Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Adult Medical Emergencies HandbookDocument317 pagesAdult Medical Emergencies HandbookRasheid Mekki100% (16)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Gut Health Guidebook 9 22Document313 pagesGut Health Guidebook 9 2219760227Pas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- 10a General Pest Control Study GuideDocument128 pages10a General Pest Control Study GuideRomeo Baoson100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- VBA 21 526ez AREDocument12 pagesVBA 21 526ez AREBiniam GirmaPas encore d'évaluation
- Canadian Pharmacy Review Ver1Document6 pagesCanadian Pharmacy Review Ver1Dr-Usman Khan30% (10)
- LP MAPEH 9 (Health)Document4 pagesLP MAPEH 9 (Health)Delima Ninian100% (2)
- Preterm Prelabour Rupture of MembranesDocument12 pagesPreterm Prelabour Rupture of MembranesSeptiany Indahsari DjanPas encore d'évaluation
- Oet Test Material: Occupational English Test Reading Sub-Test NursingDocument13 pagesOet Test Material: Occupational English Test Reading Sub-Test NursingRyu Tse33% (3)
- Management of Stage III Non-Small Cell Lung Cancer - UpToDateDocument23 pagesManagement of Stage III Non-Small Cell Lung Cancer - UpToDateRasheid MekkiPas encore d'évaluation
- Five Elements Chart TableDocument7 pagesFive Elements Chart TablePawanPas encore d'évaluation
- Tamiflu and ADHDDocument10 pagesTamiflu and ADHDlaboewe100% (2)
- Roadmap For TelemedicineDocument48 pagesRoadmap For TelemedicinePradip Gupta100% (2)
- Cancer in Sub-Saharan Africa 2015Document49 pagesCancer in Sub-Saharan Africa 2015Rasheid MekkiPas encore d'évaluation
- 2015 Asco EdbookDocument924 pages2015 Asco EdbookRasheid MekkiPas encore d'évaluation
- Understanding Money Handbook PDFDocument46 pagesUnderstanding Money Handbook PDFRasheid MekkiPas encore d'évaluation
- Milestones in Cancer NATURE 0Document17 pagesMilestones in Cancer NATURE 0bioletimPas encore d'évaluation
- NICE Guidelines-Prostate CA 01:14Document48 pagesNICE Guidelines-Prostate CA 01:14Rasheid MekkiPas encore d'évaluation
- Milestones in Cancer NATURE 0Document17 pagesMilestones in Cancer NATURE 0bioletimPas encore d'évaluation
- Systemic Treatment of Metastatic Breast Cancer in Women: ChemotherapyDocument18 pagesSystemic Treatment of Metastatic Breast Cancer in Women: ChemotherapyRasheid MekkiPas encore d'évaluation
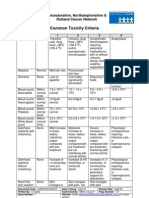
- Common Toxicity CriteriaDocument3 pagesCommon Toxicity CriteriaRasheid MekkiPas encore d'évaluation
- Metabolites 02 00303Document34 pagesMetabolites 02 00303Rasheid MekkiPas encore d'évaluation
- Program Implementation With The Health Team: Packages of Essential Services For Primary HealthcareDocument1 pageProgram Implementation With The Health Team: Packages of Essential Services For Primary Healthcare2A - Nicole Marrie HonradoPas encore d'évaluation
- Information On The Use of Domperidone To Increase Milk Production in Lactating WomenDocument3 pagesInformation On The Use of Domperidone To Increase Milk Production in Lactating WomenKhairul HananPas encore d'évaluation
- Fat Soluble VitaminsDocument20 pagesFat Soluble VitaminsWati WindayaniPas encore d'évaluation
- Delayed Homicides and The Proximate Cause.8Document5 pagesDelayed Homicides and The Proximate Cause.8rheanditahafsaPas encore d'évaluation
- Msds ChloroformDocument9 pagesMsds ChloroformAhmad ArisandiPas encore d'évaluation
- Class IX - Worksheet 4 (Comprehension & Writing Skill)Document6 pagesClass IX - Worksheet 4 (Comprehension & Writing Skill)Anis FathimaPas encore d'évaluation
- Classifying Giant Cell Lesions A Review.21Document5 pagesClassifying Giant Cell Lesions A Review.21shehla khanPas encore d'évaluation
- Operator MGC Ultima PFX - English - 142152-001rCDocument65 pagesOperator MGC Ultima PFX - English - 142152-001rCEvangelosPas encore d'évaluation
- BM Procedure and ProcessingDocument28 pagesBM Procedure and ProcessingNidhi JaisPas encore d'évaluation
- DSM OcdDocument2 pagesDSM Ocdnmyza89Pas encore d'évaluation
- Escala de Apatia de StarksteinDocument6 pagesEscala de Apatia de StarksteinVanessa HernandezPas encore d'évaluation
- Sri Lanka - Averting A National Nutrition Anomaly 2Document16 pagesSri Lanka - Averting A National Nutrition Anomaly 2Rushan LakdimuthuPas encore d'évaluation
- 2018 Surgical Rescue in Medical PatientsDocument11 pages2018 Surgical Rescue in Medical PatientsgiseladlrPas encore d'évaluation
- Paper Roleplay Group 3Document7 pagesPaper Roleplay Group 3Endah Ragil SaputriPas encore d'évaluation
- Test Bank For Pilbeams Mechanical Ventilation 5th Edition CairoDocument13 pagesTest Bank For Pilbeams Mechanical Ventilation 5th Edition Cairochowryurduq0krhPas encore d'évaluation
- Clinchers: RheumatologyDocument22 pagesClinchers: RheumatologyvarrakeshPas encore d'évaluation
- ESC - 2021 - The Growing Role of Genetics in The Understanding of Cardiovascular Diseases - Towards Personalized MedicineDocument5 pagesESC - 2021 - The Growing Role of Genetics in The Understanding of Cardiovascular Diseases - Towards Personalized MedicineDini SuhardiniPas encore d'évaluation
- Long-Term Survey of Tooth Loss in 600 PtsDocument15 pagesLong-Term Survey of Tooth Loss in 600 PtsAndy HePas encore d'évaluation
- GENERAL RISK ASSESSMENT Mechatronics LaboratoryDocument2 pagesGENERAL RISK ASSESSMENT Mechatronics LaboratoryJason TravisPas encore d'évaluation
- 24 Bio Fertilization of BananaDocument6 pages24 Bio Fertilization of Bananamiceli57Pas encore d'évaluation