Vous aimerez peut-être aussi
- Internal Memo Short Sem July 2022, Unikl Msi - 025630Document1 pageInternal Memo Short Sem July 2022, Unikl Msi - 025630johnjabarajPas encore d'évaluation
- CVCIA PeeGee Plan v2Document6 pagesCVCIA PeeGee Plan v2johnjabarajPas encore d'évaluation
- Signed Fyp Items Delivery (Diploma MDD Jan22) - 085309Document2 pagesSigned Fyp Items Delivery (Diploma MDD Jan22) - 085309johnjabarajPas encore d'évaluation
- Final Exam Engineering MechanicsDocument9 pagesFinal Exam Engineering MechanicsjohnjabarajPas encore d'évaluation
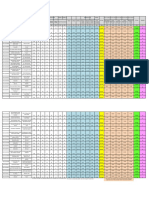
- STRENGTH OF MATERIALS MARKSDocument2 pagesSTRENGTH OF MATERIALS MARKSjohnjabarajPas encore d'évaluation
- Final Year Project 1 Results and GradesDocument1 pageFinal Year Project 1 Results and GradesjohnjabarajPas encore d'évaluation
- Subject Name: Final Year Project 1 Subject Code: Spb49804 Semester: January 2022 Programme: Beta MechanicalDocument3 pagesSubject Name: Final Year Project 1 Subject Code: Spb49804 Semester: January 2022 Programme: Beta MechanicaljohnjabarajPas encore d'évaluation
- Assignment Engineering ScienceDocument10 pagesAssignment Engineering SciencejohnjabarajPas encore d'évaluation
- Eng SC AssignmentDocument2 pagesEng SC AssignmentjohnjabarajPas encore d'évaluation
- Universiti Kuala Lumpur Kampus Cawangan Malaysian Spanish Institute January 2022Document1 pageUniversiti Kuala Lumpur Kampus Cawangan Malaysian Spanish Institute January 2022johnjabarajPas encore d'évaluation
- January 2022 Semester Academic Operation CalendarDocument2 pagesJanuary 2022 Semester Academic Operation CalendarjohnjabarajPas encore d'évaluation
- SignLogbook Faiza Week (1-14) - 051421Document60 pagesSignLogbook Faiza Week (1-14) - 051421johnjabarajPas encore d'évaluation
- TOS scb12103Document2 pagesTOS scb12103johnjabarajPas encore d'évaluation
- BETA Mech FYP2 Marks - July2021 (002) AFIQ ExtensionDocument4 pagesBETA Mech FYP2 Marks - July2021 (002) AFIQ ExtensionjohnjabarajPas encore d'évaluation
- Invoice #30496: John Jabaraj 1651 Persiaran Utama 4 Kulim Utama Fasa 2 Kul 09000 Kulim MalaysiaDocument1 pageInvoice #30496: John Jabaraj 1651 Persiaran Utama 4 Kulim Utama Fasa 2 Kul 09000 Kulim MalaysiajohnjabarajPas encore d'évaluation
- Universiti Kuala Lumpur: Final ExaminationDocument5 pagesUniversiti Kuala Lumpur: Final ExaminationjohnjabarajPas encore d'évaluation
- Engineering ScienceDocument4 pagesEngineering SciencejohnjabarajPas encore d'évaluation
- SDD23503 Strength of Materials (Newcode2017)Document5 pagesSDD23503 Strength of Materials (Newcode2017)johnjabarajPas encore d'évaluation
- Section B: Learning Schedule: Unikl MsiDocument2 pagesSection B: Learning Schedule: Unikl MsijohnjabarajPas encore d'évaluation
- FYP2 Panel For Final Presentation: Name Tittle Panel SupervisorDocument3 pagesFYP2 Panel For Final Presentation: Name Tittle Panel SupervisorjohnjabarajPas encore d'évaluation
- Es Final Exam Set A AnswerDocument20 pagesEs Final Exam Set A AnswerjohnjabarajPas encore d'évaluation
- TPFS - Title Proposal Form Jan 2022Document2 pagesTPFS - Title Proposal Form Jan 2022johnjabarajPas encore d'évaluation
- VectorDocument4 pagesVectorjohnjabarajPas encore d'évaluation
- 3 SCB12103 Engineering Mechanics (CDDH-20W-T1)Document5 pages3 SCB12103 Engineering Mechanics (CDDH-20W-T1)johnjabarajPas encore d'évaluation
- Strength of Materials Course SyllabusDocument6 pagesStrength of Materials Course SyllabusjohnjabarajPas encore d'évaluation
- Group 7 - March 2016Document2 pagesGroup 7 - March 2016johnjabarajPas encore d'évaluation
- Universiti Kuala Lumpur: Final ExaminationDocument1 pageUniversiti Kuala Lumpur: Final ExaminationjohnjabarajPas encore d'évaluation
- SCB23103 - John - MSI-Test 1 (Jul 21) - GradesDocument2 pagesSCB23103 - John - MSI-Test 1 (Jul 21) - GradesjohnjabarajPas encore d'évaluation
- Exam Mech2 Set Aa-1Document4 pagesExam Mech2 Set Aa-1johnjabarajPas encore d'évaluation
- JULY 2021 Det in Mechanical Design and Development (MDD) : SPD39806 Final Year ProjectDocument23 pagesJULY 2021 Det in Mechanical Design and Development (MDD) : SPD39806 Final Year ProjectjohnjabarajPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Centrifugal Compressor Settle Out Conditions TutorialDocument5 pagesCentrifugal Compressor Settle Out Conditions TutorialJHOEARGPas encore d'évaluation
- Concept of Net Zero Energy Buildings (NZEB) - A Literature ReviewDocument16 pagesConcept of Net Zero Energy Buildings (NZEB) - A Literature ReviewJaime PazPas encore d'évaluation
- 2008 27 Summer Wiring Matters Supplementary Equipotential BondingDocument5 pages2008 27 Summer Wiring Matters Supplementary Equipotential BondingPascal DumontPas encore d'évaluation
- Perkins Derate Tables Engine 4000Document20 pagesPerkins Derate Tables Engine 4000Marcello RosiniPas encore d'évaluation
- Material Turbina A GásDocument47 pagesMaterial Turbina A GásGetúlio RibeiroPas encore d'évaluation
- Compressor FinalDocument20 pagesCompressor FinalshihabPas encore d'évaluation
- Journal of Physics EconomicsDocument6 pagesJournal of Physics EconomicsmauudyPas encore d'évaluation
- GEI41047 Rev K - Liquid FuelDocument24 pagesGEI41047 Rev K - Liquid FuelHameed100% (3)
- Part-Turn Worm Gearboxes Gs 160 - Gs 250Document2 pagesPart-Turn Worm Gearboxes Gs 160 - Gs 250SUNIL SINGHPas encore d'évaluation
- EEDC DetailDocument21 pagesEEDC DetailAfrian HindrawijayaPas encore d'évaluation
- Beam Powered PropulsionDocument19 pagesBeam Powered PropulsionSai Sushma100% (1)
- Water Resources EngineeringDocument1 199 pagesWater Resources EngineeringVikaas Jha97% (35)
- IGCSE Term 2 Assessment - Date sheetDocument7 pagesIGCSE Term 2 Assessment - Date sheetKausthubhi KillamsettiPas encore d'évaluation
- Belt Driven 230VAC Generator DatasheetDocument2 pagesBelt Driven 230VAC Generator DatasheetMohamed ElfayomyPas encore d'évaluation
- Engg Chemistry R13 Model Question PapersDocument4 pagesEngg Chemistry R13 Model Question PapersBell P PedPas encore d'évaluation
- Gas Welding Workshop ReportDocument12 pagesGas Welding Workshop ReportDuventhirenPas encore d'évaluation
- Fracture MechanicsDocument31 pagesFracture MechanicsDhany SSat100% (2)
- Heui PDFDocument56 pagesHeui PDFGerman Ramos German Ramos100% (5)
- Aermec WRL 026-161HDocument6 pagesAermec WRL 026-161HMilan PizdunPas encore d'évaluation
- Ezstim Ii: Operator'S ManualDocument29 pagesEzstim Ii: Operator'S ManualBabajee NavirajPas encore d'évaluation
- Manual - IR Nirvana Troubleshooting GuideDocument63 pagesManual - IR Nirvana Troubleshooting GuideKurserg92% (51)
- Everything about steam condensersDocument17 pagesEverything about steam condensersASHOKPas encore d'évaluation
- Science Fair Report 2906Document24 pagesScience Fair Report 2906LONDONPas encore d'évaluation
- Inputs To Piping DisciplineDocument2 pagesInputs To Piping DisciplineJACKMAAAAPas encore d'évaluation
- 4 - Kama - Kde 6500 TWDocument2 pages4 - Kama - Kde 6500 TWJavadPas encore d'évaluation
- Student Exploration: Photosynthesis LabDocument4 pagesStudent Exploration: Photosynthesis LabIranzi Mujanama0% (1)
- Final Diesel DesignDocument111 pagesFinal Diesel DesignJerome JeremiasPas encore d'évaluation
- P Module 6A PDFDocument52 pagesP Module 6A PDFSundareshwar SPas encore d'évaluation
- Mehdi Rahmani Andebili Differential Equations Practice ProblemsDocument109 pagesMehdi Rahmani Andebili Differential Equations Practice ProblemsvdeodaatoPas encore d'évaluation
- HV Generation and Testing 1.0 Slides PDFDocument43 pagesHV Generation and Testing 1.0 Slides PDFzuhairulPas encore d'évaluation