Vous aimerez peut-être aussi
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- NCLEX Random FactsDocument34 pagesNCLEX Random FactsLegnaMary100% (8)
- Oop Say You Know MeDocument1 pageOop Say You Know MeawuahbohPas encore d'évaluation
- The BSN Job Search: Interview Preparation: Telling Your StoryDocument25 pagesThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohPas encore d'évaluation
- King Rush MoreDocument1 pageKing Rush MoreawuahbohPas encore d'évaluation
- Article For JournalDocument6 pagesArticle For JournalawuahbohPas encore d'évaluation
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Document23 pagesMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohPas encore d'évaluation
- HandOff SampleToolsDocument9 pagesHandOff SampleToolsOllie EvansPas encore d'évaluation
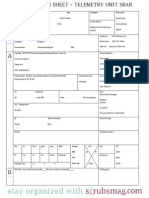
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624Pas encore d'évaluation
- Pharm NclexDocument9 pagesPharm NclexawuahbohPas encore d'évaluation
- Drugs NclexDocument30 pagesDrugs Nclexawuahboh100% (1)
- Probability of A or B and A and B-1Document2 pagesProbability of A or B and A and B-1awuahbohPas encore d'évaluation
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohPas encore d'évaluation
- PolypharmacyDocument24 pagesPolypharmacySurina Zaman HuriPas encore d'évaluation
- Massachusetts Department of Public HealthDocument24 pagesMassachusetts Department of Public HealthawuahbohPas encore d'évaluation
- Random FactsDocument338 pagesRandom Factscyram81100% (1)
- EBP Article 1Document11 pagesEBP Article 1awuahbohPas encore d'évaluation
- EBP Article 3Document6 pagesEBP Article 3awuahbohPas encore d'évaluation
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohPas encore d'évaluation
- Tips On Answering NclexDocument4 pagesTips On Answering NclexawuahbohPas encore d'évaluation
- ENT Throat and EsophagusDocument41 pagesENT Throat and EsophagusMUHAMMAD HASAN NAGRAPas encore d'évaluation
- Therapeutic CommunicationDocument1 pageTherapeutic CommunicationawuahbohPas encore d'évaluation
- Critical Thinking StrategiesDocument3 pagesCritical Thinking StrategiesawuahbohPas encore d'évaluation
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDocument24 pagesDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohPas encore d'évaluation
- STDA VaricealDocument8 pagesSTDA VaricealDeisy de JesusPas encore d'évaluation
- Debate 3 Youth Incarceration in Adult PrisonsDocument6 pagesDebate 3 Youth Incarceration in Adult PrisonsawuahbohPas encore d'évaluation
- Patient Report FormDocument1 pagePatient Report FormawuahbohPas encore d'évaluation
- Parkland formula and rule of 9Document8 pagesParkland formula and rule of 9awuahbohPas encore d'évaluation
- Article For Journal 4-18-14Document8 pagesArticle For Journal 4-18-14awuahbohPas encore d'évaluation
- Article For Jouranal 2 (498P)Document5 pagesArticle For Jouranal 2 (498P)awuahbohPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Enabling Keycloak Metrics - KeycloakDocument3 pagesEnabling Keycloak Metrics - Keycloakhisyam darwisPas encore d'évaluation
- MN00119 Unicom LT User ManualDocument45 pagesMN00119 Unicom LT User ManualPhilipp A IslaPas encore d'évaluation
- 3.0 Wrap Up and SummaryDocument4 pages3.0 Wrap Up and SummaryGian SanchezPas encore d'évaluation
- Finimpianti Power EngDocument2 pagesFinimpianti Power EngJosip GrlicaPas encore d'évaluation
- Writing Emails Part 1 Informal British English Teacher Ver2Document7 pagesWriting Emails Part 1 Informal British English Teacher Ver2Madalina MandiucPas encore d'évaluation
- MDS Report Substances of Assemblies and Materials: 1. Company and Product NameDocument17 pagesMDS Report Substances of Assemblies and Materials: 1. Company and Product Namejavier ortizPas encore d'évaluation
- Cartoon Network, Boomerang & TCM TV Rate Card July - SeptemberDocument11 pagesCartoon Network, Boomerang & TCM TV Rate Card July - SeptemberR RizalPas encore d'évaluation
- Food Conformity BA 550-13Document9 pagesFood Conformity BA 550-13puipuiesperaPas encore d'évaluation
- Toolbox Meeting Or, TBT (Toolbox TalkDocument10 pagesToolbox Meeting Or, TBT (Toolbox TalkHarold PoncePas encore d'évaluation
- Formulating and Solving LPs Using Excel SolverDocument8 pagesFormulating and Solving LPs Using Excel SolverAaron MartinPas encore d'évaluation
- Mental AspectDocument29 pagesMental AspectBenjii CarlosPas encore d'évaluation
- Innovations in Drill Stem Safety Valve TechnologyDocument22 pagesInnovations in Drill Stem Safety Valve Technologymiguel mendoza0% (1)
- Attitudes and Practices Related To Sexuality and Sexual BehaviorDocument35 pagesAttitudes and Practices Related To Sexuality and Sexual BehaviorGalvin LalusinPas encore d'évaluation
- Texas Final LeadsDocument36 pagesTexas Final Leadsabdullahmohammed4460Pas encore d'évaluation
- Query Operation 2021Document35 pagesQuery Operation 2021Abdo AbaborPas encore d'évaluation
- IIT BOMBAY RESUME by SathyamoorthyDocument1 pageIIT BOMBAY RESUME by SathyamoorthySathyamoorthy VenkateshPas encore d'évaluation
- Efficacy of Platelet-Rich Fibrin On Socket Healing After Mandibular Third Molar ExtractionsDocument10 pagesEfficacy of Platelet-Rich Fibrin On Socket Healing After Mandibular Third Molar Extractionsxiaoxin zhangPas encore d'évaluation
- Statistics Interview QuestionsDocument5 pagesStatistics Interview QuestionsARCHANA R100% (1)
- 1729Document52 pages1729praj24083302Pas encore d'évaluation
- DodupukegakobemavasevuDocument3 pagesDodupukegakobemavasevuMartian SamaanPas encore d'évaluation
- Proposal BP3IP FinalDocument3 pagesProposal BP3IP FinalGiant SeptiantoPas encore d'évaluation
- Frame Fit Specs SramDocument22 pagesFrame Fit Specs SramJanekPas encore d'évaluation
- American With Disabilities Act AdaDocument16 pagesAmerican With Disabilities Act Adaapi-376186426Pas encore d'évaluation
- CP QB PT-3 Harish KumarDocument3 pagesCP QB PT-3 Harish KumarVISHNU7 77Pas encore d'évaluation
- Zeal Institute of Manangement and Computer ApplicationDocument4 pagesZeal Institute of Manangement and Computer ApplicationSONAL UTTARKARPas encore d'évaluation
- CM Group Marketing To Gen Z ReportDocument20 pagesCM Group Marketing To Gen Z Reportroni21Pas encore d'évaluation
- A Study To Assess The Effectiveness of PDocument9 pagesA Study To Assess The Effectiveness of PKamal JindalPas encore d'évaluation
- Grupo Stoncor Description - Stonhard Carboline Fibergrate PDFDocument22 pagesGrupo Stoncor Description - Stonhard Carboline Fibergrate PDFAndres OsorioPas encore d'évaluation
- Formal Analysis of Timeliness in Electronic Commerce ProtocolsDocument5 pagesFormal Analysis of Timeliness in Electronic Commerce Protocolsjuan david arteagaPas encore d'évaluation
- 3ADW000379R0301 DCS550 Manual e CDocument310 pages3ADW000379R0301 DCS550 Manual e CLaura SelvaPas encore d'évaluation