Vous aimerez peut-être aussi
- MICS Ghana 2011 - Bit24Document2 pagesMICS Ghana 2011 - Bit24BobPas encore d'évaluation
- Bio IADocument9 pagesBio IAJuan VillanuevaPas encore d'évaluation
- 532 East African Medical Journal: October 2003Document8 pages532 East African Medical Journal: October 2003Madhusudhana MvPas encore d'évaluation
- Africa - AllergiesDocument22 pagesAfrica - AllergiescafffyPas encore d'évaluation
- 2.0 ECONOMIC ANALYSIS OF COWPEA PRODUCTION (Autosaved) V2Document15 pages2.0 ECONOMIC ANALYSIS OF COWPEA PRODUCTION (Autosaved) V2official adePas encore d'évaluation
- Soil Analysis: Agsource Harris LaboratoriesDocument3 pagesSoil Analysis: Agsource Harris Laboratoriesb0taxPas encore d'évaluation
- Salt Reduction Programme - Ireland 2003-2011Document13 pagesSalt Reduction Programme - Ireland 2003-2011api-589048135Pas encore d'évaluation
- Accepted Manuscript: Food ChemistryDocument34 pagesAccepted Manuscript: Food ChemistryTâm Dương ĐứcPas encore d'évaluation
- 7368-Article Text-6932-1-10-20170216Document6 pages7368-Article Text-6932-1-10-20170216Alyxzir King ManguladPas encore d'évaluation
- Salt SurveyDocument46 pagesSalt SurveyRodrigo Uribe BravoPas encore d'évaluation
- Sauerkraut and Sauerkraut Juice Fermented Spontaneously Using Mineral Salt, Garlic and AlgaeDocument7 pagesSauerkraut and Sauerkraut Juice Fermented Spontaneously Using Mineral Salt, Garlic and Algaepawoe3064Pas encore d'évaluation
- YounJ WB1-2Document44 pagesYounJ WB1-2MindyJ.YounPas encore d'évaluation
- Biochemistry AnalyzerDocument23 pagesBiochemistry AnalyzerBunga ExsotikaPas encore d'évaluation
- Health Situational AnalysisDocument70 pagesHealth Situational AnalysisGretchen Mae Corrales100% (1)
- Sarit Polsky, M.D.,: The Influence of Herbs and Spices On Overall Liking of Reduced Fat FoodDocument27 pagesSarit Polsky, M.D.,: The Influence of Herbs and Spices On Overall Liking of Reduced Fat FoodNational Press FoundationPas encore d'évaluation
- Urinalysis ResultsDocument8 pagesUrinalysis ResultssyrerleePas encore d'évaluation
- LWT - Food Science and Technology: A B C D e A A A ADocument8 pagesLWT - Food Science and Technology: A B C D e A A A AUser InvalidPas encore d'évaluation
- The Effect of Salinity On The Growth of Phaseolus VulgarisDocument11 pagesThe Effect of Salinity On The Growth of Phaseolus VulgarisPhilip KaulPas encore d'évaluation
- Nwanguma 2013Document6 pagesNwanguma 2013elhaririolayaPas encore d'évaluation
- This Author's PDF Version Corresponds To The Article As It Appeared Upon Acceptance. Fully Formatted PDF Versions Will Be Made Available SoonDocument18 pagesThis Author's PDF Version Corresponds To The Article As It Appeared Upon Acceptance. Fully Formatted PDF Versions Will Be Made Available SoonmdmkiPas encore d'évaluation
- Total+Allowable+Error+Limits+Table+Example Rev20120725Document4 pagesTotal+Allowable+Error+Limits+Table+Example Rev20120725Meidina Siti HanifahPas encore d'évaluation
- Abdurrauf YahayaDocument10 pagesAbdurrauf YahayaJafar NuradeenPas encore d'évaluation
- tmp3AD0 TMPDocument4 pagestmp3AD0 TMPFrontiersPas encore d'évaluation
- Analysis SaltDocument40 pagesAnalysis SaltvsnaveenkPas encore d'évaluation
- Rapid Determination of Calcium in FeedstuffsDocument2 pagesRapid Determination of Calcium in FeedstuffsPhan Vinh ThinhPas encore d'évaluation
- Meat Science: A A A B A ADocument11 pagesMeat Science: A A A B A APedro MedinaPas encore d'évaluation
- IEC Organic Agriculture PPT (Compatibility Mode)Document24 pagesIEC Organic Agriculture PPT (Compatibility Mode)Arya UpadhyayaPas encore d'évaluation
- Influence of Different Levels of Sodium Chloride and of A Reduced-Sodium Salt Substitute On Volatiles Formation and Sdsensory Quality of Wheat BreadDocument9 pagesInfluence of Different Levels of Sodium Chloride and of A Reduced-Sodium Salt Substitute On Volatiles Formation and Sdsensory Quality of Wheat BreadKevin MesaPas encore d'évaluation
- 72952-Article Text-160262-1-10-20120109Document12 pages72952-Article Text-160262-1-10-20120109Anchang Don MaximPas encore d'évaluation
- NguyenH WB5Document42 pagesNguyenH WB5hnguyen92Pas encore d'évaluation
- Journal IMJ Roro Nur Fauziyah, Nabila Putri Amelia Dkk. Poltekeks Bandung, Indonesia PDFDocument11 pagesJournal IMJ Roro Nur Fauziyah, Nabila Putri Amelia Dkk. Poltekeks Bandung, Indonesia PDFSophia PujiartiPas encore d'évaluation
- Lab SauerkrautDocument6 pagesLab SauerkrautSikin Sikin100% (2)
- Indonesia: Vitamin and Mineral Nutrition Information System (VMNIS)Document11 pagesIndonesia: Vitamin and Mineral Nutrition Information System (VMNIS)mum-mpiiPas encore d'évaluation
- English FAL P1 Nov 2016Document13 pagesEnglish FAL P1 Nov 2016lulamamhlangu4Pas encore d'évaluation
- BecerrilA WB1Document39 pagesBecerrilA WB1Cruz RogersPas encore d'évaluation
- Chemistry ProjectDocument5 pagesChemistry ProjectAnukruti SawalaPas encore d'évaluation
- Journal Seasoning Fyp Nur Atikah Binti Zulkifle 3.5.23Document13 pagesJournal Seasoning Fyp Nur Atikah Binti Zulkifle 3.5.23MANSOOR ABDUL HAMID -Pas encore d'évaluation
- Fermentation Lab ReportDocument8 pagesFermentation Lab ReportJoel ComanPas encore d'évaluation
- Fertilizing AlfalfaDocument42 pagesFertilizing AlfalfaskoricmilanPas encore d'évaluation
- Week3-Physical Examination of UrineDocument24 pagesWeek3-Physical Examination of UrineDayledaniel SorvetoPas encore d'évaluation
- Review Jurnal Kadar Air Pada Sosis Daging Sapi Kelompok 3 Prak Wastu-1Document27 pagesReview Jurnal Kadar Air Pada Sosis Daging Sapi Kelompok 3 Prak Wastu-1farida zaenur yaniPas encore d'évaluation
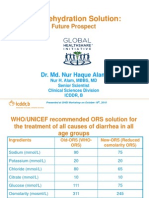
- Oral Rehydration Solution:: Future ProspectDocument48 pagesOral Rehydration Solution:: Future ProspectmustikaarumPas encore d'évaluation
- Sweet Potatoes SandovalD F2TDocument12 pagesSweet Potatoes SandovalD F2Tjacksand75Pas encore d'évaluation
- Natural Occurrence of Aflatoxins in Commercial Pepper in IranDocument8 pagesNatural Occurrence of Aflatoxins in Commercial Pepper in IranNehmyaPas encore d'évaluation
- Bala PresentationDocument72 pagesBala PresentationRajesh BhushanPas encore d'évaluation
- Ukweli Project UTI Test Strip: Elevated PH TestDocument8 pagesUkweli Project UTI Test Strip: Elevated PH Testapi-284496286Pas encore d'évaluation
- Blue Illustrative Science Project Cover Document A4Document22 pagesBlue Illustrative Science Project Cover Document A4abhimanyurv09Pas encore d'évaluation
- Analisa Makanan BayiDocument6 pagesAnalisa Makanan BayiAmanda Putri GitaPas encore d'évaluation
- Glycemic IndexDocument34 pagesGlycemic IndexGaneshPas encore d'évaluation
- Determination of Pepsin Digestability in Fish Meal 2000-1 PDFDocument26 pagesDetermination of Pepsin Digestability in Fish Meal 2000-1 PDFTuấn Anh LêPas encore d'évaluation
- C993 03 PDFDocument7 pagesC993 03 PDFdanzan1Pas encore d'évaluation
- HPLC Analysis of Organic Acids in Lactic Acid Fermented VegetablesDocument4 pagesHPLC Analysis of Organic Acids in Lactic Acid Fermented VegetablesKees VisserPas encore d'évaluation
- Conroy2019 KornetDocument10 pagesConroy2019 KornetyooNa. hmdPas encore d'évaluation
- PMNQ WQ Standard 2Document34 pagesPMNQ WQ Standard 2PatrickDizonPas encore d'évaluation
- Zhang 2008Document6 pagesZhang 2008Siska khoirunnisaPas encore d'évaluation
- Crude Fat, Hexanes Extraction, in Feed, Cereal Grain, and Forage (Randall/Soxtec/Submersion Method) : Collaborative StudyDocument10 pagesCrude Fat, Hexanes Extraction, in Feed, Cereal Grain, and Forage (Randall/Soxtec/Submersion Method) : Collaborative StudyIshtiaque IshtiPas encore d'évaluation
- Lecture 17-Hypertension-19Document23 pagesLecture 17-Hypertension-19Muhammad NuraPas encore d'évaluation
- Electric Pressure Cooker + Dash Diet: 100 Easy Recipes for Healthy Eating, Healthy Living & Weight LossD'EverandElectric Pressure Cooker + Dash Diet: 100 Easy Recipes for Healthy Eating, Healthy Living & Weight LossPas encore d'évaluation
- Electric Pressure Cooker & Crockpot: 100 Easy Recipes for Healthy Eating, Healthy Living, & Weight LossD'EverandElectric Pressure Cooker & Crockpot: 100 Easy Recipes for Healthy Eating, Healthy Living, & Weight LossPas encore d'évaluation
- Complementary and Alternative Medical Lab Testing Part 19: MiscellaneousD'EverandComplementary and Alternative Medical Lab Testing Part 19: MiscellaneousPas encore d'évaluation
- 2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part7Document1 page2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part7BobPas encore d'évaluation
- 2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part11Document1 page2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part11BobPas encore d'évaluation
- 2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part10Document1 page2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part10BobPas encore d'évaluation
- 2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part9Document1 page2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part9BobPas encore d'évaluation
- 2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part5Document1 page2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part5BobPas encore d'évaluation
- 2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part4Document1 page2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part4BobPas encore d'évaluation
- 2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part6Document1 page2010 - Patouillard - MJ - Retail Sector Distribution Chains - Part6BobPas encore d'évaluation
- MICS Ghana 2011 - Bit21Document2 pagesMICS Ghana 2011 - Bit21BobPas encore d'évaluation
- MICS Ghana 2011 - Bit22Document2 pagesMICS Ghana 2011 - Bit22BobPas encore d'évaluation
- MICS Ghana 2011 - Bit20Document2 pagesMICS Ghana 2011 - Bit20BobPas encore d'évaluation
- Peebles Baptist Church Magazine - April 2013Document24 pagesPeebles Baptist Church Magazine - April 2013Ian K. GrayPas encore d'évaluation
- Bswe 002Document5 pagesBswe 002Melwin DsouzaPas encore d'évaluation
- DSWD 4PsDocument3 pagesDSWD 4PsHannaPas encore d'évaluation
- Research Proposal On Sustainable ConsumptionDocument12 pagesResearch Proposal On Sustainable ConsumptionSaadgi AgarwalPas encore d'évaluation
- Maths Quesiton Bank - Class 12Document49 pagesMaths Quesiton Bank - Class 12woooa maliniPas encore d'évaluation
- Poverty in The PhilippinesDocument1 pagePoverty in The PhilippinesArianne Jane C. RodriguezPas encore d'évaluation
- National Strategy For The Neighbourhood Renewal: A Framework For ConsultationDocument21 pagesNational Strategy For The Neighbourhood Renewal: A Framework For ConsultationOxfamPas encore d'évaluation
- The Impact of Liberalisation and Privatisation in India Economy SeminarDocument5 pagesThe Impact of Liberalisation and Privatisation in India Economy SeminargoforjessicaPas encore d'évaluation
- Dimension of Rural Development in NepalDocument6 pagesDimension of Rural Development in NepalJay KhadkaPas encore d'évaluation
- CBMS PDFDocument20 pagesCBMS PDFjoecath2013Pas encore d'évaluation
- Durham (1995) Soliciting Gifts and Negotiating AgencyDocument19 pagesDurham (1995) Soliciting Gifts and Negotiating AgencytofaniskoPas encore d'évaluation
- My Year of No Spending (Advanced)Document5 pagesMy Year of No Spending (Advanced)Phung Thanh Thom100% (2)
- Ngonedo Strategic Plan 2008 - 2011Document36 pagesNgonedo Strategic Plan 2008 - 2011EdwardMbogoPas encore d'évaluation
- World Trade OrganizationDocument7 pagesWorld Trade OrganizationBorof TuhinPas encore d'évaluation
- Sociological Perspectives On Poverty: Key PointsDocument4 pagesSociological Perspectives On Poverty: Key PointsdwanePas encore d'évaluation
- Reviewer Business EthicsDocument6 pagesReviewer Business EthicsJean Rose IglesiasPas encore d'évaluation
- 30618062Document405 pages30618062ghjuthrgefegthyjugtrdePas encore d'évaluation
- Approved Specialization 1 - Pamayanang MaliksiDocument26 pagesApproved Specialization 1 - Pamayanang MaliksiNowitzkiTramonto100% (5)
- Public Art Fee Files PDFDocument23 pagesPublic Art Fee Files PDFRecordTrac - City of OaklandPas encore d'évaluation
- 07 Health Psycology-Prevention of Dease and Illness PDFDocument12 pages07 Health Psycology-Prevention of Dease and Illness PDFlebssbel1Pas encore d'évaluation
- Teaching With Poverty MindDocument3 pagesTeaching With Poverty MindJDValencia Piano100% (1)
- Veteran Build Brochure - Anas EditDocument2 pagesVeteran Build Brochure - Anas Editapi-325745351Pas encore d'évaluation
- FA3 QuizonDocument2 pagesFA3 QuizonHugh BenchPas encore d'évaluation
- BBBBBBBBBDocument33 pagesBBBBBBBBBTesfaye GemechuPas encore d'évaluation
- PET Buster Test 2Document2 pagesPET Buster Test 2Aleksandra Pavlovska100% (1)
- The Prince and Hitler's WinterhilfswerkDocument9 pagesThe Prince and Hitler's WinterhilfswerkJACK-LAMEDPas encore d'évaluation
- Essays of RizalDocument13 pagesEssays of RizalRanger Rodz Tennyson100% (1)
- 21 Century Literature From The Philippines and The WorldDocument21 pages21 Century Literature From The Philippines and The Worldwendell john medianaPas encore d'évaluation
- Moral Issues in Globalization PDFDocument39 pagesMoral Issues in Globalization PDFAriadnaNatyPas encore d'évaluation
- 2003 Family Income Expenditure SurveyDocument112 pages2003 Family Income Expenditure SurveyJoseph SalazarPas encore d'évaluation