Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Oop Say You Know MeDocument1 pageOop Say You Know MeawuahbohPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Article For JournalDocument6 pagesArticle For JournalawuahbohPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- NCLEX Random FactsDocument34 pagesNCLEX Random FactsLegnaMary100% (8)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
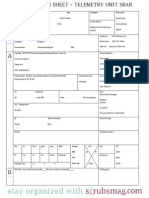
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624Pas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The BSN Job Search: Interview Preparation: Telling Your StoryDocument25 pagesThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- King Rush MoreDocument1 pageKing Rush MoreawuahbohPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- HandOff SampleToolsDocument9 pagesHandOff SampleToolsOllie EvansPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Pharm NclexDocument9 pagesPharm NclexawuahbohPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Massachusetts Department of Public HealthDocument24 pagesMassachusetts Department of Public HealthawuahbohPas encore d'évaluation
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Document23 pagesMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- PolypharmacyDocument24 pagesPolypharmacySurina Zaman HuriPas encore d'évaluation
- Probability of A or B and A and B-1Document2 pagesProbability of A or B and A and B-1awuahbohPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Random FactsDocument338 pagesRandom Factscyram81100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- ENT Throat and EsophagusDocument41 pagesENT Throat and EsophagusMUHAMMAD HASAN NAGRAPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- EBP Article 1Document11 pagesEBP Article 1awuahbohPas encore d'évaluation
- Drugs NclexDocument30 pagesDrugs Nclexawuahboh100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Tips On Answering NclexDocument4 pagesTips On Answering NclexawuahbohPas encore d'évaluation
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDocument24 pagesDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohPas encore d'évaluation
- EBP Article 3Document6 pagesEBP Article 3awuahbohPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Critical Thinking StrategiesDocument3 pagesCritical Thinking StrategiesawuahbohPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- STDA VaricealDocument8 pagesSTDA VaricealDeisy de JesusPas encore d'évaluation
- Therapeutic CommunicationDocument1 pageTherapeutic CommunicationawuahbohPas encore d'évaluation
- Patient Report FormDocument1 pagePatient Report FormawuahbohPas encore d'évaluation
- Med Surg BurnsDocument8 pagesMed Surg BurnsawuahbohPas encore d'évaluation
- Article For JournalDocument6 pagesArticle For JournalawuahbohPas encore d'évaluation
- Debate 3 Youth Incarceration in Adult PrisonsDocument6 pagesDebate 3 Youth Incarceration in Adult PrisonsawuahbohPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohPas encore d'évaluation
- Article For Jouranal 2 (498P)Document5 pagesArticle For Jouranal 2 (498P)awuahbohPas encore d'évaluation
- CP 4Document79 pagesCP 4Kalichandren ArumugamPas encore d'évaluation
- Oral Rehydration SaltDocument3 pagesOral Rehydration SaltVincent ManganaanPas encore d'évaluation
- Tanzania Stgs EmlDocument220 pagesTanzania Stgs EmlHervis Francisco FantiniPas encore d'évaluation
- Frequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaDocument4 pagesFrequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaRaja Bajak LautPas encore d'évaluation
- Nursing Exam For Review With RationaleDocument39 pagesNursing Exam For Review With RationaleKeizha Ronatay100% (2)
- DIARRHOEAL DISEASES FinalDocument86 pagesDIARRHOEAL DISEASES FinalBinaya100% (1)
- Dehydration in ChildrenDocument24 pagesDehydration in ChildrenDani AsmarePas encore d'évaluation
- Acute Diarrhea in Adults and Children A Global PerspectiveDocument10 pagesAcute Diarrhea in Adults and Children A Global PerspectiverobyPas encore d'évaluation
- Treatment of DiarrheaDocument6 pagesTreatment of DiarrheaVictor TayoPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Food Based Oral Rehydration Therapy Towards A Better Choleratreatment 2329 8901 1000151Document3 pagesFood Based Oral Rehydration Therapy Towards A Better Choleratreatment 2329 8901 1000151Michael HusainPas encore d'évaluation
- Acute Viral Gastroenteritis in Children in Resource-Rich Countries: Management and PreventionDocument25 pagesAcute Viral Gastroenteritis in Children in Resource-Rich Countries: Management and Preventiondaniso12Pas encore d'évaluation
- Icrc NutrationDocument712 pagesIcrc NutrationSamar Saad100% (1)
- Roosterman 26Document36 pagesRoosterman 26Huey VillanuevaPas encore d'évaluation
- Management of The Short Bowel Syndrome in Adults - UpToDateDocument10 pagesManagement of The Short Bowel Syndrome in Adults - UpToDateyessyPas encore d'évaluation
- DehydrationDocument14 pagesDehydrationReimer LaquihuanacoPas encore d'évaluation
- American Journal of Gastroenterology Volume 104 Issue 10 2009 (Doi 10.1038/ajg.2009.329) Atia, Antwan N Buchman, Alan L - Oral Rehydration Solutions in Non-Cholera Diarrhea - A ReviewDocument9 pagesAmerican Journal of Gastroenterology Volume 104 Issue 10 2009 (Doi 10.1038/ajg.2009.329) Atia, Antwan N Buchman, Alan L - Oral Rehydration Solutions in Non-Cholera Diarrhea - A ReviewFadhil AbdillahPas encore d'évaluation
- Fluids and Electrolytes: Department of Family & Community MedicineDocument40 pagesFluids and Electrolytes: Department of Family & Community MedicineNoornihuma AsharPas encore d'évaluation
- Food PoisoningDocument24 pagesFood PoisoningSena AjahPas encore d'évaluation
- World Health Organization: WHO/CDD/SER/91.15 REV.1Document10 pagesWorld Health Organization: WHO/CDD/SER/91.15 REV.1IjafiyaPas encore d'évaluation
- Acute GastroenteritisDocument11 pagesAcute GastroenteritisIneke PutriPas encore d'évaluation
- Fluid and Electrolytes JoyDocument10 pagesFluid and Electrolytes JoyM Rizal IsburhanPas encore d'évaluation
- Six Pack GuideDocument49 pagesSix Pack GuideGeet_DPas encore d'évaluation
- Maple Syrup Urine Disease (MSUD)Document28 pagesMaple Syrup Urine Disease (MSUD)Dr. Mohammed Al Ja’fari, MDPas encore d'évaluation
- Fall Cleanse GuideDocument58 pagesFall Cleanse GuideMarifé Cepeda CastroPas encore d'évaluation
- An Overview of Management of Dehydration in Paediatric Age GroupDocument3 pagesAn Overview of Management of Dehydration in Paediatric Age Grouppriyanka2Pas encore d'évaluation
- Fluids and Electrolytes in Pediatrics FinalDocument41 pagesFluids and Electrolytes in Pediatrics FinalArun GeorgePas encore d'évaluation
- Paediatric Diarrhoea - Lee Way SeahDocument42 pagesPaediatric Diarrhoea - Lee Way SeahayunisallehPas encore d'évaluation
- Unit-6 New Born IgnouDocument26 pagesUnit-6 New Born IgnouVijay MgPas encore d'évaluation
- Esnm12 Acute Diarrhoea in Children Racecadotril As An Adjunct To Oral Rehydration Esnm12Document16 pagesEsnm12 Acute Diarrhoea in Children Racecadotril As An Adjunct To Oral Rehydration Esnm12Rom IrPas encore d'évaluation
- Whooping CoughDocument72 pagesWhooping Coughwengie100% (1)