Vous aimerez peut-être aussi
- General Surgery SMALL INTESTINES-Dr MendozaDocument101 pagesGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101Pas encore d'évaluation
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocument11 pagesClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388Pas encore d'évaluation
- Visayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieDocument43 pagesVisayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieJanseen EdizaPas encore d'évaluation
- 1100 Ultrasound of The Acute Abdomen 15 3Document84 pages1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016Pas encore d'évaluation
- Based on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDocument37 pagesBased on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDanielle FosterPas encore d'évaluation
- Examination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaDocument29 pagesExamination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaForeighn97Pas encore d'évaluation
- Colonic and Small Intestine Disorders-1Document28 pagesColonic and Small Intestine Disorders-1YIKI ISAACPas encore d'évaluation
- The Stomach and Duodenum: Dr. Elian EliasDocument48 pagesThe Stomach and Duodenum: Dr. Elian EliasmodarPas encore d'évaluation
- Pemicu 5Document75 pagesPemicu 5Cantika Monica LonanPas encore d'évaluation
- Dr. H. Achmad Fuadi, SPB-KBD, MkesDocument47 pagesDr. H. Achmad Fuadi, SPB-KBD, MkesytreiiaaPas encore d'évaluation
- Instestinal Obstruction UbthDocument34 pagesInstestinal Obstruction UbthDonald IDEDEPas encore d'évaluation
- VolvulusDocument38 pagesVolvulusHector RaulPas encore d'évaluation
- K11 Bedah EsofagusDocument37 pagesK11 Bedah EsofagusenriPas encore d'évaluation
- SURG - Hepatobiliary, Pancreas, SpleenDocument230 pagesSURG - Hepatobiliary, Pancreas, SpleenJoan Timbol100% (1)
- Large Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005Document22 pagesLarge Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005samsabesPas encore d'évaluation
- Ulcerative ColitisDocument63 pagesUlcerative ColitismahalakshmiPas encore d'évaluation
- 3.radiation InjDocument9 pages3.radiation Injapi-3829364Pas encore d'évaluation
- Small Intestine: Earle J. Niervo Medical ClerkDocument168 pagesSmall Intestine: Earle J. Niervo Medical ClerkEarle Jimenez Niervo RNPas encore d'évaluation
- Intestinal Obstruction: by Dr. Shereen Abd El-MoniemDocument44 pagesIntestinal Obstruction: by Dr. Shereen Abd El-MoniemフセインPas encore d'évaluation
- Screenshot 2023-11-26 at 5.15.31 PMDocument39 pagesScreenshot 2023-11-26 at 5.15.31 PMgauravsingh708284Pas encore d'évaluation
- DiverticulosisDocument9 pagesDiverticulosisSyafiq Shahbudin100% (1)
- Small & Large Intestines - LectureDocument70 pagesSmall & Large Intestines - Lecturehussain AltaherPas encore d'évaluation
- Colilithiasis 2Document53 pagesColilithiasis 2Worku KiflePas encore d'évaluation
- Small Bowel: Alaa MaaliDocument78 pagesSmall Bowel: Alaa MaaliHalima AssiPas encore d'évaluation
- Intestinal ObstructionDocument19 pagesIntestinal ObstructionAna-Maria OchialbiPas encore d'évaluation
- Acute Calculous CholecystitisDocument25 pagesAcute Calculous CholecystitisShankar LamichhanePas encore d'évaluation
- ABDOMINAL PAIN AFTER CHOLECYSTECTOMYDocument77 pagesABDOMINAL PAIN AFTER CHOLECYSTECTOMYShermin ShakilPas encore d'évaluation
- Disorders of Small IntestineDocument41 pagesDisorders of Small IntestineSamuel kuriaPas encore d'évaluation
- Acute Intestinal Obstruction...Document42 pagesAcute Intestinal Obstruction...Ali100% (2)
- The Digestive System: and ItsDocument102 pagesThe Digestive System: and ItsRhea Andrea Uy100% (1)
- Surgical AbdomenDocument3 pagesSurgical Abdomendude dPas encore d'évaluation
- Large Bowel Obstruction by Nic MDocument42 pagesLarge Bowel Obstruction by Nic MRisky OpponentPas encore d'évaluation
- Causes, Symptoms and Treatment of Intestinal ObstructionDocument15 pagesCauses, Symptoms and Treatment of Intestinal ObstructionEmmeline Dycangchon-GarmaPas encore d'évaluation
- Nursing Stomach NotesDocument5 pagesNursing Stomach Noteslucas dibenedettoPas encore d'évaluation
- Longcase Surgery ListDocument11 pagesLongcase Surgery ListDiyana ZatyPas encore d'évaluation
- Diverticular Disease: Etiology, Pathophysiology and ManagementDocument67 pagesDiverticular Disease: Etiology, Pathophysiology and Managementunknownsince1986Pas encore d'évaluation
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenPas encore d'évaluation
- Inflammatory Bowel Disease: Younes R YounesDocument38 pagesInflammatory Bowel Disease: Younes R YounesDarawan MirzaPas encore d'évaluation
- K-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUDocument38 pagesK-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUChristian Lumban GaolPas encore d'évaluation
- Appendicitis 5.9Document50 pagesAppendicitis 5.9Smart SaravanaPas encore d'évaluation
- Acute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Document63 pagesAcute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Rumana IslamPas encore d'évaluation
- Gastro NephroDocument93 pagesGastro Nephrohasanatiya41Pas encore d'évaluation
- Colon: Malueth AbrahamDocument39 pagesColon: Malueth AbrahamMalueth AnguiPas encore d'évaluation
- ConstipationDocument33 pagesConstipationsalmawalidPas encore d'évaluation
- Chronic DiarrheaDocument66 pagesChronic DiarrheaJulita Yanti100% (1)
- Intestinal Diseases in Cattle 2023Document30 pagesIntestinal Diseases in Cattle 2023Krystyna WędrychowskaPas encore d'évaluation
- Bowel ObstructionDocument10 pagesBowel Obstructionenke.nwekePas encore d'évaluation
- Acute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenDocument25 pagesAcute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenLuqman Arif Ahmad HazriPas encore d'évaluation
- Intestinal Obstruction GuideDocument80 pagesIntestinal Obstruction GuideAbhirami AnilPas encore d'évaluation
- Benign Colorectal Disease: Ahmed AlzahraniDocument47 pagesBenign Colorectal Disease: Ahmed Alzahraniahmad alzahraniPas encore d'évaluation
- Intestinal Obstruction: Methas Arunnart MDDocument42 pagesIntestinal Obstruction: Methas Arunnart MDJhe-sie AngelinaPas encore d'évaluation
- Acute Cholecystitis:: Etiological TypesDocument5 pagesAcute Cholecystitis:: Etiological Typesvivek yadavPas encore d'évaluation
- PANCREASDocument74 pagesPANCREASzaiba0786Pas encore d'évaluation
- Chronic Bowel Disease and SepsisDocument52 pagesChronic Bowel Disease and SepsisOlga Goryacheva100% (1)
- Intestinal Obstruction PDFDocument7 pagesIntestinal Obstruction PDFmist73Pas encore d'évaluation
- The PancreasDocument37 pagesThe PancreasFaiza AshrafPas encore d'évaluation
- Problem 4 GITDocument94 pagesProblem 4 GITArioPas encore d'évaluation
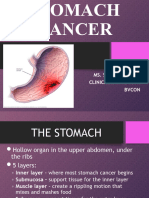
- Stomach CancerDocument36 pagesStomach CancerSonali DakhorePas encore d'évaluation
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsÉvaluation : 5 sur 5 étoiles5/5 (1)
- A&P Coloring Workbook - The Endocrine System PDFDocument12 pagesA&P Coloring Workbook - The Endocrine System PDFAnonymous WwJAxdz100% (4)
- OSU Admissions Publications - Oklahoma State UniversityDocument3 pagesOSU Admissions Publications - Oklahoma State UniversityaaaPas encore d'évaluation
- Reading Test Text A Corona Virus Disease 19 - A Brief NoteDocument23 pagesReading Test Text A Corona Virus Disease 19 - A Brief Notedevaki dangalPas encore d'évaluation
- LiposarcomaDocument9 pagesLiposarcomaKenneth ColePas encore d'évaluation
- IPHO Accomplishment Report For May 2018Document12 pagesIPHO Accomplishment Report For May 2018ebc07Pas encore d'évaluation
- Case Study On LEUKEMIADocument55 pagesCase Study On LEUKEMIAmacky90% (21)
- PSAE review-AWMS PDFDocument37 pagesPSAE review-AWMS PDFCynthia B.GayumbaPas encore d'évaluation
- ESICM EDIC Part I exam guideDocument6 pagesESICM EDIC Part I exam guideErlan SantosPas encore d'évaluation
- Atrophic GlossitisDocument7 pagesAtrophic Glossitisbima prabuPas encore d'évaluation
- Artifical Feeding Summary SheetDocument3 pagesArtifical Feeding Summary SheetCyrelle Jen TorresPas encore d'évaluation
- Thesis On Food AdulterationDocument4 pagesThesis On Food Adulterationkatieparkersaintpaul100% (1)
- Top 10 Tips Flyer 8.5x11-English 10-18Document1 pageTop 10 Tips Flyer 8.5x11-English 10-18Maren JensenPas encore d'évaluation
- RPB Astro Instruction ManualDocument20 pagesRPB Astro Instruction ManualJayvee Baradas ValdezPas encore d'évaluation
- National Transportation Strategy: Kingdom of Saudi Arabia Ministry of TransportDocument100 pagesNational Transportation Strategy: Kingdom of Saudi Arabia Ministry of Transportvprajan82Pas encore d'évaluation
- Outlining the Differences Between the Medical and Social Models of DisabilityDocument8 pagesOutlining the Differences Between the Medical and Social Models of DisabilityJon CollagePas encore d'évaluation
- Anti Parkinson Disease - PDF - Pharmacology - AssignmentDocument11 pagesAnti Parkinson Disease - PDF - Pharmacology - AssignmentMr HotmasterPas encore d'évaluation
- Pertanggungjawaban Hukum Praktik Tukang Gigi Yang Melebihi Wewenangnya Devi Dharmawan, Ivonne JonathanDocument9 pagesPertanggungjawaban Hukum Praktik Tukang Gigi Yang Melebihi Wewenangnya Devi Dharmawan, Ivonne Jonathanboooow92Pas encore d'évaluation
- Level 3 Health and Social Care PackDocument735 pagesLevel 3 Health and Social Care PackGeorgiana Deaconu100% (4)
- 49 Ways To Increase Natural Cannabinoids Without Smoking Pot (Including Ways That Decrease Cannabinoids) - SelfhackedDocument27 pages49 Ways To Increase Natural Cannabinoids Without Smoking Pot (Including Ways That Decrease Cannabinoids) - SelfhackedwhsprzPas encore d'évaluation
- History of Experimental PsychologyDocument20 pagesHistory of Experimental PsychologyakmalrahmanPas encore d'évaluation
- Effects of Restricted Feed Intake On Heat Energy BDocument14 pagesEffects of Restricted Feed Intake On Heat Energy BdrcdevaPas encore d'évaluation
- Patient Satisfaction About Hospital Services: A Study From The Outpatient Department of Tertiary Care Hospital, Jabalpur, Madhya Pradesh, IndiaDocument6 pagesPatient Satisfaction About Hospital Services: A Study From The Outpatient Department of Tertiary Care Hospital, Jabalpur, Madhya Pradesh, IndiaVikram AripakaPas encore d'évaluation
- Spinning Mill ProcessDocument10 pagesSpinning Mill ProcessAnees PainkalPas encore d'évaluation
- Safety Management and Culture: The Long Hard RoadDocument24 pagesSafety Management and Culture: The Long Hard RoadCesar J Vicente APas encore d'évaluation
- Cva (Npte)Document16 pagesCva (Npte)papermannerPas encore d'évaluation
- Identifying Depression On Reddit: The Effect of Training DataDocument4 pagesIdentifying Depression On Reddit: The Effect of Training DataZaabaIbnuAhmadPas encore d'évaluation
- HRM Compensation PolicyDocument30 pagesHRM Compensation PolicyAfroza KhanPas encore d'évaluation
- Ventilator Associated Pneumonia (Vap) Sop: V1 February 2018 VAP-02-2018-SK-V1Document6 pagesVentilator Associated Pneumonia (Vap) Sop: V1 February 2018 VAP-02-2018-SK-V1Devi Humairah IrawanPas encore d'évaluation
- Fundamentals of Nursing: Urinary Elimination, Catheterization, Ostomy Care & Pain ManagementDocument29 pagesFundamentals of Nursing: Urinary Elimination, Catheterization, Ostomy Care & Pain ManagementKatrina Issa A. GelagaPas encore d'évaluation
- Individual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledDocument12 pagesIndividual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledTiffanny Diane Agbayani RuedasPas encore d'évaluation