Vous aimerez peut-être aussi
- Diagnostic Values of Tests For Acromioclavicular Joint PainDocument6 pagesDiagnostic Values of Tests For Acromioclavicular Joint Painarum_negariPas encore d'évaluation
- SaisDocument5 pagesSaiselchinovichileno420Pas encore d'évaluation
- Journal PPT - Imt 3Document39 pagesJournal PPT - Imt 3Iqbal KhanPas encore d'évaluation
- Disability and Related Factors in Patients With Chronic Cervical Myofascial PainDocument8 pagesDisability and Related Factors in Patients With Chronic Cervical Myofascial Painaria tristayanthiPas encore d'évaluation
- Material and MethodologyDocument3 pagesMaterial and MethodologySonam PandyaPas encore d'évaluation
- Goniometric Reliability of Shoulder MeasurementsDocument6 pagesGoniometric Reliability of Shoulder MeasurementssaswepakPas encore d'évaluation
- Rodrigo Py Gonçalves Barreto Bilateral MagneticDocument8 pagesRodrigo Py Gonçalves Barreto Bilateral MagneticfilipecorsairPas encore d'évaluation
- Non-Operative Treatment of Subacromial Impingement Syndrome PDFDocument6 pagesNon-Operative Treatment of Subacromial Impingement Syndrome PDFAnonymous 8viyyVPas encore d'évaluation
- Thermo TomesDocument5 pagesThermo Tomesaaronjdriver2248Pas encore d'évaluation
- Jurnal PrintDocument5 pagesJurnal PrintAnugrah PratamaPas encore d'évaluation
- Sacroiliac Joint Pain Referral Zones: of ofDocument5 pagesSacroiliac Joint Pain Referral Zones: of ofGabriel Gaspar Bike FitPas encore d'évaluation
- J Crad 2007 11 011Document7 pagesJ Crad 2007 11 011Simon Ocares AranguizPas encore d'évaluation
- Cervicothoracic Thrust Manipulation in An Acute Painful Shoulder - A Case ReportDocument6 pagesCervicothoracic Thrust Manipulation in An Acute Painful Shoulder - A Case ReportIJAR JOURNALPas encore d'évaluation
- Prevelance of Piriformis Syndrome in Chronic Low Back Pain Patients. A Clinical Diagnosis With Modified FAIR Test PainPractice20121 PDFDocument9 pagesPrevelance of Piriformis Syndrome in Chronic Low Back Pain Patients. A Clinical Diagnosis With Modified FAIR Test PainPractice20121 PDFAuliadi AnsharPas encore d'évaluation
- Mccre Esh 2013Document1 pageMccre Esh 2013Francisco Javier Luza RamosPas encore d'évaluation
- Accuracy of Physical Examination in Subacromial Impingement SyndromeDocument5 pagesAccuracy of Physical Examination in Subacromial Impingement SyndromeClaudia BuitragoPas encore d'évaluation
- MRI Findings of 26 Patients With Parsonage-Turner SyndromeDocument6 pagesMRI Findings of 26 Patients With Parsonage-Turner SyndromeTopciu Mihaela FeliciaPas encore d'évaluation
- Lumbal Spinal Stenosis ODI ScoreDocument10 pagesLumbal Spinal Stenosis ODI ScoreTusan SidhartaPas encore d'évaluation
- PIIS0003999311007957Document8 pagesPIIS0003999311007957soylahijadeunvampiroPas encore d'évaluation
- Tare de TotDocument25 pagesTare de TotantohebogdanalexPas encore d'évaluation
- Comparative of The Milch Method and The Spaso Method in The Reduction of Anterior Dislocation of ShoulderDocument4 pagesComparative of The Milch Method and The Spaso Method in The Reduction of Anterior Dislocation of ShoulderAnonymous UTUWFODCEYPas encore d'évaluation
- 16 Van Leerdam Et Al J Hand Surg Eur Vol. 2017 Jun 42 5 501 506 AAMDocument13 pages16 Van Leerdam Et Al J Hand Surg Eur Vol. 2017 Jun 42 5 501 506 AAMChristopher Freddy Bermeo RiveraPas encore d'évaluation
- Inclinometer Reliability For Shoulder Ranges of Motion in Individuals With Subacromial Impingement SyndromeDocument8 pagesInclinometer Reliability For Shoulder Ranges of Motion in Individuals With Subacromial Impingement SyndromeMarcela TozzoPas encore d'évaluation
- Clinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitisDocument6 pagesClinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitistriptykhannaPas encore d'évaluation
- Physiotherapy For Anterior Knee Pain: A Randomised Controlled TrialDocument6 pagesPhysiotherapy For Anterior Knee Pain: A Randomised Controlled TrialIshika SharmaPas encore d'évaluation
- Pandian Et Al 2013 Shoulder Taping Reduces Injury and Pain in StrokeDocument6 pagesPandian Et Al 2013 Shoulder Taping Reduces Injury and Pain in StrokeCynthia RodriguesPas encore d'évaluation
- Shoulder Impingement SyndromeDocument6 pagesShoulder Impingement SyndromeluizamgoPas encore d'évaluation
- A New Evaluation Method For Lumbar Spinal Instability: Passive Lumbar Extension TestDocument7 pagesA New Evaluation Method For Lumbar Spinal Instability: Passive Lumbar Extension TestSteven Vindas TrejosPas encore d'évaluation
- Evaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramDocument13 pagesEvaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramZzDel VerdePas encore d'évaluation
- Dorratun Rezky, S. Ked / NIM: 71 2018 042: Dr. Rizal Daulay, Sp. OT MARSDocument33 pagesDorratun Rezky, S. Ked / NIM: 71 2018 042: Dr. Rizal Daulay, Sp. OT MARSzafira anandaPas encore d'évaluation
- Characteristics of Myofascial Pain Syndrome of The Infraspinatus MuscleDocument9 pagesCharacteristics of Myofascial Pain Syndrome of The Infraspinatus Musclearia tristayanthiPas encore d'évaluation
- Piva ErhardDocument10 pagesPiva ErhardJulie RosePas encore d'évaluation
- Ilter 2015Document8 pagesIlter 2015Ahmad Awaludin TaslimPas encore d'évaluation
- Shoulder and Elbow OITE - 2012 2013 2014Document204 pagesShoulder and Elbow OITE - 2012 2013 2014ICH KhuyPas encore d'évaluation
- The Diagnosis and Treatment of The Cervical VertigoDocument5 pagesThe Diagnosis and Treatment of The Cervical VertigoDjumadi AkbarPas encore d'évaluation
- Cervical DiscographyDocument8 pagesCervical DiscographyYhoga Timur LagaPas encore d'évaluation
- TER Piriformis Muscle SyndromeDocument13 pagesTER Piriformis Muscle SyndromeJorge Lucas JimenezPas encore d'évaluation
- Reliability and Diagnostic Validity of The Slump Knee Bend Neurodynamic Test For Upper/mid Lumbar Nerve Root Compression: A Pilot StudyDocument6 pagesReliability and Diagnostic Validity of The Slump Knee Bend Neurodynamic Test For Upper/mid Lumbar Nerve Root Compression: A Pilot StudyFlávio GuimarãesPas encore d'évaluation
- Sarimo 2011Document4 pagesSarimo 2011Pe T. ErPas encore d'évaluation
- Evaluation of Benign Paroxysmal Positional Vertigo in American Football PlayersDocument4 pagesEvaluation of Benign Paroxysmal Positional Vertigo in American Football PlayersEnvhy WinaPas encore d'évaluation
- Tens 1Document8 pagesTens 1marcelogascon.oPas encore d'évaluation
- The Effects of A Conservative Rehabilitation Program For Multidirectional Instability of The ShoulderDocument8 pagesThe Effects of A Conservative Rehabilitation Program For Multidirectional Instability of The ShoulderHernando Enrique Willie J.Pas encore d'évaluation
- Poster PapersDocument262 pagesPoster PapersLeonardo RodríguezPas encore d'évaluation
- Risk Prediction For Development of Traumatic Cervical Spinal Cord Injury Without Spinal InstabilityDocument7 pagesRisk Prediction For Development of Traumatic Cervical Spinal Cord Injury Without Spinal InstabilityTantriSaptennoPattiradjawanePas encore d'évaluation
- To Analyse The Short Term Effect of Upper Trapezius Inhibition Taping in Patients With Mechanical Neck PainDocument8 pagesTo Analyse The Short Term Effect of Upper Trapezius Inhibition Taping in Patients With Mechanical Neck PainDr. Krishna N. SharmaPas encore d'évaluation
- Superior Laryngeal Nerve Neuralgia: Case Series and Review of Anterior Neck Pain SyndromesDocument4 pagesSuperior Laryngeal Nerve Neuralgia: Case Series and Review of Anterior Neck Pain SyndromesjtbattaPas encore d'évaluation
- A Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051Document8 pagesA Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051sebafigueroa94Pas encore d'évaluation
- Investigation of Sagittal Thoracic Spinal Curvature and MobilityDocument7 pagesInvestigation of Sagittal Thoracic Spinal Curvature and MobilityDr.Khalid GhaznaviPas encore d'évaluation
- 1103 Full PDFDocument5 pages1103 Full PDFlionkingPas encore d'évaluation
- Seguimiento A 5 Años PTGH ReversaDocument7 pagesSeguimiento A 5 Años PTGH Reversamarcelogascon.oPas encore d'évaluation
- Acute LBP ScreenDocument6 pagesAcute LBP ScreenIsnaenyEraKartikaPas encore d'évaluation
- RNM Dinamica 2Document6 pagesRNM Dinamica 2Alfredo GuiroyPas encore d'évaluation
- John E. Brown, Jason O. Jaeger, Todd A. Polatis, Alexander J. Peters, Paul A. Oakley, Deed E. HarrisonDocument11 pagesJohn E. Brown, Jason O. Jaeger, Todd A. Polatis, Alexander J. Peters, Paul A. Oakley, Deed E. HarrisonJose JiménezPas encore d'évaluation
- Jarbo OJSM Lever TestDocument7 pagesJarbo OJSM Lever Testashlyn granthamPas encore d'évaluation
- Physical Examination Tests For Hip Dysfunction and Injury: March 2015Document8 pagesPhysical Examination Tests For Hip Dysfunction and Injury: March 2015wladjaPas encore d'évaluation
- Suprascapular Nerve Block Versus Steroid Injection For Non-Specific Shoulder PainDocument7 pagesSuprascapular Nerve Block Versus Steroid Injection For Non-Specific Shoulder PainTri KurniawanPas encore d'évaluation
- Validity of The Lateral Gliding Test As Tool ForDocument7 pagesValidity of The Lateral Gliding Test As Tool ForFelippe GuarigliaPas encore d'évaluation
- Resonance Arthrography Estimating The Dimensions of The Rotator Interval With Use of MagneticDocument7 pagesResonance Arthrography Estimating The Dimensions of The Rotator Interval With Use of MagneticKirubakaran Saraswathy PattabiramanPas encore d'évaluation
- Immediate Effects of 2 Types of Braces On Pain and Grip Strength in People With Lateral Epicondylalgia: A Randomized Controlled TrialDocument9 pagesImmediate Effects of 2 Types of Braces On Pain and Grip Strength in People With Lateral Epicondylalgia: A Randomized Controlled TrialRodrigo HamadaPas encore d'évaluation
- Korean Hand Acupuncture LectureDocument66 pagesKorean Hand Acupuncture LectureDavid Drepak67% (3)
- Science of The HeartDocument72 pagesScience of The HeartEvrim Kuran100% (1)
- Sullivan Siegelman Retention Exam With AnswersDocument9 pagesSullivan Siegelman Retention Exam With AnswersJed A. MartirPas encore d'évaluation
- Overview of The Nervous System: Lesson A1.1Document40 pagesOverview of The Nervous System: Lesson A1.1Khobie PabilicoPas encore d'évaluation
- Higher Cortical Functions and Basis of LanguageDocument78 pagesHigher Cortical Functions and Basis of Languagelovelots1234Pas encore d'évaluation
- ماكزلو3Document16 pagesماكزلو3haidergamer658Pas encore d'évaluation
- Morphology McqsDocument8 pagesMorphology McqsHiba Shah100% (2)
- DPT SyllabusDocument277 pagesDPT Syllabusshahidmahboob60100% (1)
- Working With Ankle Mobility, Part I (Myofascial Techniques)Document5 pagesWorking With Ankle Mobility, Part I (Myofascial Techniques)Advanced-Trainings.com100% (4)
- Exclusivepreview Mcqsinforensicmedicineandtoxicology6ebyreddy 110827052724 Phpapp01Document16 pagesExclusivepreview Mcqsinforensicmedicineandtoxicology6ebyreddy 110827052724 Phpapp01prasadhrao20Pas encore d'évaluation
- 37 Posture Yang Short FormDocument3 pages37 Posture Yang Short Formschorleworle100% (1)
- Direct Factors Affecting The PeriodontiumDocument4 pagesDirect Factors Affecting The PeriodontiumHayley WelshPas encore d'évaluation
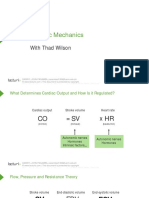
- Cardiac Mechanics: With Thad WilsonDocument26 pagesCardiac Mechanics: With Thad WilsonpasambalyrradjohndarPas encore d'évaluation
- Muscles of The Foot (Table)Document2 pagesMuscles of The Foot (Table)Neil Victor Ongco Pajugot0% (1)
- Match The Words and The PicturesDocument4 pagesMatch The Words and The PicturesJa Mi LahPas encore d'évaluation
- 2nd Year Past Papers UHS PDFDocument92 pages2nd Year Past Papers UHS PDFAhmad UsmanPas encore d'évaluation
- (1912) Practical Guide of Physical Education - Georges Hebert (Includes Parkour)Document33 pages(1912) Practical Guide of Physical Education - Georges Hebert (Includes Parkour)Samurai_Chef100% (3)
- Hagerman Et Al. (2006) - A Pre Game Soccer Warm Up PDFDocument5 pagesHagerman Et Al. (2006) - A Pre Game Soccer Warm Up PDFMarko BrzakPas encore d'évaluation
- Lower Extremity Physical Therapy ExercisesDocument13 pagesLower Extremity Physical Therapy ExercisesShruti100% (1)
- Productos La 1Document6 pagesProductos La 1Anderson GarzonPas encore d'évaluation
- Orthopedic Implants CatalogDocument112 pagesOrthopedic Implants CatalogMuhammad Shoaib JavedPas encore d'évaluation
- I. Muscles ActivatedDocument3 pagesI. Muscles ActivatedSerifa PasovicPas encore d'évaluation
- Periodization PowerDocument3 pagesPeriodization Powertinerete_100% (1)
- Thyroid Hormone Therapy of Hypothyroidism in PregnancyDocument8 pagesThyroid Hormone Therapy of Hypothyroidism in PregnancySoul DreamPas encore d'évaluation
- This Study Resource Was: WEEKS 5-8Document6 pagesThis Study Resource Was: WEEKS 5-8Carudel0% (1)
- The-Nervous-System-Written ReportDocument5 pagesThe-Nervous-System-Written ReportHeileen S. San GabrielPas encore d'évaluation
- Patellar Tendinosus - The Vert Code-EliteDocument4 pagesPatellar Tendinosus - The Vert Code-Elitelebron100% (2)
- 3rd Quarter Science 10 Week 3Document28 pages3rd Quarter Science 10 Week 3Aple RigorPas encore d'évaluation
- Lateral Calcaneal Artery Skin FlapDocument8 pagesLateral Calcaneal Artery Skin FlapLuiggi FayadPas encore d'évaluation
- Centric RelationDocument18 pagesCentric RelationKrupali JainPas encore d'évaluation