Vous aimerez peut-être aussi
- HandOff SampleToolsDocument9 pagesHandOff SampleToolsOllie EvansPas encore d'évaluation
- The COAT & Review Approach: How to recognise and manage unwell patientsD'EverandThe COAT & Review Approach: How to recognise and manage unwell patientsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Blank Medication Card TemplateDocument1 pageBlank Medication Card Templatemichelle chenPas encore d'évaluation
- Sbar Mini Case StudiesDocument2 pagesSbar Mini Case Studiesapi-367705934Pas encore d'évaluation
- Week 4Document8 pagesWeek 4api-312973588Pas encore d'évaluation
- Code Blue Policy - Adult Care Sites - Calgary ZoneDocument9 pagesCode Blue Policy - Adult Care Sites - Calgary ZoneLLyreOPas encore d'évaluation
- Typhon Case LogDocument3 pagesTyphon Case LogJeremy HallPas encore d'évaluation
- Nursing Assessment Form: A. Demographic DataDocument5 pagesNursing Assessment Form: A. Demographic Datacat_w0m4nPas encore d'évaluation
- Module 1 REVIEW OF THE NURSING PROCESS 1Document3 pagesModule 1 REVIEW OF THE NURSING PROCESS 1hamisi100% (2)
- Nursing Administration AssessmentDocument6 pagesNursing Administration Assessmentkatnebrija89Pas encore d'évaluation
- Screening Test Sensitivity vs SpecificityDocument7 pagesScreening Test Sensitivity vs SpecificityKinuPatel100% (2)
- Documentation: Basic Nursing: Foundations of Skills & Concepts DocumentationDocument8 pagesDocumentation: Basic Nursing: Foundations of Skills & Concepts DocumentationJona GarzonPas encore d'évaluation
- Please Read The Entire Form Carefully Before SigningDocument2 pagesPlease Read The Entire Form Carefully Before SigningKoh LudzPas encore d'évaluation
- Elder Abuse and NelgectDocument10 pagesElder Abuse and Nelgectنادر القحطانيPas encore d'évaluation
- Department of Nursing Initial Competency Validation Checklist: Orientation: RNDocument4 pagesDepartment of Nursing Initial Competency Validation Checklist: Orientation: RNAmeng GosimPas encore d'évaluation
- Perceived Clinical Competence Among Undergraduate Nursing Students in The University of Gondar and Bahir Dar University, Northwest Ethiopia - A Cross-Sectional Institution Based StudyDocument12 pagesPerceived Clinical Competence Among Undergraduate Nursing Students in The University of Gondar and Bahir Dar University, Northwest Ethiopia - A Cross-Sectional Institution Based Studyedy harahapPas encore d'évaluation
- Clinical CasesDocument12 pagesClinical CasesAndreea HanuPas encore d'évaluation
- Medical Assitant ProjectDocument18 pagesMedical Assitant Projectapi-378167354100% (1)
- 05-NIH Stroke ScaleDocument11 pages05-NIH Stroke ScaleMus TikaPas encore d'évaluation
- Patient Case Presentation StructureDocument30 pagesPatient Case Presentation StructureAmira HelayelPas encore d'évaluation
- Emergency Department Orientation for New NursesDocument38 pagesEmergency Department Orientation for New NursesNers SenPas encore d'évaluation
- Responding To A Code BlueDocument33 pagesResponding To A Code Blueamanrup randhawaPas encore d'évaluation
- Restraint CompetencyDocument6 pagesRestraint CompetencyFrederick RyanPas encore d'évaluation
- 05 Nursing Note SampleDocument3 pages05 Nursing Note Sampletesttest testPas encore d'évaluation
- Aprn PresentationDocument12 pagesAprn Presentationapi-234511817Pas encore d'évaluation
- TB QuestionnaireDocument1 pageTB QuestionnaireaplesgjskPas encore d'évaluation
- ADA-Vitamin L Guide Writing Admission OrdersDocument35 pagesADA-Vitamin L Guide Writing Admission Orderssilvercentaur16Pas encore d'évaluation
- Lippincott ProceduresDocument3 pagesLippincott ProceduresYmon TuallaPas encore d'évaluation
- Nursing Audit Tool PDFDocument12 pagesNursing Audit Tool PDFjamiePas encore d'évaluation
- List of Committees With Their Roles and Composition 1. Quality Improvement CommitteeDocument5 pagesList of Committees With Their Roles and Composition 1. Quality Improvement CommitteetanishaPas encore d'évaluation
- Medication Administration Error 3Document16 pagesMedication Administration Error 3Priya bhattiPas encore d'évaluation
- Vital Signs and Early Warning ScoresDocument47 pagesVital Signs and Early Warning Scoresdr_nadheem100% (1)
- ENA Leadership Conference 2013 ProgramDocument17 pagesENA Leadership Conference 2013 ProgramEmergency Nurses AssociationPas encore d'évaluation
- Medication Errors PaperDocument6 pagesMedication Errors Paperapi-542442476Pas encore d'évaluation
- Respiratory SystemDocument9 pagesRespiratory Systemmariel.angeles29Pas encore d'évaluation
- Preceptor EvaluationDocument2 pagesPreceptor Evaluationapi-380898658Pas encore d'évaluation
- Nursing Diagnosis TemplateDocument6 pagesNursing Diagnosis Templatesdk6972Pas encore d'évaluation
- The Importance of An Accurate and Honest Observership Program EvaluationDocument12 pagesThe Importance of An Accurate and Honest Observership Program EvaluationMaria DoukaPas encore d'évaluation
- The 5 Nursing Process StepsDocument124 pagesThe 5 Nursing Process StepsEstrera Ruschelle A.Pas encore d'évaluation
- Emergency Department Operational SOP v1.1 Mar2017Document15 pagesEmergency Department Operational SOP v1.1 Mar2017agelesswapPas encore d'évaluation
- AbbreviationDocument19 pagesAbbreviationJayson NatividadPas encore d'évaluation
- CEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsDocument18 pagesCEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsLauren GarciaPas encore d'évaluation
- Isolation Guidelines PDFDocument209 pagesIsolation Guidelines PDFlimiya varghesePas encore d'évaluation
- Patient Support AreasDocument22 pagesPatient Support AreasVivienne Rozenn LaytoPas encore d'évaluation
- GCOE Provision 4-6Document29 pagesGCOE Provision 4-6Justine May GervacioPas encore d'évaluation
- Documentation and Nurse Practitioner RoleDocument5 pagesDocumentation and Nurse Practitioner RoleEnerolisa ParedesPas encore d'évaluation
- StatementDocument5 pagesStatementtrinity_brannonPas encore d'évaluation
- QI Student Proposal Handoffs PDFDocument6 pagesQI Student Proposal Handoffs PDFDxtr MedinaPas encore d'évaluation
- Observation Summary 2Document5 pagesObservation Summary 2api-493028287Pas encore d'évaluation
- Nursing Process HandoutsDocument10 pagesNursing Process HandoutsNayumi VillanuevaPas encore d'évaluation
- NURS 3305 Syllabus Spring 2022Document13 pagesNURS 3305 Syllabus Spring 2022Chris GongPas encore d'évaluation
- Research Paper - FinalDocument16 pagesResearch Paper - Finalapi-455663099Pas encore d'évaluation
- CVDocument2 pagesCVapi-242412922Pas encore d'évaluation
- SBAR Communication Form: and Progress NoteDocument3 pagesSBAR Communication Form: and Progress NoteTisa Meriel100% (1)
- Rapid Response TeamDocument4 pagesRapid Response TeamMichael SilvaPas encore d'évaluation
- Presentor-: Ruma Sen: MN (Previous) RakconDocument40 pagesPresentor-: Ruma Sen: MN (Previous) Rakconcy100% (1)
- Documentation and ReportingDocument62 pagesDocumentation and ReportingTimPas encore d'évaluation
- Western Australian Patient Identification Policy PDFDocument14 pagesWestern Australian Patient Identification Policy PDFpuspadiniaPas encore d'évaluation
- Summer Study at The University of Colorado BoulderDocument1 pageSummer Study at The University of Colorado BoulderJan MarcPas encore d'évaluation
- NURSING THE CHILDBEARING FAMILY: Passbooks Study GuideD'EverandNURSING THE CHILDBEARING FAMILY: Passbooks Study GuidePas encore d'évaluation
- E2415 PDFDocument4 pagesE2415 PDFdannychacon27Pas encore d'évaluation
- Unit 2 - Programming of 8085 MicroprocessorDocument32 pagesUnit 2 - Programming of 8085 MicroprocessorSathiyarajPas encore d'évaluation
- Characteristics and Elements of A Business Letter Characteristics of A Business LetterDocument3 pagesCharacteristics and Elements of A Business Letter Characteristics of A Business LetterPamela Galang100% (1)
- 1 Ancient-IndiaDocument14 pages1 Ancient-Indiakaushik joshiPas encore d'évaluation
- Comment On Motion To Release Vehicle BeridoDocument3 pagesComment On Motion To Release Vehicle BeridoRaffy PangilinanPas encore d'évaluation
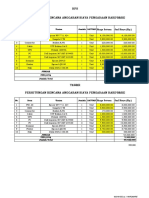
- HPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANDocument2 pagesHPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANYanto AstriPas encore d'évaluation
- Global Pre-Qualification - Registration of Vendors For Supply of Various Raw Materials - ProductsDocument2 pagesGlobal Pre-Qualification - Registration of Vendors For Supply of Various Raw Materials - Productsjavaidkhan83Pas encore d'évaluation
- PORT DEVELOPMENT in MALAYSIADocument25 pagesPORT DEVELOPMENT in MALAYSIAShhkyn MnPas encore d'évaluation
- Marylebone Construction UpdateDocument2 pagesMarylebone Construction UpdatePedro SousaPas encore d'évaluation
- ScriptsDocument6 pagesScriptsDx CatPas encore d'évaluation
- EDMOTO 4th TopicDocument24 pagesEDMOTO 4th TopicAngel Delos SantosPas encore d'évaluation
- Module 3 - Risk Based Inspection (RBI) Based On API and ASMEDocument4 pagesModule 3 - Risk Based Inspection (RBI) Based On API and ASMEAgustin A.Pas encore d'évaluation
- 9 Specific Relief Act, 1877Document20 pages9 Specific Relief Act, 1877mostafa faisalPas encore d'évaluation
- TOPIC 12 Soaps and DetergentsDocument14 pagesTOPIC 12 Soaps and DetergentsKaynine Kiko50% (2)
- Statement. Cash.: M.B.A. Semester-Ill Exadinatioh Working Capital Management Paper-Mba/3103/FDocument2 pagesStatement. Cash.: M.B.A. Semester-Ill Exadinatioh Working Capital Management Paper-Mba/3103/FPavan BasundePas encore d'évaluation
- How To Use Google FormsDocument126 pagesHow To Use Google FormsBenedict Bagube100% (1)
- Voiceless Alveolar Affricate TsDocument78 pagesVoiceless Alveolar Affricate TsZomiLinguisticsPas encore d'évaluation
- Israel Bible MapDocument1 pageIsrael Bible MapMoses_JakkalaPas encore d'évaluation
- MEAB Enewsletter 14 IssueDocument5 pagesMEAB Enewsletter 14 Issuekristine8018Pas encore d'évaluation
- Amadora V CA Case DigestDocument3 pagesAmadora V CA Case DigestLatjing SolimanPas encore d'évaluation
- Temperature Rise HV MotorDocument11 pagesTemperature Rise HV Motorashwani2101Pas encore d'évaluation
- SPACES Nepal - Green Schools Building The FutureDocument3 pagesSPACES Nepal - Green Schools Building The FutureBimal ThapaPas encore d'évaluation
- Effectiveness of Laundry Detergents and Bars in Removing Common StainsDocument9 pagesEffectiveness of Laundry Detergents and Bars in Removing Common StainsCloudy ClaudPas encore d'évaluation
- GeM Bidding 2920423 - 2Document4 pagesGeM Bidding 2920423 - 2Sulvine CharliePas encore d'évaluation
- Bell I Do Final PrintoutDocument38 pagesBell I Do Final PrintoutAthel BellidoPas encore d'évaluation
- Organizational CultureDocument76 pagesOrganizational Culturenaty fishPas encore d'évaluation
- DPS Chief Michael Magliano DIRECTIVE. Arrests Inside NYS Courthouses April 17, 2019 .Document1 pageDPS Chief Michael Magliano DIRECTIVE. Arrests Inside NYS Courthouses April 17, 2019 .Desiree YaganPas encore d'évaluation
- Protein Synthesis: Class Notes NotesDocument2 pagesProtein Synthesis: Class Notes NotesDale HardingPas encore d'évaluation
- A Brief History of The White Nationalist MovementDocument73 pagesA Brief History of The White Nationalist MovementHugenPas encore d'évaluation
- Focus 4 Unit 2 Grammar Quiz 2.5 A GrupaDocument1 pageFocus 4 Unit 2 Grammar Quiz 2.5 A GrupaЕвгения КоноваловаPas encore d'évaluation