Vous aimerez peut-être aussi
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderD'EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderPas encore d'évaluation
- Percutaneous Imaging-Guided Spinal Facet Joint InjectionsDocument6 pagesPercutaneous Imaging-Guided Spinal Facet Joint InjectionsAlvaro Perez HenriquezPas encore d'évaluation
- Eular Us Course Modulo 5 Tornozelo e PeDocument44 pagesEular Us Course Modulo 5 Tornozelo e PeGustavo Bernardo DamascenoPas encore d'évaluation
- Minimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachD'EverandMinimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachGiorgio PietramaggioriPas encore d'évaluation
- Ultrasound Guided Lower Limb Blocks Tony AllenDocument39 pagesUltrasound Guided Lower Limb Blocks Tony Allenrepre64Pas encore d'évaluation
- Peripheral Nerve Blocks Lower ExtremityDocument53 pagesPeripheral Nerve Blocks Lower ExtremityArief Hariyadi SantosoPas encore d'évaluation
- MSK Us ProtocolsDocument40 pagesMSK Us Protocolsjamir59Pas encore d'évaluation
- Cervical Spine Trauma: Shreya Kangovi Radiology Core, BIDMC July 25th, 2004Document25 pagesCervical Spine Trauma: Shreya Kangovi Radiology Core, BIDMC July 25th, 2004ComagaPas encore d'évaluation
- Ultrasound Guided Interventional Procedures In.13Document14 pagesUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Hill - Workshop - Intro To MSK US Shoulder WS 2014-1Document32 pagesHill - Workshop - Intro To MSK US Shoulder WS 2014-1Raihan LuthfiPas encore d'évaluation
- Platelet-Rich Plasma in Osteoarthritis Treatment: Review of Current EvidenceDocument18 pagesPlatelet-Rich Plasma in Osteoarthritis Treatment: Review of Current EvidenceIrham KhairiPas encore d'évaluation
- Limb Length DiscrepancyDocument2 pagesLimb Length DiscrepancyMuhammed BarznjiPas encore d'évaluation
- Fundamentals of Diagnostic RadiologyDocument52 pagesFundamentals of Diagnostic RadiologyYabets100% (1)
- Knee Differential DiagnosisDocument2 pagesKnee Differential DiagnosisJade Kenneth Gonzales LomansocPas encore d'évaluation
- USG - Hip & Knee-Dr - NarayanDocument92 pagesUSG - Hip & Knee-Dr - NarayancmonmanPas encore d'évaluation
- Regional Anesthesia For Scapular Fracture Surgery: An Educational Review of Anatomy and TechniquesDocument6 pagesRegional Anesthesia For Scapular Fracture Surgery: An Educational Review of Anatomy and TechniquesSean SmythPas encore d'évaluation
- Acetabular FractureDocument136 pagesAcetabular FracturePicha PichiPas encore d'évaluation
- Peroneal Nerve Palsy PDFDocument10 pagesPeroneal Nerve Palsy PDFChristian Reza WibowoPas encore d'évaluation
- Crozer-Keystone Ex Tern Ship ManualDocument187 pagesCrozer-Keystone Ex Tern Ship ManualRihamary CruzPas encore d'évaluation
- Lumbar Radiculopathy Medback Castillo Mendez EDITEDDocument12 pagesLumbar Radiculopathy Medback Castillo Mendez EDITEDSteve ColbertPas encore d'évaluation
- SJAMS 43B 750 754 Thesis Tibial PlateauDocument5 pagesSJAMS 43B 750 754 Thesis Tibial PlateauNisheshJainPas encore d'évaluation
- Collateral Ligament Injury MRIDocument29 pagesCollateral Ligament Injury MRILeksmana AcPas encore d'évaluation
- Suspecting and Diagnosing The Patient With Spondyloarthritis 2021. CLINICSDocument15 pagesSuspecting and Diagnosing The Patient With Spondyloarthritis 2021. CLINICSluisa100% (1)
- Bone AgeDocument65 pagesBone AgeueumanaPas encore d'évaluation
- Diagnosis in OrthopaedicsDocument48 pagesDiagnosis in OrthopaedicsBakta Giri100% (1)
- Quadrilatral and Ischial SocketDocument133 pagesQuadrilatral and Ischial Socketjay prakashPas encore d'évaluation
- Review - Presby Residency ManualDocument400 pagesReview - Presby Residency ManualSneha SutharPas encore d'évaluation
- Treatment of SLAC-CartagenaDocument40 pagesTreatment of SLAC-CartagenaProfesseur Christian DumontierPas encore d'évaluation
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsDocument7 pagesTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersPas encore d'évaluation
- PDFDocument328 pagesPDFBreak DerulsPas encore d'évaluation
- Outpatientassessmentand Managementofthediabeticfoot: John A. DipretaDocument21 pagesOutpatientassessmentand Managementofthediabeticfoot: John A. DipretaAnonymous kdBDppigEPas encore d'évaluation
- LEAN Boards Review CL 2011Document9 pagesLEAN Boards Review CL 2011pudding35Pas encore d'évaluation
- Rheumatology - For BPTsDocument72 pagesRheumatology - For BPTsfire_n_icePas encore d'évaluation
- Journal ReadingDocument7 pagesJournal ReadingTommy HardiantoPas encore d'évaluation
- Braun Neurology Endoscope SystemDocument132 pagesBraun Neurology Endoscope SystemMārcis RancānsPas encore d'évaluation
- Sample ResumeDocument5 pagesSample ResumeAstro BlackPas encore d'évaluation
- EMR Documentation TemplatesDocument25 pagesEMR Documentation TemplatesFlint Ray100% (1)
- Checklist For Physical Examination of Knee PDFDocument13 pagesChecklist For Physical Examination of Knee PDFpadmja4purohitPas encore d'évaluation
- Rheumatology Examination: Physical Examination-N ManoliosDocument7 pagesRheumatology Examination: Physical Examination-N ManoliosRohit SharmaPas encore d'évaluation
- 4.the Pathogenesis of Psoriatic ArthritisDocument12 pages4.the Pathogenesis of Psoriatic ArthritisstuckinbedPas encore d'évaluation
- Long Case OrthopaedicDocument24 pagesLong Case OrthopaedicSyimah UmarPas encore d'évaluation
- Wiki TractographyDocument4 pagesWiki TractographynsurgphotoPas encore d'évaluation
- Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFDocument11 pagesPelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFJulio Cesar Guillen MoralesPas encore d'évaluation
- Ankle Arthrodesis - Screw FixationDocument26 pagesAnkle Arthrodesis - Screw FixationChristopher HoodPas encore d'évaluation
- Aaos PDFDocument4 pagesAaos PDFWisnu CahyoPas encore d'évaluation
- Entrapmentneuropathiesof Theupperextremity: Christopher T. Doughty,, Michael P. BowleyDocument14 pagesEntrapmentneuropathiesof Theupperextremity: Christopher T. Doughty,, Michael P. BowleydwiPas encore d'évaluation
- Tannoury C Failed BackDocument24 pagesTannoury C Failed BackneareastspinePas encore d'évaluation
- Chapter 4 and 4a Introduction To Medicine and DermatologyDocument16 pagesChapter 4 and 4a Introduction To Medicine and DermatologypodmmgfPas encore d'évaluation
- Orthopedics: Notes, 1/eDocument26 pagesOrthopedics: Notes, 1/evkPas encore d'évaluation
- Aaos Pediatric 2020Document57 pagesAaos Pediatric 2020ABUBAKER ZANBOUZIPas encore d'évaluation
- Neurologic AssessmentDocument28 pagesNeurologic AssessmentJoshua KellyPas encore d'évaluation
- Advances in Spinal Stabilization PDFDocument333 pagesAdvances in Spinal Stabilization PDFMateo CortesPas encore d'évaluation
- Ficat and Arlet Staging of Avascular Necrosis of Femoral HeadDocument6 pagesFicat and Arlet Staging of Avascular Necrosis of Femoral HeadFernando Sugiarto0% (1)
- Mri Clinics - Imaging of Sports InjuriesDocument182 pagesMri Clinics - Imaging of Sports Injuriespinky003100% (2)
- Spondylolisthesis: To Reduce or Not Case Discussion: Early Onset ScoliosisDocument36 pagesSpondylolisthesis: To Reduce or Not Case Discussion: Early Onset ScoliosisneareastspinePas encore d'évaluation
- Orthopediatric LWWDocument398 pagesOrthopediatric LWWかちえ ちょうPas encore d'évaluation
- Gpe - 017.1 - Orthopaedic ExaminationDocument3 pagesGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumPas encore d'évaluation
- Charnley Ankle ArthrodesisDocument12 pagesCharnley Ankle Arthrodesisdr_s_ganeshPas encore d'évaluation
- Roux 2013Document7 pagesRoux 2013andrew herringPas encore d'évaluation
- Buprenorphine 2016-7-18Document1 pageBuprenorphine 2016-7-18andrew herringPas encore d'évaluation
- Highland Guidelines - LDK 2013-2-15Document3 pagesHighland Guidelines - LDK 2013-2-15andrew herringPas encore d'évaluation
- K Opiods For Pain BupDocument2 pagesK Opiods For Pain Bupandrew herringPas encore d'évaluation
- Original Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve BlockDocument7 pagesOriginal Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve Blockandrew herringPas encore d'évaluation
- Rib Fracture W: PecsDocument8 pagesRib Fracture W: Pecsandrew herring100% (1)
- Rib Fracture SerratusDocument3 pagesRib Fracture Serratusandrew herring100% (1)
- Ultrasound-Guided Block of TheDocument6 pagesUltrasound-Guided Block of Theandrew herringPas encore d'évaluation
- Intravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-OperatóriaDocument6 pagesIntravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-Operatóriaandrew herringPas encore d'évaluation
- Herring ED Intractable Abdominal pain-N+VDocument1 pageHerring ED Intractable Abdominal pain-N+Vandrew herringPas encore d'évaluation
- 3.2.16.highland Emergency Medicine Journal Club Methods.2Document2 pages3.2.16.highland Emergency Medicine Journal Club Methods.2andrew herringPas encore d'évaluation
- Ketamine As Rescue Treatment FDocument8 pagesKetamine As Rescue Treatment Fandrew herringPas encore d'évaluation
- Dex For Dental Pain & SwellingDocument7 pagesDex For Dental Pain & Swellingandrew herring100% (1)
- Nej MR A 1511480Document9 pagesNej MR A 1511480Tohari Masidi AminPas encore d'évaluation
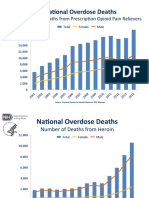
- OPR - Heroin DeathsDocument2 pagesOPR - Heroin Deathsandrew herringPas encore d'évaluation
- CVS Action Plan v2Document1 pageCVS Action Plan v2andrew herringPas encore d'évaluation
- Ultrasound Guided Interventional Procedures In.13Document14 pagesUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringPas encore d'évaluation
- Cedar Crest College Clinical and Concept Map Worksheet For Nursing 330 PediatricsDocument13 pagesCedar Crest College Clinical and Concept Map Worksheet For Nursing 330 Pediatricsapi-405374041Pas encore d'évaluation
- 10 Dapat Tandaan Sa Pagsulat NG Artikulo Sa WikiFilipinoDocument2 pages10 Dapat Tandaan Sa Pagsulat NG Artikulo Sa WikiFilipinoFrancisJudeRafilPas encore d'évaluation
- Ethical Judgments Limit The Methods Available in The Production of Knowledge in Both The Arts and The Natural SciencesDocument5 pagesEthical Judgments Limit The Methods Available in The Production of Knowledge in Both The Arts and The Natural SciencesMilena ŁachPas encore d'évaluation
- Orthorexia Nervosa: HistoryDocument3 pagesOrthorexia Nervosa: HistorySimona LeafuPas encore d'évaluation
- Phylum PlatyhelminthesDocument19 pagesPhylum PlatyhelminthesBudi AfriyansyahPas encore d'évaluation
- 1 66th WHA Provisional AgendaDocument6 pages1 66th WHA Provisional AgendaRenzo R. GuintoPas encore d'évaluation
- Manila Standard Today - July 21, 2012 IssueDocument16 pagesManila Standard Today - July 21, 2012 IssueManila Standard TodayPas encore d'évaluation
- Occlusion - DevelopmentDocument33 pagesOcclusion - Developmentsameerortho100% (1)
- FRE - L3 Core Terminology - 2018Document28 pagesFRE - L3 Core Terminology - 2018RahulPas encore d'évaluation
- The Radiology AssistantDocument30 pagesThe Radiology AssistantIcha IchaPas encore d'évaluation
- Lesson Plan NutritionDocument7 pagesLesson Plan NutritionPraveenPas encore d'évaluation
- Use of Autism Diagnostic Interview1 Adi R in Clinical PracticeDocument1 pageUse of Autism Diagnostic Interview1 Adi R in Clinical Practiceaspire centerPas encore d'évaluation
- 5 Nursing Services Scheduling PolicyDocument7 pages5 Nursing Services Scheduling PolicyVin BitzPas encore d'évaluation
- Clinical Study: Overjet and Overbite Influence On Cyclic Masticatory Movements: A CT StudyDocument7 pagesClinical Study: Overjet and Overbite Influence On Cyclic Masticatory Movements: A CT Studyarya091193Pas encore d'évaluation
- Occupational Health Hazards Among Textile WorkersDocument9 pagesOccupational Health Hazards Among Textile WorkersINSTITUTE OF LEGAL EDUCATIONPas encore d'évaluation
- Toxoplasma GondiiDocument7 pagesToxoplasma GondiiDedy SavradinataPas encore d'évaluation
- Case Presentation OB - GYNDocument14 pagesCase Presentation OB - GYNRaidah Ayesha RazackPas encore d'évaluation
- Module 2 HistopathologyDocument34 pagesModule 2 HistopathologyKim RuizPas encore d'évaluation
- Dental ImplantsDocument1 pageDental ImplantsPaWan VelagaPas encore d'évaluation
- Laboratory Tests InterpretationDocument12 pagesLaboratory Tests InterpretationKaloy Kamao100% (1)
- 09 Marijuana Facts For TeensDocument24 pages09 Marijuana Facts For Teensapi-309082881Pas encore d'évaluation
- DafpusDocument1 pageDafpusJeliny Bintan MaisuriPas encore d'évaluation
- Health and WellnessDocument59 pagesHealth and Wellnessvenkata karthikPas encore d'évaluation
- Aberdeenvaricoseveinsquestionnaire PDFDocument4 pagesAberdeenvaricoseveinsquestionnaire PDFdesyislamiatiPas encore d'évaluation
- Okir A DatuDocument6 pagesOkir A DatuRonel FillomenaPas encore d'évaluation
- Hain GenoType Line Probe Assay TestDocument20 pagesHain GenoType Line Probe Assay Testpacome abdulPas encore d'évaluation
- Goat ManualDocument64 pagesGoat ManualIrfan YaqoobPas encore d'évaluation
- Ventilation: Kinematics and Kinetics.: Thorax Structure and FunctionDocument52 pagesVentilation: Kinematics and Kinetics.: Thorax Structure and FunctionAlejandra RomeroPas encore d'évaluation
- Ulibas V Republic - DigestDocument2 pagesUlibas V Republic - DigesttheamorerosaPas encore d'évaluation
- IM-Module B Summarized Notes (IBD)Document69 pagesIM-Module B Summarized Notes (IBD)DeepbluexPas encore d'évaluation