesDealership Application FormmadhujayarajPas encore d'évaluation
- The National Cancer Institute Estimates That at Least 35Document1 pageThe National Cancer Institute Estimates That at Least 35madhujayarajPas encore d'évaluation
- Inventory Report 06-16-2019Document1 pageInventory Report 06-16-2019madhujayarajPas encore d'évaluation
- Animal SuP RIlDocument23 pagesAnimal SuP RIlmadhujayaraj100% (1)
- Innovative Integrated 3G Bio-Refineries: Presenter Name - Company NameDocument24 pagesInnovative Integrated 3G Bio-Refineries: Presenter Name - Company NamemadhujayarajPas encore d'évaluation
- Purchase Order 04Document2 pagesPurchase Order 04madhujayarajPas encore d'évaluation
- ReportDocument1 pageReportmadhujayarajPas encore d'évaluation
- Liquid-Liquid Extraction PrinciplesDocument34 pagesLiquid-Liquid Extraction PrinciplesAlonso D'AlburquePas encore d'évaluation
- Purchase Order 04Document1 pagePurchase Order 04madhujayarajPas encore d'évaluation
- VaginitisDocument16 pagesVaginitiserfPas encore d'évaluation
- Thesis Statement Examples Alzheimers DiseaseDocument6 pagesThesis Statement Examples Alzheimers DiseaseJulie Davis100% (2)
- Ampicillin Sodium - Sulbactam Sodium Drug StudyDocument1 pageAmpicillin Sodium - Sulbactam Sodium Drug StudyMelissa Marie Custodio100% (3)
- Oxford Handbook of Respiratory Nursing 2Nd Edition Terry Robinson Download PDF ChapterDocument51 pagesOxford Handbook of Respiratory Nursing 2Nd Edition Terry Robinson Download PDF Chapterpriscilla.villegas794100% (5)
- Renal Cell Carcinoma Tuberous SclerosisDocument48 pagesRenal Cell Carcinoma Tuberous SclerosisPiyushPas encore d'évaluation
- Scored Patient Generated Subjective Global Assessment PG SGA PDFDocument2 pagesScored Patient Generated Subjective Global Assessment PG SGA PDFOrlea Francisco-Sisio100% (1)
- TEN Mudras For Amazing Health BenefitsDocument3 pagesTEN Mudras For Amazing Health Benefitsrasikaa100% (3)
- Cerebral PalsyDocument96 pagesCerebral PalsyRahini PaniPas encore d'évaluation
- Approach To The Differential Diagnosis of Leg Ulcers - UpToDateDocument44 pagesApproach To The Differential Diagnosis of Leg Ulcers - UpToDatePriscillaPas encore d'évaluation
- Abdominal Pains in Children Under 12Document5 pagesAbdominal Pains in Children Under 12clubsanatatePas encore d'évaluation
- The Role of Educational Reform in Technology DevelopmentDocument6 pagesThe Role of Educational Reform in Technology DevelopmentpiaPas encore d'évaluation
- Classic Radiology SignsDocument9 pagesClassic Radiology SignsJui DirDapPas encore d'évaluation
- PADocument8 pagesPAtriziasisonPas encore d'évaluation
- Zang-Fu Syndrome Differentiation - UERMDocument113 pagesZang-Fu Syndrome Differentiation - UERMNathaniel P. Peralta0% (1)
- Cristian Zanartu, MD Joins New York Cancer & Blood SpecialistsDocument3 pagesCristian Zanartu, MD Joins New York Cancer & Blood SpecialistsPR.comPas encore d'évaluation
- Cor PulmonaleDocument13 pagesCor PulmonaleHayaPas encore d'évaluation
- Clinical Applications of Neuroimaging in PsychiatryDocument10 pagesClinical Applications of Neuroimaging in PsychiatryJujuPas encore d'évaluation
- Case Presentation On GbsDocument23 pagesCase Presentation On GbsRucHi ShArmaPas encore d'évaluation
- Oral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeDocument7 pagesOral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeSnowPas encore d'évaluation
- A Patient With Dry Mouth PDFDocument6 pagesA Patient With Dry Mouth PDFWahdatPas encore d'évaluation
- How To Paidalajin For Common Symptoms-Final VersionDocument35 pagesHow To Paidalajin For Common Symptoms-Final VersionAndy100% (2)
- Psychological Hardiness, Workplace Stress and Related Stress Reduction StrategiesDocument4 pagesPsychological Hardiness, Workplace Stress and Related Stress Reduction StrategiesAmir Parvez100% (2)
- MEDL The Integumentary SystemDocument37 pagesMEDL The Integumentary SystemEmil LacanilaoPas encore d'évaluation
- Causes of Cheyne-Stokes RespirationDocument9 pagesCauses of Cheyne-Stokes Respirationhlouis8Pas encore d'évaluation
- HB EstimationDocument15 pagesHB EstimationHaider AliPas encore d'évaluation
- Acute Bioligic CrisisDocument141 pagesAcute Bioligic CrisisJanelle MatamorosaPas encore d'évaluation
- تجميع المذكرات الاورثوDocument59 pagesتجميع المذكرات الاورثوMarah AbdulrahimPas encore d'évaluation
- Differential Diagnosis of CHDDocument42 pagesDifferential Diagnosis of CHDDr Piyush100% (1)