Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Foot reflexology chart shows how hand acupressure points relate to body partsDocument3 pagesFoot reflexology chart shows how hand acupressure points relate to body partsgautamlipika100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenPas encore d'évaluation
- Advanced Burn Life SupportDocument118 pagesAdvanced Burn Life SupportIntan Noa100% (1)
- Blood Bank ChecklistDocument4 pagesBlood Bank ChecklistFIAZ MAQBOOL FAZILIPas encore d'évaluation
- Guidelines For The Management of Severe Pre-Eclampsia (Anaes and Analgesia) 31.07.06Document5 pagesGuidelines For The Management of Severe Pre-Eclampsia (Anaes and Analgesia) 31.07.06grigmihPas encore d'évaluation
- How To Write A Clinical PaperDocument5 pagesHow To Write A Clinical PapergrigmihPas encore d'évaluation
- 1957213973Document173 pages1957213973grigmihPas encore d'évaluation
- HE2012 - Immunise Against HPVDocument6 pagesHE2012 - Immunise Against HPVgrigmihPas encore d'évaluation
- Dhillon 2022 How To Write A Good Scientific ReviDocument11 pagesDhillon 2022 How To Write A Good Scientific Revi邢振凯Pas encore d'évaluation
- General Best PracticeDocument193 pagesGeneral Best PracticegrigmihPas encore d'évaluation
- Global Routine Immunization Strategies and Practices: (Grisp)Document80 pagesGlobal Routine Immunization Strategies and Practices: (Grisp)Novita Dian PertiwiPas encore d'évaluation
- PIIS0748798322004966Document10 pagesPIIS0748798322004966grigmihPas encore d'évaluation
- Development and Novel Therapeutics in Hepatocellular Carcinoma A ReviewDocument11 pagesDevelopment and Novel Therapeutics in Hepatocellular Carcinoma A ReviewgrigmihPas encore d'évaluation
- 361 Full PDFDocument5 pages361 Full PDFgrigmihPas encore d'évaluation
- Guidelines For Obstetric Epidural Blood Patch NPS 5.4.06Document2 pagesGuidelines For Obstetric Epidural Blood Patch NPS 5.4.06grigmihPas encore d'évaluation
- Aasld 2018 HCCDocument28 pagesAasld 2018 HCCAzuzephre ClaraPas encore d'évaluation
- Multimodal Treatment of HCCDocument8 pagesMultimodal Treatment of HCCgrigmihPas encore d'évaluation
- Dual GraftDocument25 pagesDual GraftgrigmihPas encore d'évaluation
- BiomedJ382173-2563889 070718 PDFDocument4 pagesBiomedJ382173-2563889 070718 PDFgrigmihPas encore d'évaluation
- Thromboprophylaxis in Preg Following Vaginal CS Section 16-11-07Document9 pagesThromboprophylaxis in Preg Following Vaginal CS Section 16-11-07grigmihPas encore d'évaluation
- Nexavar GuideDocument8 pagesNexavar GuidegrigmihPas encore d'évaluation
- How To Practise Evidence-Based SurgeryDocument5 pagesHow To Practise Evidence-Based SurgerygrigmihPas encore d'évaluation
- Guide To Registration - 10 June 2009Document40 pagesGuide To Registration - 10 June 2009grigmihPas encore d'évaluation
- Influence of Hepatitis Viruses On Clinico-Pathological Profiles and Long-Term Outcome in Patients Undergoing Surgery For Hepatocellular CarcinomaDocument11 pagesInfluence of Hepatitis Viruses On Clinico-Pathological Profiles and Long-Term Outcome in Patients Undergoing Surgery For Hepatocellular CarcinomagrigmihPas encore d'évaluation
- Ha Tace For MMLM 2008Document6 pagesHa Tace For MMLM 2008grigmihPas encore d'évaluation
- Staging HCCDocument5 pagesStaging HCCgrigmihPas encore d'évaluation
- Gpc3 Generate de Celule Dendritice 2010Document11 pagesGpc3 Generate de Celule Dendritice 2010grigmihPas encore d'évaluation
- Nursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDocument5 pagesNursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDr-Marudhar MarudharPas encore d'évaluation
- Ir Medical 2017 A3 PDFDocument25 pagesIr Medical 2017 A3 PDFHeidi BluePas encore d'évaluation
- Elevated BilirubinDocument5 pagesElevated BilirubinNovita ApramadhaPas encore d'évaluation
- Hypertension in PregnancyDocument18 pagesHypertension in Pregnancyshubham kumarPas encore d'évaluation
- Periapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesDocument9 pagesPeriapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesFlorin Ionescu100% (1)
- rút gọnDocument3 pagesrút gọnUyen VuPas encore d'évaluation
- Kasus Farter 2 10 Mei 2019Document3 pagesKasus Farter 2 10 Mei 2019YonicaryanPas encore d'évaluation
- Bronchopulmonary Dysplasia (BPD)Document13 pagesBronchopulmonary Dysplasia (BPD)Joan BuiPas encore d'évaluation
- Abnormal PuerperiumDocument65 pagesAbnormal PuerperiumNigus AfessaPas encore d'évaluation
- Artikel IlmiahDocument12 pagesArtikel IlmiahAsti NurchasanahPas encore d'évaluation
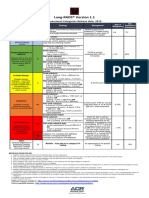
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotPas encore d'évaluation
- Definition:: Between 16Document3 pagesDefinition:: Between 16NIDA MUSTAFAPas encore d'évaluation
- Adult Hippocampal NeurogenesisDocument14 pagesAdult Hippocampal NeurogenesisElaine HermansPas encore d'évaluation
- Femoral Acetabular Impingement: RadiographyDocument9 pagesFemoral Acetabular Impingement: Radiography杨钦杰Pas encore d'évaluation
- CNA Chapter 1 & 2 TermsDocument1 pageCNA Chapter 1 & 2 TermsMarina ChakarPas encore d'évaluation
- Basic pharmacology of anaesthesia drugs in 40 charactersDocument56 pagesBasic pharmacology of anaesthesia drugs in 40 charactersrajvikram87Pas encore d'évaluation
- Aula 1Document14 pagesAula 1Brigida Cirqueira GuimaraesPas encore d'évaluation
- HematologyDocument100 pagesHematologyerzaraptorPas encore d'évaluation
- Ann JeinaDocument7 pagesAnn JeinaMizumoriFumairaPas encore d'évaluation
- It 18 - Neonatal Seizure - HerDocument35 pagesIt 18 - Neonatal Seizure - HerRurie Awalia SuhardiPas encore d'évaluation
- Acute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsDocument2 pagesAcute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsSachin SinghPas encore d'évaluation
- Type2 Diabetes HandoutDocument1 pageType2 Diabetes Handouthendra_darmawan_4Pas encore d'évaluation
- Choose 2 From The Disease Below That Are Emerging in The PhilippinesDocument4 pagesChoose 2 From The Disease Below That Are Emerging in The PhilippinesMICHELLE BIANCA PATRICE CRUZPas encore d'évaluation
- Case Report模板Document18 pagesCase Report模板ChenPas encore d'évaluation
- Kali Bichromicum 30C For COPD 2005Document8 pagesKali Bichromicum 30C For COPD 2005Dr. Nancy MalikPas encore d'évaluation
- Corneal Dystrophies: Causes, Symptoms, and TreatmentDocument2 pagesCorneal Dystrophies: Causes, Symptoms, and TreatmentBadgal BazingaPas encore d'évaluation