Vous aimerez peut-être aussi
- A Travel Medicine CaseDocument65 pagesA Travel Medicine CaseDiskta W RonicaPas encore d'évaluation
- Catatonia, Neuroleptic Malignant Syndrome, and Cotard Syndrome in A 22-Year-Old Woman - A Case ReportDocument3 pagesCatatonia, Neuroleptic Malignant Syndrome, and Cotard Syndrome in A 22-Year-Old Woman - A Case ReportDiskta W RonicaPas encore d'évaluation
- Paediatrica Indonesiana: M. Sholeh Kosim, N.P. Noerpramana, Asril Aminullah, Suharyo HadisaputroDocument6 pagesPaediatrica Indonesiana: M. Sholeh Kosim, N.P. Noerpramana, Asril Aminullah, Suharyo HadisaputroDiskta W RonicaPas encore d'évaluation
- Diagnosis of Scabies With DermosDocument2 pagesDiagnosis of Scabies With DermosDiskta W RonicaPas encore d'évaluation
- Diagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDocument8 pagesDiagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDiskta W RonicaPas encore d'évaluation
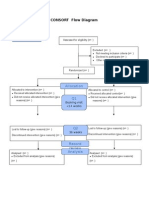
- Additional File 1: CONSORT Flow Diagram: EnrollmentDocument1 pageAdditional File 1: CONSORT Flow Diagram: EnrollmentDiskta W RonicaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Booster Class ABPSY HandoutsDocument16 pagesBooster Class ABPSY HandoutsEunice BasarioPas encore d'évaluation
- 29.4 Sleep Neurology.2023Document317 pages29.4 Sleep Neurology.2023velto anjosPas encore d'évaluation
- Call of Cthulhu - More Adventures in Arkham CountryDocument178 pagesCall of Cthulhu - More Adventures in Arkham Countryrobin82% (11)
- Neurobiology and Neuroprotective Benefits of Sleep.4 PDFDocument23 pagesNeurobiology and Neuroprotective Benefits of Sleep.4 PDFchanguito17Pas encore d'évaluation
- 6a - Ready For Advanced SB Edited - 78 - 1Document3 pages6a - Ready For Advanced SB Edited - 78 - 1ANddfsdsfsPas encore d'évaluation
- Sleep and Sleep Disorders: Velayudhan Mohan KumarDocument8 pagesSleep and Sleep Disorders: Velayudhan Mohan KumarmeiutaPas encore d'évaluation
- 1 - Diagnostic Pre-TestDocument11 pages1 - Diagnostic Pre-Testkasturia wira amarizPas encore d'évaluation
- recalls 4 - NP VDocument9 pagesrecalls 4 - NP VsaguiguitpPas encore d'évaluation
- Bab 7Document27 pagesBab 7bangarudaugtherPas encore d'évaluation
- Krister Ann Jimenez ACTIVITY 14 ParagraphDocument17 pagesKrister Ann Jimenez ACTIVITY 14 ParagraphJamie JimenezPas encore d'évaluation
- Psy - Mod 3Document25 pagesPsy - Mod 3Daev Thara RanjithPas encore d'évaluation
- Soal Bahasa Inggris SIMAK UI 2013 PDFDocument20 pagesSoal Bahasa Inggris SIMAK UI 2013 PDFTiara Rahmadianti AlawiPas encore d'évaluation
- Joiner 2018 The Neurobiological Basis of Sleep and Sleep DisordersDocument11 pagesJoiner 2018 The Neurobiological Basis of Sleep and Sleep DisordersAldo GuascoPas encore d'évaluation
- Nidra - SleepDocument15 pagesNidra - SleepSreedhar RaoPas encore d'évaluation
- Abnormal Psychology (Outline Reviewer) PDFDocument39 pagesAbnormal Psychology (Outline Reviewer) PDFClaire Irish D. BorjaPas encore d'évaluation
- Introduction To Psychology: States of ConsciousnessDocument27 pagesIntroduction To Psychology: States of ConsciousnessCharlie Ken Cruz-GrazaPas encore d'évaluation
- NarcolepsyDocument12 pagesNarcolepsyapi-489712369Pas encore d'évaluation
- The Prevalence of Sleep Disorders in College Students Impact On Academic PerformanceDocument8 pagesThe Prevalence of Sleep Disorders in College Students Impact On Academic PerformancehaniszaniiiPas encore d'évaluation
- Sleep Wake DisordersDocument5 pagesSleep Wake DisordersIsabel CastilloPas encore d'évaluation
- Modafinil AnnotatedDocument13 pagesModafinil AnnotatedMistah RoflcopterPas encore d'évaluation
- The Study of Human Sleep: A Historical Perspective: William C DementDocument6 pagesThe Study of Human Sleep: A Historical Perspective: William C DementKrisha ann MesanaPas encore d'évaluation
- Psych Chap 4+5Document26 pagesPsych Chap 4+5lmaoheartsPas encore d'évaluation
- SleepDocument78 pagesSleepbiswajitsinha100% (4)
- 41 Prep GuideDocument73 pages41 Prep Guidedaljit chahalPas encore d'évaluation
- Physiology of SleepDocument36 pagesPhysiology of SleepTanisha DiwanPas encore d'évaluation
- Sleep MedicineDocument8 pagesSleep MedicineCarlos HernándezPas encore d'évaluation
- NarcolepsyDocument25 pagesNarcolepsysnackwellsPas encore d'évaluation
- Chapter 3 Neuroimmune Aspects of Sleep and Wakefulness: August 2016Document20 pagesChapter 3 Neuroimmune Aspects of Sleep and Wakefulness: August 2016Ganjar AdityoPas encore d'évaluation
- Stahl's 1st Ed Child & AdolDocument388 pagesStahl's 1st Ed Child & AdolfpPas encore d'évaluation
- Brown2012 SleepWakefulnessReviewDocument101 pagesBrown2012 SleepWakefulnessReviewvkasPas encore d'évaluation