Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Dr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementDocument34 pagesDr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementajescoolPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Laporan Harian TGL 4 Agustus 2015Document7 pagesLaporan Harian TGL 4 Agustus 2015ajescoolPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Dr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementDocument34 pagesDr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementajescoolPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Male UrethraDocument5 pagesThe Male UrethraajescoolPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- 5 Minute Pediatric ConsultDocument5 pages5 Minute Pediatric Consultajescool0% (4)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Contoh Majalah PIDocument6 pagesContoh Majalah PIajescoolPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Erythromycin As A Prokinetic Agent in Preterm Neonates: A Systematic ReviewDocument6 pagesErythromycin As A Prokinetic Agent in Preterm Neonates: A Systematic ReviewajescoolPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
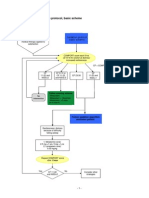
- Sedation Protocol Basic SchemeDocument2 pagesSedation Protocol Basic SchemeajescoolPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Jadwal HarianDocument3 pagesJadwal HarianajescoolPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- TMP - 6100-Tardive PGMay04Article3Document7 pagesTMP - 6100-Tardive PGMay04Article3ajescoolPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Blood and Tissue NematodesDocument37 pagesBlood and Tissue NematodesjelenaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Wuchereria Bancrofti Brugia Malayi Loa Loa Onchocerca Volvulus Mansonella Perstans Mansonella Ozzardi Dracunculus MedinensisDocument4 pagesWuchereria Bancrofti Brugia Malayi Loa Loa Onchocerca Volvulus Mansonella Perstans Mansonella Ozzardi Dracunculus MedinensisJoshua TrinidadPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Vector BiologyDocument21 pagesVector BiologyMrimona ChakrabortyPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- FCM Group3 FilariasisDocument90 pagesFCM Group3 FilariasisAngela CaguitlaPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Wunchereria Bancrofti: Brugia MalayiDocument6 pagesWunchereria Bancrofti: Brugia MalayiGela Reyes100% (1)
- Phylum Nematoda (Revised) 2014 EditionDocument188 pagesPhylum Nematoda (Revised) 2014 EditionArchieDuquePas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- WuchereriozaDocument37 pagesWuchereriozaSteames EaPas encore d'évaluation
- Nematodes 1. Enterobius VermicularisDocument19 pagesNematodes 1. Enterobius VermicularisAngelica Joy GonzalesPas encore d'évaluation
- Human Health and Disease - CBSE Notes For Class 12 Biology - Learn CBSEDocument15 pagesHuman Health and Disease - CBSE Notes For Class 12 Biology - Learn CBSEDr. Vinod GuptaPas encore d'évaluation
- ThesisDocument197 pagesThesisAnil BatraPas encore d'évaluation
- FILARIADocument25 pagesFILARIAKristina DavidPas encore d'évaluation
- Week 13 Tremadotes and NematodesDocument36 pagesWeek 13 Tremadotes and NematodesKatrina Kaycee B. AraPas encore d'évaluation
- Human Health and DiseasesDocument24 pagesHuman Health and DiseasesAnujith AnuPas encore d'évaluation
- Intestinal Nematodes (Unholy Trinity)Document6 pagesIntestinal Nematodes (Unholy Trinity)DAN JR. M. BAUSAPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- ElephantiasisDocument8 pagesElephantiasiscoltrane_x100% (1)
- Filarial Worm: Richard David Silvestre, RMT, MSMT 9 C 0Document13 pagesFilarial Worm: Richard David Silvestre, RMT, MSMT 9 C 0Hearts heavy Moms spaghettiPas encore d'évaluation
- Metazoa A ReviewerDocument4 pagesMetazoa A ReviewerMJ LomuntadPas encore d'évaluation
- Brugia TimoriDocument6 pagesBrugia TimoriNurul Farhana IsmailPas encore d'évaluation
- Filarial Diseases Are - Lymphatic Filariasis - Onchocerciasis (Subcutan Filariasis)Document30 pagesFilarial Diseases Are - Lymphatic Filariasis - Onchocerciasis (Subcutan Filariasis)perisaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Report PARA Lymphatic Filarial Nematodes Group 2 Adalid Asug AustriaDocument28 pagesReport PARA Lymphatic Filarial Nematodes Group 2 Adalid Asug AustriaDaniel AustriaPas encore d'évaluation
- Common Parasites and Diseases of ManDocument14 pagesCommon Parasites and Diseases of Manpramodrp2007Pas encore d'évaluation
- PHD Research ProposalDocument8 pagesPHD Research ProposalMalik Ijaz Khan100% (1)
- Farmakologi Obat Kusta Dan Antiparasit 2015Document84 pagesFarmakologi Obat Kusta Dan Antiparasit 2015Alex FerdinandPas encore d'évaluation
- Elephantiasis: Report AboutDocument8 pagesElephantiasis: Report AboutAmjadRashidPas encore d'évaluation
- Major Tropical Diseases - Prof. Dr. Sugeng JuwonoDocument48 pagesMajor Tropical Diseases - Prof. Dr. Sugeng JuwonosittihajarPas encore d'évaluation
- Phylum Nematoda 13Document132 pagesPhylum Nematoda 13Iseth ISeth100% (1)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Pathology STB 212Document16 pagesPathology STB 212fagadeprecious59Pas encore d'évaluation
- Parasitology - Blood & Tissue - W Bancrofti B Malayi - PresentationDocument43 pagesParasitology - Blood & Tissue - W Bancrofti B Malayi - PresentationNicole ManogPas encore d'évaluation
- FCM 1.6 - NFEP (Filariasis)Document10 pagesFCM 1.6 - NFEP (Filariasis)ZazaPas encore d'évaluation
- Blood and Tissue NematodesDocument60 pagesBlood and Tissue NematodesJefferson SorianoPas encore d'évaluation