Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Dr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementDocument34 pagesDr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementajescoolPas encore d'évaluation
- Dr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementDocument34 pagesDr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementajescoolPas encore d'évaluation
- The Male UrethraDocument5 pagesThe Male UrethraajescoolPas encore d'évaluation
- Laporan Harian TGL 4 Agustus 2015Document7 pagesLaporan Harian TGL 4 Agustus 2015ajescoolPas encore d'évaluation
- 5 Minute Pediatric ConsultDocument5 pages5 Minute Pediatric Consultajescool0% (4)
- Contoh Majalah PIDocument6 pagesContoh Majalah PIajescoolPas encore d'évaluation
- Erythromycin As A Prokinetic Agent in Preterm Neonates: A Systematic ReviewDocument6 pagesErythromycin As A Prokinetic Agent in Preterm Neonates: A Systematic ReviewajescoolPas encore d'évaluation
- TMP - 6100-Tardive PGMay04Article3Document7 pagesTMP - 6100-Tardive PGMay04Article3ajescoolPas encore d'évaluation
- Jadwal HarianDocument3 pagesJadwal HarianajescoolPas encore d'évaluation
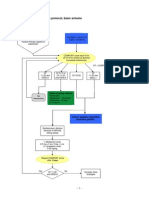
- Sedation Protocol Basic SchemeDocument2 pagesSedation Protocol Basic SchemeajescoolPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Fundamentals in Nursing Lesson #1 INTRODUCTORY CONCEPTSDocument6 pagesFundamentals in Nursing Lesson #1 INTRODUCTORY CONCEPTSSophia Duquinlay100% (1)
- Isbi Practice Guidelines For Burn Care, Part 2: SciencedirectDocument90 pagesIsbi Practice Guidelines For Burn Care, Part 2: SciencedirectDella pinkaPas encore d'évaluation
- Health Psychology: Bio Psychosocial Perspective: Ranya Al-Mandawi Dr. Tyrin Stevenson Psych 331Document6 pagesHealth Psychology: Bio Psychosocial Perspective: Ranya Al-Mandawi Dr. Tyrin Stevenson Psych 331Ranya NajiPas encore d'évaluation
- Health 7: Learning More About Noncommunicable Diseases Written Report About CancerDocument2 pagesHealth 7: Learning More About Noncommunicable Diseases Written Report About CancerRafaella Feroza CastroPas encore d'évaluation
- Medical Service Citizen's Charter FY 2023Document12 pagesMedical Service Citizen's Charter FY 2023admin OESPAPas encore d'évaluation
- Riddle of DeathDocument2 pagesRiddle of DeathReka182Pas encore d'évaluation
- Ms Question 1Document33 pagesMs Question 1yra capiliPas encore d'évaluation
- Gynae Obs NuggetsDocument20 pagesGynae Obs Nuggetsdrusmansaleem100% (1)
- Airway Management in TraumaDocument9 pagesAirway Management in TraumaAnonymous h0DxuJTPas encore d'évaluation
- Advance in MaterialsDocument10 pagesAdvance in Materialssami robalinoPas encore d'évaluation
- Fields of NursingDocument8 pagesFields of NursingOmie TumanguilPas encore d'évaluation
- DRTP Announcement 2012-EnglishDocument2 pagesDRTP Announcement 2012-EnglishHengameh JavaheryPas encore d'évaluation
- Report AyendeDocument13 pagesReport AyendeAbubakar RabiuPas encore d'évaluation
- CDC PoliciesDocument2 pagesCDC PoliciesMonteza Dela SernaPas encore d'évaluation
- PM PFC MatrixDocument4 pagesPM PFC MatrixFamed residentsPas encore d'évaluation
- Assignment in FAMCOMDocument1 pageAssignment in FAMCOMFeyre LunaPas encore d'évaluation
- Add Risk Min MeasDocument12 pagesAdd Risk Min MeasVladimir KostovskiPas encore d'évaluation
- National TB Control Program Form 7 - Referral FormDocument1 pageNational TB Control Program Form 7 - Referral FormAre Pee EtcPas encore d'évaluation
- Coping With Addiction: 6 Dysfunctional Family RolesDocument4 pagesCoping With Addiction: 6 Dysfunctional Family RolesMy LanePas encore d'évaluation
- English For Medicine - A Doctor's ViewDocument6 pagesEnglish For Medicine - A Doctor's ViewАнна ОлексинPas encore d'évaluation
- Drug Information Bulletin 05 07Document4 pagesDrug Information Bulletin 05 07amritaryaaligarghPas encore d'évaluation
- Nursing Diagnosis Common Health Problems That Develop During InfamcyDocument5 pagesNursing Diagnosis Common Health Problems That Develop During InfamcyNur SanaaniPas encore d'évaluation
- Tubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSDocument12 pagesTubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSAulia PuspitaPas encore d'évaluation
- Aromatherapy in Psychiatric DisordersDocument24 pagesAromatherapy in Psychiatric Disordersxiuhtlaltzin100% (3)
- Challenges Faced by Pakistani Healthcare SystemDocument4 pagesChallenges Faced by Pakistani Healthcare SystemMustafa MahmoodPas encore d'évaluation
- ReflectionDocument11 pagesReflectionSarahJane100% (1)
- Child Find PowerpointDocument15 pagesChild Find PowerpointRose Marie Mario0% (1)
- Ar ResumeDocument2 pagesAr Resumeapi-462238327Pas encore d'évaluation
- Final English 211c Part ADocument4 pagesFinal English 211c Part Aapi-341958041Pas encore d'évaluation
- Nurse Writing 003 OET Practice Letter by PASS OETDocument3 pagesNurse Writing 003 OET Practice Letter by PASS OETTwila Abuedo78% (9)