Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- 03 - ICD-10-CM Proficiency Assessment WorkbookDocument117 pages03 - ICD-10-CM Proficiency Assessment Workbookprabhujaya97893100% (4)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Polycythemia Vera ReportDocument31 pagesPolycythemia Vera ReportAdrianPas encore d'évaluation
- Approach To Unknown Drug OverdoseDocument3 pagesApproach To Unknown Drug OverdoseRobert So JrPas encore d'évaluation
- HISTORY AND PHYSICAL EXAMINATION (Putul)Document2 pagesHISTORY AND PHYSICAL EXAMINATION (Putul)Reshma Francis100% (1)
- Periodontology MCQDocument103 pagesPeriodontology MCQMohamad SaidPas encore d'évaluation
- Peritoneal DialysisDocument56 pagesPeritoneal DialysisVanet100% (1)
- Facial Expressions of Pain in CatsDocument11 pagesFacial Expressions of Pain in CatsJohan SalazarPas encore d'évaluation
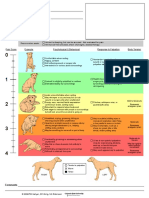
- Universidad Estadual de Colorado - Acute - Pain - Scale - Canine PDFDocument1 pageUniversidad Estadual de Colorado - Acute - Pain - Scale - Canine PDFJohan SalazarPas encore d'évaluation
- Atkins Et Al-Journal of Veterinary Internal Medicine PDFDocument9 pagesAtkins Et Al-Journal of Veterinary Internal Medicine PDFizabel bordinPas encore d'évaluation
- Root Kust Ritz 2003Document47 pagesRoot Kust Ritz 2003Celene La CruzPas encore d'évaluation
- Fri May 23rd 2014 Blog PostDocument3 pagesFri May 23rd 2014 Blog PostCelene La CruzPas encore d'évaluation
- La 09015Document5 pagesLa 09015Celene La CruzPas encore d'évaluation
- Philippine CPG On The Diagnosis and Management of Urinary Tract Infections in Adults-2015 Update - Part 2 PDFDocument140 pagesPhilippine CPG On The Diagnosis and Management of Urinary Tract Infections in Adults-2015 Update - Part 2 PDFspringdingPas encore d'évaluation
- Alzheimer Disease EngDocument35 pagesAlzheimer Disease EngAna IantucPas encore d'évaluation
- Chestpain 150320061131 Conversion Gate01Document36 pagesChestpain 150320061131 Conversion Gate01Aisha AldosreyPas encore d'évaluation
- Types of Stroke: Stroke - CVA Cerebral Vascular Accident Ischemic Cerebrovascular DiseaseDocument7 pagesTypes of Stroke: Stroke - CVA Cerebral Vascular Accident Ischemic Cerebrovascular DiseaseMarrylane GamisPas encore d'évaluation
- Eop Paediatric Posting C 2017Document3 pagesEop Paediatric Posting C 2017ayunisallehPas encore d'évaluation
- Monitoring key dermatologic medicationsDocument3 pagesMonitoring key dermatologic medicationsriskhakovPas encore d'évaluation
- Assessment Report On Ginkgo Biloba L., Folium DDocument120 pagesAssessment Report On Ginkgo Biloba L., Folium DMiroslav IlicPas encore d'évaluation
- Oral Manifestations ShareDocument38 pagesOral Manifestations SharePrachi ChaturvediPas encore d'évaluation
- Differential DiagnosisDocument14 pagesDifferential DiagnosisnurulPas encore d'évaluation
- PH20-000531 SDV Pneumococcal 13-Valent Conjugate Vaccine Prevenar 13 VialDocument39 pagesPH20-000531 SDV Pneumococcal 13-Valent Conjugate Vaccine Prevenar 13 VialLoanne RamiterrePas encore d'évaluation
- Lectura Previa3-Approach To The Patient With Abnormal Vital SignsDocument7 pagesLectura Previa3-Approach To The Patient With Abnormal Vital SignsEdwin Robles NorabuenaPas encore d'évaluation
- Rheumatology NotesDocument10 pagesRheumatology NotesBrandonRyanF.MosidinPas encore d'évaluation
- Laryngitis and PericarditisDocument17 pagesLaryngitis and Pericarditis2B-4- TUNAC, Avvy Charlotte R.Pas encore d'évaluation
- Medical CertificateDocument2 pagesMedical CertificatelekacaPas encore d'évaluation
- Acute Inflammatory Demyelinating PolyneuropathyDocument55 pagesAcute Inflammatory Demyelinating PolyneuropathyImmanuel100% (1)
- Anticholinergic Drugs,: Ganglion Blocking Agents and Neuromuscular Blocking AgentsDocument26 pagesAnticholinergic Drugs,: Ganglion Blocking Agents and Neuromuscular Blocking AgentsLoai Mohammed IssaPas encore d'évaluation
- Articulo Clase Miercoles 2Document15 pagesArticulo Clase Miercoles 2franciscoPas encore d'évaluation
- Graves' Disease OverviewDocument1 pageGraves' Disease OverviewMichael PutraPas encore d'évaluation
- Recent Advances in NGF and Related Molecules: Laura Calzà Luigi Aloe Luciana Giardino EditorsDocument302 pagesRecent Advances in NGF and Related Molecules: Laura Calzà Luigi Aloe Luciana Giardino EditorsPedro CastroPas encore d'évaluation
- Acquired Hypopigmentation Disorders Other Than Vitiligo - UpToDateDocument23 pagesAcquired Hypopigmentation Disorders Other Than Vitiligo - UpToDateBhargav YagnikPas encore d'évaluation
- EKG Interpretation: DR K P Tripathy Kims, BhubaneswarDocument58 pagesEKG Interpretation: DR K P Tripathy Kims, BhubaneswarAbhilash MohantyPas encore d'évaluation
- Kompilasi - ICD MM Dan PM - Reference GuideDocument93 pagesKompilasi - ICD MM Dan PM - Reference GuidehijraPas encore d'évaluation
- ESUR Guidelines 10.0 Final VersionDocument46 pagesESUR Guidelines 10.0 Final Versionkon shirePas encore d'évaluation
- FMGE March 2008 MCQs Hello Everyone, If The Results AreDocument15 pagesFMGE March 2008 MCQs Hello Everyone, If The Results Arearslansaeed007Pas encore d'évaluation