Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Daftar PustakaDocument3 pagesDaftar PustakaSilverius Seantoni SabellaPas encore d'évaluation
- Tuberculosis/General InformationDocument2 pagesTuberculosis/General InformationKatherine McNennyPas encore d'évaluation
- Buku Dpho Askes Tahun 2013Document142 pagesBuku Dpho Askes Tahun 2013yanuar_anggoro100% (1)
- Daftar PustakaDocument2 pagesDaftar PustakaSilverius Seantoni SabellaPas encore d'évaluation
- Hemoragik Syok NewDocument20 pagesHemoragik Syok NewDarna SiskaPas encore d'évaluation
- Magnetic Resonansi CholangioPancreatografiDocument17 pagesMagnetic Resonansi CholangioPancreatografiSilverius Seantoni SabellaPas encore d'évaluation
- BedahDocument8 pagesBedahFebrianaPas encore d'évaluation
- Daftar PustakaDocument3 pagesDaftar PustakaSilverius Seantoni SabellaPas encore d'évaluation
- Daftar PustakaDocument3 pagesDaftar PustakaSilverius Seantoni SabellaPas encore d'évaluation
- Bacterial Meningitis and Meningococcal SepticaemiaDocument53 pagesBacterial Meningitis and Meningococcal SepticaemiaSilverius Seantoni SabellaPas encore d'évaluation
- Daftar PustakaDocument3 pagesDaftar PustakaSilverius Seantoni SabellaPas encore d'évaluation
- Contact DermatitisDocument1 pageContact DermatitisSilverius Seantoni SabellaPas encore d'évaluation
- Meningitis: Frequently Asked QuestionsDocument3 pagesMeningitis: Frequently Asked QuestionsSilverius Seantoni SabellaPas encore d'évaluation
- Ageing Changes of The Eyelids and Lacrimal SystemDocument10 pagesAgeing Changes of The Eyelids and Lacrimal SystemSilverius Seantoni SabellaPas encore d'évaluation
- PIHDocument30 pagesPIHPatcharavit PloynumponPas encore d'évaluation
- Diagnosis and Management of Placenta PreviaDocument6 pagesDiagnosis and Management of Placenta PreviaNoveno Semestre FmuaqPas encore d'évaluation
- Pre and EclampsiaDocument29 pagesPre and EclampsiaSilverius Seantoni SabellaPas encore d'évaluation
- Placenta PreviaDocument2 pagesPlacenta PreviaSilverius Seantoni SabellaPas encore d'évaluation
- Prevention of PreeclampsiaDocument10 pagesPrevention of PreeclampsiaSilverius Seantoni SabellaPas encore d'évaluation
- High Blood PressureDocument2 pagesHigh Blood PressureSilverius Seantoni SabellaPas encore d'évaluation
- Bone Tumors and Tumor-Like LesionsDocument22 pagesBone Tumors and Tumor-Like LesionsSilverius Seantoni SabellaPas encore d'évaluation
- Jurnal Plasenta PreviaDocument10 pagesJurnal Plasenta Previadiah_201192Pas encore d'évaluation
- Mitral StenosisDocument23 pagesMitral StenosisSilverius Seantoni SabellaPas encore d'évaluation
- A Comprehensive Analysis of 51 Neonates With Congenital Intestinal AtresiaDocument5 pagesA Comprehensive Analysis of 51 Neonates With Congenital Intestinal AtresiaSilverius Seantoni SabellaPas encore d'évaluation
- Letter of RecommendationDocument2 pagesLetter of RecommendationSilverius Seantoni SabellaPas encore d'évaluation
- Icd 10Document170 pagesIcd 10Silverius Seantoni SabellaPas encore d'évaluation
- Anemia Chronic Disease-Dr - FifyDocument4 pagesAnemia Chronic Disease-Dr - FifySilverius Seantoni SabellaPas encore d'évaluation
- Insuficiencia MitralDocument13 pagesInsuficiencia MitralSilverius Seantoni SabellaPas encore d'évaluation
- Pancytopenia DR - RiadiDocument10 pagesPancytopenia DR - RiadiSilverius Seantoni SabellaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Childhood BlindnessDocument14 pagesChildhood BlindnessAditya Arya PutraPas encore d'évaluation
- Can't Place That SmellDocument2 pagesCan't Place That SmellkatweaselPas encore d'évaluation
- Bionic Eye ReportDocument46 pagesBionic Eye ReportJHANSI .NPas encore d'évaluation
- Anatomy and Physiology of Vestibular Organ and NeuralDocument56 pagesAnatomy and Physiology of Vestibular Organ and NeuralVineet Chadha0% (1)
- Anatomy and Physiology of The EyeDocument3 pagesAnatomy and Physiology of The EyecarminaduriasPas encore d'évaluation
- Hearing SensitivityDocument1 pageHearing SensitivityMarcus Philip GonzalesPas encore d'évaluation
- الدكتور سامي عطا دعسان استشاري طب وجراحة العيون والقرنية مركز دعسان للعيون medics index member 7122010Document6 pagesالدكتور سامي عطا دعسان استشاري طب وجراحة العيون والقرنية مركز دعسان للعيون medics index member 7122010jordanmedicsPas encore d'évaluation
- SOAL KELAS 8-WPS OfficeDocument6 pagesSOAL KELAS 8-WPS OfficeLina LagaPas encore d'évaluation
- Neuronitis Vestibular PDFDocument18 pagesNeuronitis Vestibular PDFvalesiegmundPas encore d'évaluation
- Optic DiscDocument126 pagesOptic DiscRielz ThereaperzPas encore d'évaluation
- Construction of Human EyeDocument16 pagesConstruction of Human EyeJovi AbabanPas encore d'évaluation
- L10 Analysis ProcedureDocument10 pagesL10 Analysis Procedureyoho hohoPas encore d'évaluation
- Skripsi. Jurnal Untan - Ac.id Miopi PDFDocument20 pagesSkripsi. Jurnal Untan - Ac.id Miopi PDFrifkaraihanaPas encore d'évaluation
- Intro To OphthDocument20 pagesIntro To OphthHassan RazaPas encore d'évaluation
- Anosmia and HyposmiaDocument4 pagesAnosmia and HyposmiafaradillaPas encore d'évaluation
- Elementsandprinciples Poster2Document1 pageElementsandprinciples Poster2api-310282544Pas encore d'évaluation
- CH 15Document8 pagesCH 15naguguPas encore d'évaluation
- Cataract Case StudyDocument11 pagesCataract Case Studyibheng_ling67% (9)
- Sistem Sensorik: Dr. Astri Handayani M.Biomed Bagian Fisiologi Fakultas Kedokteran Universitas TrisaktiDocument58 pagesSistem Sensorik: Dr. Astri Handayani M.Biomed Bagian Fisiologi Fakultas Kedokteran Universitas TrisaktiharsheenaPas encore d'évaluation
- 8L Sound and Hearing Multiple Choice TestDocument3 pages8L Sound and Hearing Multiple Choice Testapi-3698146Pas encore d'évaluation
- The John Colvin Saturday Morning Ophthalmology Lectures Series 2015Document5 pagesThe John Colvin Saturday Morning Ophthalmology Lectures Series 2015LynertheanPas encore d'évaluation
- Good Afternoon Ladies and GentlemanDocument2 pagesGood Afternoon Ladies and GentlemanDDBPas encore d'évaluation
- Eye MD Examination Report Form - CopyrightDocument1 pageEye MD Examination Report Form - CopyrightsolihaPas encore d'évaluation
- Ophthalmology Final Questions (2010-2012) : Pseudophakia Is The Presence of A False Lens That Cannot AccommodateDocument39 pagesOphthalmology Final Questions (2010-2012) : Pseudophakia Is The Presence of A False Lens That Cannot Accommodateazryhafify84% (19)
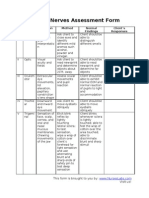
- Cranial Nerves Assessment FormDocument3 pagesCranial Nerves Assessment Formmhel03_chickmagnetPas encore d'évaluation
- Diopter Focus of ANVIS EyepiecesDocument39 pagesDiopter Focus of ANVIS Eyepieceswildan mullerPas encore d'évaluation
- Lay Forum NotesDocument7 pagesLay Forum NotesCleoGomezPas encore d'évaluation
- Assessment of Eyes and EarsDocument31 pagesAssessment of Eyes and EarsShahmeerPas encore d'évaluation
- Osram-Os Led-Fundamentals Mesopic Vision v1 4-2-141Document16 pagesOsram-Os Led-Fundamentals Mesopic Vision v1 4-2-141Adolf ReyesPas encore d'évaluation
- Chronic Benign Paroxysmal Positional Vertigo (BPPVDocument2 pagesChronic Benign Paroxysmal Positional Vertigo (BPPVicarosalernoPas encore d'évaluation