Vous aimerez peut-être aussi
- Step by Step Understanding Technical AnalysisDocument68 pagesStep by Step Understanding Technical Analysisbelwer100% (6)
- CPG Dementia BookletDocument91 pagesCPG Dementia BookletBadrun IbrahimPas encore d'évaluation
- Best Stochastic Trading StrategyDocument5 pagesBest Stochastic Trading StrategyBadrun Ibrahim67% (3)
- Geriatrics AMTSDocument1 pageGeriatrics AMTSBadrun IbrahimPas encore d'évaluation
- Patient - Info/doctor/abbreviated Mental Test AmtDocument3 pagesPatient - Info/doctor/abbreviated Mental Test AmtBadrun IbrahimPas encore d'évaluation
- Pi Is 0891524513001429Document4 pagesPi Is 0891524513001429Badrun IbrahimPas encore d'évaluation
- ACI Cognition Screening For Older AdultsDocument2 pagesACI Cognition Screening For Older AdultsBadrun IbrahimPas encore d'évaluation
- Nature of Growth & DevelopmentDocument12 pagesNature of Growth & DevelopmentBadrun IbrahimPas encore d'évaluation
- Pain On Injection of Propofol: Efficacy of Paracetamol and LidocaineDocument7 pagesPain On Injection of Propofol: Efficacy of Paracetamol and LidocaineBadrun IbrahimPas encore d'évaluation
- Daftar PustakaDocument2 pagesDaftar PustakaBadrun IbrahimPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Adolescent Screening and Assessment Instrument Compendium: For Substance Abuse and Mental Health DisordersDocument21 pagesAdolescent Screening and Assessment Instrument Compendium: For Substance Abuse and Mental Health DisordersIván Rosario VillafañePas encore d'évaluation
- Enteral Tube Administration of Oral Chemotherapy DrugsDocument15 pagesEnteral Tube Administration of Oral Chemotherapy DrugsCoté HuertaPas encore d'évaluation
- CV AustraliaDocument10 pagesCV Australiaralfh1992Pas encore d'évaluation
- Infection - Nursing Test QuestionsDocument58 pagesInfection - Nursing Test QuestionsRNStudent1100% (3)
- Dobutamine IV Infusion for Heart FailureDocument1 pageDobutamine IV Infusion for Heart FailureAnnie SethiPas encore d'évaluation
- Improving Medical Education With TechnologyDocument2 pagesImproving Medical Education With Technologytummalapalli venkateswara raoPas encore d'évaluation
- Hormone Therapy For Prostate Cancer Exploring Current ControversiesDocument8 pagesHormone Therapy For Prostate Cancer Exploring Current ControversiesNenad MladenovicPas encore d'évaluation
- Reservoir Bag Physics J PhilipDocument44 pagesReservoir Bag Physics J PhilipJashim JumliPas encore d'évaluation
- CISP - First Year ReportDocument50 pagesCISP - First Year ReportMANOJ HEMADRIPas encore d'évaluation
- Executive Summary CapstoneDocument3 pagesExecutive Summary Capstoneapi-272956109Pas encore d'évaluation
- Covid Injections For Dummkopfs - A Summary For Us in Flyover CountryDocument74 pagesCovid Injections For Dummkopfs - A Summary For Us in Flyover CountryBerk ShirePas encore d'évaluation
- Unit 5Document44 pagesUnit 5bereket gashuPas encore d'évaluation
- Clinical Case Reports - 2018 - Toh Yoon - A Novel Semi Solidifying Liquid Formula Via The Nasogastric Route To MaintainDocument5 pagesClinical Case Reports - 2018 - Toh Yoon - A Novel Semi Solidifying Liquid Formula Via The Nasogastric Route To MaintainValentina RusuPas encore d'évaluation
- Transmission Precautions ExplainedDocument8 pagesTransmission Precautions Explainedniraj_sd100% (1)
- Social and Public HealthDocument54 pagesSocial and Public HealthMekuriya BeregaPas encore d'évaluation
- Nebuliser - Care of Your NebuliserDocument13 pagesNebuliser - Care of Your NebuliserRahulNargotraPas encore d'évaluation
- Peelings PDFDocument222 pagesPeelings PDFEdy Estévez100% (3)
- 2nd Prof Catalogue 2019 LRDocument40 pages2nd Prof Catalogue 2019 LRGangadhar DungaPas encore d'évaluation
- Question ID Title: Page 14) Page 16)Document3 pagesQuestion ID Title: Page 14) Page 16)AnisulHaquePas encore d'évaluation
- Vaccination Partnership Promotes Preventive HealthcareDocument27 pagesVaccination Partnership Promotes Preventive HealthcareLoanne RamiterrePas encore d'évaluation
- First AidDocument5 pagesFirst AidDencio Jr. Gosing CayatPas encore d'évaluation
- Drugs and Alcohol in TeenagersDocument3 pagesDrugs and Alcohol in TeenagersDavid UrestiPas encore d'évaluation
- Omega-3 Fish OilDocument2 pagesOmega-3 Fish OilAshutosh KumarPas encore d'évaluation
- Resume - Taraneh Sadeghian HaghighiDocument3 pagesResume - Taraneh Sadeghian Haghighiarian tejaratPas encore d'évaluation
- Diseases of The Vitreo-Macular InterfaceDocument126 pagesDiseases of The Vitreo-Macular InterfaceCarlos OrtegaPas encore d'évaluation
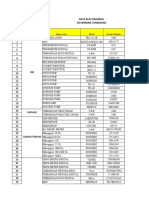
- Data Alat Kalibrasi Rs TNGDocument10 pagesData Alat Kalibrasi Rs TNGHelena LowaPas encore d'évaluation
- Curriculum Vitae: C ErsonalDocument4 pagesCurriculum Vitae: C Ersonalmeenakshi.r.agrawalPas encore d'évaluation
- Ovarian CancerDocument34 pagesOvarian CancerHealth Education Library for People100% (4)
- ComprehensiveUnifiedPolicy TBDocument159 pagesComprehensiveUnifiedPolicy TBallan14_reyesPas encore d'évaluation
- Paracetamol IV AmpuleDocument3 pagesParacetamol IV AmpuleEli Thy IgopPas encore d'évaluation