Vous aimerez peut-être aussi
- Laboratory Data in EHRs 2014Document20 pagesLaboratory Data in EHRs 2014sairi_nagarajuPas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationD'EverandTextbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationPas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordD'EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordPas encore d'évaluation
- Ahima Data Quality Management ModelDocument11 pagesAhima Data Quality Management Modelselinasimpson2301Pas encore d'évaluation
- Clinical Audit ToolkitDocument41 pagesClinical Audit ToolkitDewi Ratna Sari100% (1)
- Clinical Documentation Improvement (CDI) TrainingDocument6 pagesClinical Documentation Improvement (CDI) Trainingmaricel bismaniPas encore d'évaluation
- Care ManualDocument70 pagesCare ManualQMx2014Pas encore d'évaluation
- Ahimajournal 2015 07 DLDocument73 pagesAhimajournal 2015 07 DLDarrin OpdyckePas encore d'évaluation
- Assg Codingcasestudies 20171109 Ah102 KPDocument1 pageAssg Codingcasestudies 20171109 Ah102 KPapi-427618755Pas encore d'évaluation
- Clinical ValidationDocument39 pagesClinical ValidationMohammed HammedPas encore d'évaluation
- 10 Principle in Medical DocumentationDocument4 pages10 Principle in Medical DocumentationKKCDIAL100% (1)
- Assignment 1Document4 pagesAssignment 1mp1757100% (1)
- Em Coding TablesDocument2 pagesEm Coding Tablesapi-270179959Pas encore d'évaluation
- HCC Coding Feb 2022 ICD-10 InformantDocument2 pagesHCC Coding Feb 2022 ICD-10 InformantSonali PawarPas encore d'évaluation
- National Guideline For Patient Safety Incident Reporting and Learning in South Africa Version 2 - Web LayoutDocument82 pagesNational Guideline For Patient Safety Incident Reporting and Learning in South Africa Version 2 - Web LayoutSheena Mabaquiao-PadernalPas encore d'évaluation
- Coding For Medical Home VisitsDocument14 pagesCoding For Medical Home VisitsSicColoPas encore d'évaluation
- Medical Transcription Industry: Prepared byDocument27 pagesMedical Transcription Industry: Prepared byrohitpatel203100% (1)
- EDE 5th Ed - VDocument99 pagesEDE 5th Ed - VJanet WhitePas encore d'évaluation
- Cdip - 4Document58 pagesCdip - 4SURESHPas encore d'évaluation
- Asrs 2018 Mastering Retina Coding Joy WoodkeDocument79 pagesAsrs 2018 Mastering Retina Coding Joy Woodkeapi-405859281Pas encore d'évaluation
- Documentation and Coding Presentation Focuses on Risk AdjustmentDocument24 pagesDocumentation and Coding Presentation Focuses on Risk AdjustmentVANESSAPas encore d'évaluation
- Analytics Landscape in Healthcare-1Document24 pagesAnalytics Landscape in Healthcare-1positiveworker88Pas encore d'évaluation
- HSMN Healthcare Payment MethodologiesDocument20 pagesHSMN Healthcare Payment MethodologiesMarvin Whitfield100% (1)
- 2007 Guidelines For ClinicalDocument16 pages2007 Guidelines For ClinicalSumitha JeraldPas encore d'évaluation
- CPHQ Detailed Content OutlineDocument8 pagesCPHQ Detailed Content Outlineempire707Pas encore d'évaluation
- Medical DocumentationDocument42 pagesMedical Documentationtummalapalli venkateswara raoPas encore d'évaluation
- Ahimajournal 2015 08 DLDocument69 pagesAhimajournal 2015 08 DLDarrin OpdyckePas encore d'évaluation
- OIG-Hospice Quality Care ReportDocument45 pagesOIG-Hospice Quality Care ReportMaria Tomasch100% (1)
- Standard Coding Guideline ICD-10-TM 2006Document192 pagesStandard Coding Guideline ICD-10-TM 2006api-3835927100% (1)
- Utilization Review Coordinator: Passbooks Study GuideD'EverandUtilization Review Coordinator: Passbooks Study GuidePas encore d'évaluation
- Specification of Use Cases For Information Management Practices in Healthcare: Patient Registration Use CaseDocument24 pagesSpecification of Use Cases For Information Management Practices in Healthcare: Patient Registration Use Casecooking with shab'sPas encore d'évaluation
- Electronic Medical RecordsDocument39 pagesElectronic Medical Recordsleyaljesus leyaljesusPas encore d'évaluation
- CRC Coding Boot Camp 2019 FINALDocument2 pagesCRC Coding Boot Camp 2019 FINALRuban Kumar0% (1)
- Guide Clinical Audit LeadsDocument40 pagesGuide Clinical Audit LeadsppeterarmstrongPas encore d'évaluation
- Sician Advisor's Guide To Clinical Documentation Improvem: Phy EntDocument28 pagesSician Advisor's Guide To Clinical Documentation Improvem: Phy EntBudi YunantoPas encore d'évaluation
- Unusual May-Thurner Syndrome CaseDocument5 pagesUnusual May-Thurner Syndrome CaseJ. Ruben HermannPas encore d'évaluation
- ICD 10 Training Sessions Training AgendaDocument3 pagesICD 10 Training Sessions Training AgendaAntonSusantoPas encore d'évaluation
- Cdip - 3Document86 pagesCdip - 3SURESHPas encore d'évaluation
- Blue Collar Billing CodingDocument18 pagesBlue Collar Billing CodingShell VenkatPas encore d'évaluation
- Risk Scoring in Health Insurance-A PrimerDocument27 pagesRisk Scoring in Health Insurance-A PrimerdimitrisaPas encore d'évaluation
- Cost-Effective Urgent Care Center Reduces ED OveruseDocument6 pagesCost-Effective Urgent Care Center Reduces ED Overusedaron_vchulekPas encore d'évaluation
- HCC Training Manual: Risk Adjustment Coding GuidelinesDocument112 pagesHCC Training Manual: Risk Adjustment Coding GuidelinesKrishna Kamuni100% (1)
- DocumentationDocument13 pagesDocumentationNathaniel Karl Enin Pulido100% (1)
- Differences between Health Informatics and Health Information ManagementDocument3 pagesDifferences between Health Informatics and Health Information ManagementDavid MeléndezPas encore d'évaluation
- MedicalRecordsManual PDFDocument126 pagesMedicalRecordsManual PDFnurhaidahPas encore d'évaluation
- HL7Document13 pagesHL7sony100% (3)
- Medical Transcription Industry FactsDocument2 pagesMedical Transcription Industry FactsSrinivas Pandian0% (1)
- Identifying Patient Safety PrioritiesDocument10 pagesIdentifying Patient Safety PrioritiesReybs -isabella CalubPas encore d'évaluation
- (AMA) CPT 2021 Professional EditionDocument3 824 pages(AMA) CPT 2021 Professional EditionjbmbritoPas encore d'évaluation
- Medical Terminology On CPC Exam2 - YouTubeDocument2 pagesMedical Terminology On CPC Exam2 - YouTubedgina8800Pas encore d'évaluation
- Value Based Care, Reimbursement ModelsDocument3 pagesValue Based Care, Reimbursement ModelsAlexandria NovaPas encore d'évaluation
- A few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentD'EverandA few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentPas encore d'évaluation
- Basics of Evaluation and ManagementDocument45 pagesBasics of Evaluation and ManagementRoaring King100% (2)
- Principles of Healthcare Reimbursement: Sixth EditionDocument28 pagesPrinciples of Healthcare Reimbursement: Sixth EditionDestiny Hayes100% (2)
- Fun Facts About ICD-10 HandoutDocument7 pagesFun Facts About ICD-10 HandoutDhsc01Pas encore d'évaluation
- Rhs Exam OutlineDocument7 pagesRhs Exam OutlineKim SteiningerPas encore d'évaluation
- eClinicalWorks Guide for CliniciansDocument40 pageseClinicalWorks Guide for CliniciansStephany GrandersonPas encore d'évaluation
- @@assessment of Medical Documentation As Per Joint Commission InternationDocument6 pages@@assessment of Medical Documentation As Per Joint Commission InternationNahari ArifinPas encore d'évaluation
- Healthcare Environmental Services A Complete Guide - 2020 EditionD'EverandHealthcare Environmental Services A Complete Guide - 2020 EditionPas encore d'évaluation
- Supervising Registered Nurse: Passbooks Study GuideD'EverandSupervising Registered Nurse: Passbooks Study GuidePas encore d'évaluation
- Joy's Knowledge Quiz AnswersDocument1 pageJoy's Knowledge Quiz AnswersjoyturualloPas encore d'évaluation
- Steps To Christ Bahasa IndonesiaDocument112 pagesSteps To Christ Bahasa Indonesiajoyturuallo100% (1)
- 50 Piano Classics, Easy°Document10 pages50 Piano Classics, Easy°joyturualloPas encore d'évaluation
- Picture Grammar For Children - StarterDocument51 pagesPicture Grammar For Children - Starterpialorena100% (5)
- Lent & Easter Bible Stories: Triumphal Entry to AscensionDocument12 pagesLent & Easter Bible Stories: Triumphal Entry to AscensionjoyturualloPas encore d'évaluation
- Icd oDocument250 pagesIcd oInnovRaditaPas encore d'évaluation
- ICD10CM FY2013 Full PDF TableofNeoplasmsDocument43 pagesICD10CM FY2013 Full PDF TableofNeoplasmsjoyturualloPas encore d'évaluation
- Seni Mengenal Paper CraftDocument0 pageSeni Mengenal Paper CraftRudi SetiawanPas encore d'évaluation
- Surgical Instruments Can Be Generally Divided Into Six Classes by FunctionDocument8 pagesSurgical Instruments Can Be Generally Divided Into Six Classes by FunctionjoyturualloPas encore d'évaluation
- (E-Book) Teaching English To ChildrenDocument119 pages(E-Book) Teaching English To Childrenemmaromera95% (41)
- Seni Mengenal Paper CraftDocument0 pageSeni Mengenal Paper CraftRudi SetiawanPas encore d'évaluation
- Songbook Good News! Gospel Album IIIDocument36 pagesSongbook Good News! Gospel Album IIIEdmilson Cruz SilvaPas encore d'évaluation
- 25 Latino Craft ProjectDocument92 pages25 Latino Craft Projectjoyturuallo100% (2)
- Medical Record Form Igd and TreatmentDocument200 pagesMedical Record Form Igd and TreatmentjoyturualloPas encore d'évaluation
- Medical Record Administration and Health Care Doc 21 Jul 06.8522101Document208 pagesMedical Record Administration and Health Care Doc 21 Jul 06.8522101joyturualloPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- (E-Book) Teaching English To ChildrenDocument119 pages(E-Book) Teaching English To Childrenemmaromera95% (41)
- Askep FormDocument12 pagesAskep Formjoyturuallo50% (2)
- Mastering Medical Terminology Australia and New Zealand Walker 9780729541114Document39 pagesMastering Medical Terminology Australia and New Zealand Walker 9780729541114joyturualloPas encore d'évaluation
- ICD9CMDocument470 pagesICD9CMBayyinah ArdianPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- ICD9CM 2007d8Document458 pagesICD9CM 2007d8SpaljkoPas encore d'évaluation
- Word Medterm SyllabusDocument41 pagesWord Medterm SyllabusjoyturualloPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Prefix, Root, Suffix Meaning Example: Medical Terminology Medical Prefixes, Roots, and SuffixesDocument7 pagesPrefix, Root, Suffix Meaning Example: Medical Terminology Medical Prefixes, Roots, and SuffixesJansher Ali Chohan100% (1)
- Guidelines TBC TerbaruDocument160 pagesGuidelines TBC TerbaruSutoto MoeljadiPas encore d'évaluation
- Mastering Medical Terminology Australia and New Zealand Walker 9780729541114Document39 pagesMastering Medical Terminology Australia and New Zealand Walker 9780729541114joyturualloPas encore d'évaluation
- Conceptual Framework for Improving Pediatric Intensive CareDocument4 pagesConceptual Framework for Improving Pediatric Intensive CareArmstrong AsenaviPas encore d'évaluation
- WBC Non Neoplastic DisordersDocument10 pagesWBC Non Neoplastic Disordersthomas palmejarPas encore d'évaluation
- CGN Pediatric 1 Lesson 2Document20 pagesCGN Pediatric 1 Lesson 2okumu atanasPas encore d'évaluation
- Tinnitus Causes and TreatmentDocument3 pagesTinnitus Causes and TreatmentTinnituscausesandtreatment Tinnituscausesandtreatment100% (1)
- Classification of Hernia: (CITATION Amr15 /L 1057)Document3 pagesClassification of Hernia: (CITATION Amr15 /L 1057)dianPas encore d'évaluation
- Colon Cleansing, Cleanse - Net Colon Plaque - Mucoid PlaqueDocument15 pagesColon Cleansing, Cleanse - Net Colon Plaque - Mucoid Plaquetigerlo75100% (1)
- PHARMA BulletsDocument6 pagesPHARMA BulletsRhea Anne VeraPas encore d'évaluation
- Rest and Sleep Study Guide AnswersDocument7 pagesRest and Sleep Study Guide AnswersvickisscribdPas encore d'évaluation
- Thomas Pynchon-The Crying Lot of 49Document56 pagesThomas Pynchon-The Crying Lot of 49RobertoBanda100% (3)
- HomelessDocument8 pagesHomelessapi-520141947Pas encore d'évaluation
- Adult-Inpatient Eating Disorder GuidelinesDocument18 pagesAdult-Inpatient Eating Disorder GuidelinesJuanCarlos Yogi100% (1)
- AS Geography: Case StudiesDocument26 pagesAS Geography: Case StudiesBrittany FarrantPas encore d'évaluation
- Train Your Brain Build A Framework For Clear ThinkingDocument235 pagesTrain Your Brain Build A Framework For Clear ThinkingyashyiPas encore d'évaluation
- Acupuncture: How It Works, Uses, Benefits, and RisksDocument48 pagesAcupuncture: How It Works, Uses, Benefits, and RisksKim CorpuzPas encore d'évaluation
- Diagnosing Periodic ParalysisDocument46 pagesDiagnosing Periodic Paralysisthelegend 2022Pas encore d'évaluation
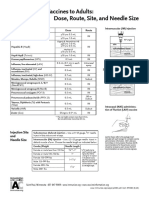
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 pageAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashPas encore d'évaluation
- Nursing Care Plan for ChickenpoxDocument2 pagesNursing Care Plan for ChickenpoxAkeroPas encore d'évaluation
- Enterobius Vermicularis (Pinworm) : Statpearls (Internet)Document6 pagesEnterobius Vermicularis (Pinworm) : Statpearls (Internet)Nosa MnPas encore d'évaluation
- Entity EHS Incident ReportDocument5 pagesEntity EHS Incident ReportwritemeyouPas encore d'évaluation
- PEMF Machine Destroys Parasitic InfectionsDocument2 pagesPEMF Machine Destroys Parasitic InfectionskjprnewsPas encore d'évaluation
- Health QuizDocument6 pagesHealth QuizBrith FranklinPas encore d'évaluation
- Dietary Analysis ProjectDocument3 pagesDietary Analysis ProjectMichelle Davis0% (1)
- Concept Map SeizuresDocument1 pageConcept Map SeizuresMary GiuntiniPas encore d'évaluation
- Introduction To MicrobiologyDocument27 pagesIntroduction To MicrobiologyNicoel67% (3)
- History of DohDocument3 pagesHistory of Dohleslie ann gaspar100% (2)
- Poligen & MultifaktorDocument49 pagesPoligen & MultifaktorLovina Falendini AndriPas encore d'évaluation
- Assessing Body Temperature SitesDocument3 pagesAssessing Body Temperature SitesJUANJOSEFOXPas encore d'évaluation
- Pandemic challenges faced in rural IndiaDocument9 pagesPandemic challenges faced in rural IndiaPREJA PATELPas encore d'évaluation
- Perinial Absecess Case StudyDocument7 pagesPerinial Absecess Case StudymicahatiensaPas encore d'évaluation
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいPas encore d'évaluation