Vous aimerez peut-être aussi
- 05 Clinical Failures and Its Management in Fixed Partial DentureDocument45 pages05 Clinical Failures and Its Management in Fixed Partial Denturesonal_karania66% (29)
- Periodontal Plastic Surgery: Soft Tissue Grafting Indications and ProceduresDocument44 pagesPeriodontal Plastic Surgery: Soft Tissue Grafting Indications and ProceduresAvita RathPas encore d'évaluation
- Calcium Hydroxide ReviewDocument26 pagesCalcium Hydroxide Reviewkonda_siri83100% (1)
- Oral Wound Healing: Cell Biology and Clinical ManagementD'EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaPas encore d'évaluation
- Essential Tissue Healing of the Face and NeckD'EverandEssential Tissue Healing of the Face and NeckÉvaluation : 5 sur 5 étoiles5/5 (2)
- Urban - Effectiveness of Two Different Lingual Flap Advancing Techniques For Vertical Bone Augmentation in The Posterior MandibleDocument7 pagesUrban - Effectiveness of Two Different Lingual Flap Advancing Techniques For Vertical Bone Augmentation in The Posterior MandibleEliza DraganPas encore d'évaluation
- 08 - Salivary Biomarkers A Periodontal OverviewDocument6 pages08 - Salivary Biomarkers A Periodontal OverviewFisaPas encore d'évaluation
- Gingival InflammationDocument12 pagesGingival InflammationdeenmPas encore d'évaluation
- Developmental Disturbances of Oral and Paraoral StructuresDocument14 pagesDevelopmental Disturbances of Oral and Paraoral StructuresYashmeen XPas encore d'évaluation
- Dental Clinics of North AmericaDocument204 pagesDental Clinics of North Americasam4slPas encore d'évaluation
- Modified Papilla Preservation TechniqueDocument26 pagesModified Papilla Preservation TechniqueWendy JengPas encore d'évaluation
- InflammationDocument14 pagesInflammationPrince AhmedPas encore d'évaluation
- Immunology of Periodontal DiseasesDocument9 pagesImmunology of Periodontal DiseasesoladunniPas encore d'évaluation
- Biologicals: Mito Kobayashi, Tomoyuki Kawase, Makoto Horimizu, Kazuhiro Okuda, Larry F. Wolff, Hiromasa YoshieDocument7 pagesBiologicals: Mito Kobayashi, Tomoyuki Kawase, Makoto Horimizu, Kazuhiro Okuda, Larry F. Wolff, Hiromasa YoshieVijay Prabu GPas encore d'évaluation
- Perio 2000 VOL-76 Treatment of Pathologic Peri-Implant Pocket PDFDocument11 pagesPerio 2000 VOL-76 Treatment of Pathologic Peri-Implant Pocket PDFchandanaPas encore d'évaluation
- Oral IrrigatorDocument30 pagesOral IrrigatorNorman Tri Kusumo100% (1)
- HalitosisDocument6 pagesHalitosispratyusha vallamPas encore d'évaluation
- Rationale of Endodontic TreatmentDocument30 pagesRationale of Endodontic Treatmentaakriti100% (1)
- The Periodontal Pocket PDFDocument9 pagesThe Periodontal Pocket PDFIgnacio PulleyPas encore d'évaluation
- 313 Classification of Periodontal and Peri-Implant Diseases and Conditions 2020 - Part IIDocument52 pages313 Classification of Periodontal and Peri-Implant Diseases and Conditions 2020 - Part IIAbdulrahman100% (1)
- 01 Oral Cavity PDFDocument106 pages01 Oral Cavity PDFGhaydaa Abukhairan0% (1)
- Gingival Crevicular FluidDocument48 pagesGingival Crevicular FluidDUKUZIMANA CONCORDEPas encore d'évaluation
- Bacterial Infections of Oral CavityDocument63 pagesBacterial Infections of Oral CavityAkash Anilkumar Malini60% (5)
- Preventive DentistryDocument70 pagesPreventive Dentistryceudmd3dPas encore d'évaluation
- Local Drug Delivery in PeriodonticsDocument40 pagesLocal Drug Delivery in PeriodonticsruchaPas encore d'évaluation
- New Drug Delivery Systems: A Global OpportunityDocument24 pagesNew Drug Delivery Systems: A Global OpportunityRugun Clara SamosirPas encore d'évaluation
- History & PE of Oral Cavity FinalDocument81 pagesHistory & PE of Oral Cavity Finalapi-3743483Pas encore d'évaluation
- Bacterial Infections of The Oral CavityDocument212 pagesBacterial Infections of The Oral CavitydrrakbdsPas encore d'évaluation
- New Classification For Periodontal Diseases 2017 PDFDocument367 pagesNew Classification For Periodontal Diseases 2017 PDFblokolbPas encore d'évaluation
- Peri Implant Disease PDFDocument32 pagesPeri Implant Disease PDFHajra FarooqPas encore d'évaluation
- Lasers in Oral and Maxillofacial Surgery.Document28 pagesLasers in Oral and Maxillofacial Surgery.Sukhvinder Singh Rana0% (1)
- Imaging in Periodontics PerioDocument49 pagesImaging in Periodontics PerioFourthMolar.comPas encore d'évaluation
- Antibiotics in Periodontics PerioDocument51 pagesAntibiotics in Periodontics PerioSiddhartha BanerjeePas encore d'évaluation
- Povidone Iodine - RevisitedDocument4 pagesPovidone Iodine - RevisitedPatrick153Pas encore d'évaluation
- Intra Canal Medication PDFDocument34 pagesIntra Canal Medication PDFKhalil El HalimyPas encore d'évaluation
- 6 Surgical Periodontal TherapyDocument38 pages6 Surgical Periodontal TherapyPriya SargunanPas encore d'évaluation
- Oral Lichen PlanusDocument7 pagesOral Lichen Planusdrgurpal74100% (1)
- Antibiotics Used in DentistryDocument17 pagesAntibiotics Used in Dentistrymegamarwa50% (2)
- Sonic and Ultrasonic ScalersDocument10 pagesSonic and Ultrasonic ScalersAhmad Abd El-GhaniPas encore d'évaluation
- AGGRESSIVE PERIODONTITIS: AN INTRODUCTIONDocument101 pagesAGGRESSIVE PERIODONTITIS: AN INTRODUCTIONdileep900100% (1)
- Mandibular NerveDocument8 pagesMandibular NerveSridevi KPas encore d'évaluation
- CariesDocument148 pagesCariesSudipto BaraiPas encore d'évaluation
- Clinical Case Studies Proving Long-Term SuccessDocument46 pagesClinical Case Studies Proving Long-Term SuccessJ.A. Lorenz AdlerPas encore d'évaluation
- Aae Systemic AntibioticsDocument8 pagesAae Systemic AntibioticsIulia CiobanuPas encore d'évaluation
- Oral Mucous MembraneDocument36 pagesOral Mucous MembraneFourthMolar.comPas encore d'évaluation
- Pharmacology of Local Anesthetic in DentistryDocument32 pagesPharmacology of Local Anesthetic in DentistryAileen LooPas encore d'évaluation
- PDL DressingsDocument116 pagesPDL DressingsAnvi GuptaPas encore d'évaluation
- Department of Pediatrics and Preventive Dentistry.: Local Anasthesia in Pediatric DentistryDocument27 pagesDepartment of Pediatrics and Preventive Dentistry.: Local Anasthesia in Pediatric DentistrySudip ChakrabortyPas encore d'évaluation
- 7&8 Tooth Extraction (Exodontia)Document28 pages7&8 Tooth Extraction (Exodontia)Muntather Muhsen100% (2)
- Implant and Periodontal ConsiderationsDocument53 pagesImplant and Periodontal ConsiderationsAlphonse ThangapradeepPas encore d'évaluation
- Lecture 2 2021Document7 pagesLecture 2 2021Mateusz RadwańskiPas encore d'évaluation
- Maxillary SinusDocument67 pagesMaxillary SinusDR. NEETI TATIYAPas encore d'évaluation
- Perio-Prog Class 2012Document80 pagesPerio-Prog Class 2012moorenPas encore d'évaluation
- Local AnestheticsDocument93 pagesLocal Anestheticsgeetika100% (1)
- Endodontic MicrobiologyDocument11 pagesEndodontic MicrobiologydigdouwPas encore d'évaluation
- Diagnosis ClassDocument63 pagesDiagnosis ClassRiham AliPas encore d'évaluation
- Interpretation Basics of Cone Beam Computed TomographyD'EverandInterpretation Basics of Cone Beam Computed TomographyÉvaluation : 4 sur 5 étoiles4/5 (1)
- Leukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandLeukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Sports Dentistry: Principles and PracticeD'EverandSports Dentistry: Principles and PracticePeter D. FinePas encore d'évaluation
- Lowe Syndrome (Oculocerebrorenal syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandLowe Syndrome (Oculocerebrorenal syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Systemic Antibiotics in Periodontal Therapy: LJA Heitz-MayfieldDocument6 pagesSystemic Antibiotics in Periodontal Therapy: LJA Heitz-Mayfieldapi-239502672Pas encore d'évaluation
- Zucchelli Desepitelizado 2010Document11 pagesZucchelli Desepitelizado 2010Maximiliano Jara ContrerasPas encore d'évaluation
- Gingival Depigmentation Using Simple De-Epithelization by Bur Abrasion Technique - A Case ReportDocument5 pagesGingival Depigmentation Using Simple De-Epithelization by Bur Abrasion Technique - A Case ReportIJAR JOURNALPas encore d'évaluation
- Athlete RiveraDocument10 pagesAthlete RiveraAvi Auerbach AvilaPas encore d'évaluation
- Aggressive Periodontitis Case ReportDocument4 pagesAggressive Periodontitis Case ReportResa YudhistiPas encore d'évaluation
- Brown Algae Fucoidan's Effect on Oral BacteriaDocument8 pagesBrown Algae Fucoidan's Effect on Oral Bacteria3Racha supremacyPas encore d'évaluation
- Christensen & Luther, 2015Document7 pagesChristensen & Luther, 2015jlkdsjfljsdlfPas encore d'évaluation
- Ayu304447-3680693 101326Document12 pagesAyu304447-3680693 101326satish_CJPas encore d'évaluation
- Dental Hygiene Literature Review TopicsDocument4 pagesDental Hygiene Literature Review Topicsafmzzbfdgoupjx100% (1)
- HAL 49 Critical Decision in PeriodontologyDocument1 pageHAL 49 Critical Decision in PeriodontologyUntuk TugasPas encore d'évaluation
- Assessment of Periodontal Status in Patients With Rheumatoid Arthritis in Kelantan, Malaysia: A Preliminary StudyDocument5 pagesAssessment of Periodontal Status in Patients With Rheumatoid Arthritis in Kelantan, Malaysia: A Preliminary StudyemmypuspitasariPas encore d'évaluation
- RecessionDocument11 pagesRecessionaziz alsohailPas encore d'évaluation
- Oral Path Flipchart 1233Document11 pagesOral Path Flipchart 1233api-397871513Pas encore d'évaluation
- Pregnant Women's Oral Health Impacts Children's Heart HealthDocument23 pagesPregnant Women's Oral Health Impacts Children's Heart Healthvaria5Pas encore d'évaluation
- Ada & AnsiDocument24 pagesAda & Ansikermink100% (3)
- The Effects of Orthodontic Therapy PDFDocument11 pagesThe Effects of Orthodontic Therapy PDFDeasireePas encore d'évaluation
- Mcguire1996 6 PDFDocument8 pagesMcguire1996 6 PDFAngie AriasPas encore d'évaluation
- Antibacterial Effects of Fermented and Cold Press VCO Against Aggregatibacter Actinomycetemcomitans and Porphyromonas GingivalisDocument1 pageAntibacterial Effects of Fermented and Cold Press VCO Against Aggregatibacter Actinomycetemcomitans and Porphyromonas GingivalisMonyet...Pas encore d'évaluation
- Gingival Curretage ScribdDocument2 pagesGingival Curretage ScribdclaudianrjPas encore d'évaluation
- Oral Toxicity Associated With ChemotherapyDocument56 pagesOral Toxicity Associated With ChemotherapyRobertoPas encore d'évaluation
- Distraction Osteogenesis Review PDFDocument20 pagesDistraction Osteogenesis Review PDFMonojit DuttaPas encore d'évaluation
- Curriculum VitaeDocument2 pagesCurriculum VitaeJuan Rafael SilvaPas encore d'évaluation
- Surgical Reconstruction of Interdental Papilla Using Subepithelialconnective Tissue Graft by Microsurgical Technique A Clinical ST 2376 032X 1000229Document6 pagesSurgical Reconstruction of Interdental Papilla Using Subepithelialconnective Tissue Graft by Microsurgical Technique A Clinical ST 2376 032X 1000229neighPas encore d'évaluation
- Immediate implant placement in extraction socketsDocument11 pagesImmediate implant placement in extraction socketsEsmail AhmedPas encore d'évaluation
- Aging and Periodontium: The and Sue WithDocument4 pagesAging and Periodontium: The and Sue Withandreas kevinPas encore d'évaluation
- Treatment 01Document335 pagesTreatment 01HeberLópezRaveloPas encore d'évaluation
- The Periodontal Abscess: A ReviewDocument10 pagesThe Periodontal Abscess: A ReviewRENATO SUDATIPas encore d'évaluation
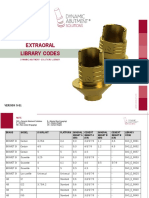
- Extraoral Library Codes: VERSION 5-81Document26 pagesExtraoral Library Codes: VERSION 5-81Zsolt PerényiPas encore d'évaluation