Vous aimerez peut-être aussi
- Anesthesia For The Patient With Peripartum Hemorrhage - UpToDateDocument25 pagesAnesthesia For The Patient With Peripartum Hemorrhage - UpToDateZurya UdayanaPas encore d'évaluation
- Vaishali Syal Moderator - Prof. J. R. ThakurDocument34 pagesVaishali Syal Moderator - Prof. J. R. ThakurTasha NurfitrianiPas encore d'évaluation
- AA Course-Difficult Airway1Document54 pagesAA Course-Difficult Airway1Anonymous V5xDcrPas encore d'évaluation
- Preoxygenation During Induction of Anesthesia in Noncritically Ill PatientsDocument6 pagesPreoxygenation During Induction of Anesthesia in Noncritically Ill PatientsasfwegerePas encore d'évaluation
- Anesthesia For ElderlyDocument27 pagesAnesthesia For ElderlyApril Joy CalayagPas encore d'évaluation
- Geriartry and AnethesiaDocument5 pagesGeriartry and AnethesiaDavidVictoriousLukasPas encore d'évaluation
- Anesthesia For Patients With Thyroid Disease - UpToDateDocument12 pagesAnesthesia For Patients With Thyroid Disease - UpToDateJavier GlezqPas encore d'évaluation
- Anesthesia For The Patient With Preeclampsia - UpToDateDocument31 pagesAnesthesia For The Patient With Preeclampsia - UpToDateJazivi AlejoPas encore d'évaluation
- Anesthesia For Geriatric PatientsDocument45 pagesAnesthesia For Geriatric PatientsIDI Bangka BaratPas encore d'évaluation
- Anesthesia PresentationDocument19 pagesAnesthesia PresentationJohnyPas encore d'évaluation
- 1095 Preoperative Risk Stratification and OptimizationDocument99 pages1095 Preoperative Risk Stratification and OptimizationHening Tirta KusumawardaniPas encore d'évaluation
- Liver Disease in AnesthesiaDocument31 pagesLiver Disease in AnesthesiaAnnan Agyekum JoshuaPas encore d'évaluation
- 2022 Preoperative Assessment Premedication Perioperative DocumentationDocument38 pages2022 Preoperative Assessment Premedication Perioperative DocumentationMohmmed Mousa100% (1)
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguPas encore d'évaluation
- Neuraxial AnesthesiaDocument26 pagesNeuraxial AnesthesiaAyen FornollesPas encore d'évaluation
- Post Op DeliriumDocument26 pagesPost Op DeliriumKannan GPas encore d'évaluation
- Intraoperative Fluid ManagementDocument15 pagesIntraoperative Fluid ManagementMirela Marina BlajPas encore d'évaluation
- Thoraxic Region Nerve Block - ESADocument35 pagesThoraxic Region Nerve Block - ESAMaraPas encore d'évaluation
- Pre Op 2010Document37 pagesPre Op 2010Tawona DhlakamaPas encore d'évaluation
- Monitoring in AnesthesiaDocument69 pagesMonitoring in AnesthesiaGiridhar GrishPas encore d'évaluation
- Bariatric SurgeryDocument37 pagesBariatric SurgerySandeep YendamuriPas encore d'évaluation
- DR Lila - Patient Preparation For Emergencies Surgeries - New 11012017Document37 pagesDR Lila - Patient Preparation For Emergencies Surgeries - New 11012017bloadyroar100% (1)
- 1.05 (Surgery) General Anesthesia - Airway ManagementDocument3 pages1.05 (Surgery) General Anesthesia - Airway ManagementLeo Mari Go LimPas encore d'évaluation
- Epidural Anatomy & PhysiologyDocument14 pagesEpidural Anatomy & PhysiologyAbel AxelPas encore d'évaluation
- Intravenous Anesthetic Agents: by Miss Maidah MehtabDocument49 pagesIntravenous Anesthetic Agents: by Miss Maidah MehtabLuqman QadirPas encore d'évaluation
- Enhanced Recovery After Surgery (ERAS) in Emergency Abdominal Surgery: Background, Preoperative Components of ERAS, Intraoperative Components of ERASDocument9 pagesEnhanced Recovery After Surgery (ERAS) in Emergency Abdominal Surgery: Background, Preoperative Components of ERAS, Intraoperative Components of ERASAndre F SusantioPas encore d'évaluation
- General Anesthetics: General Anesthesia - Characteristics Balanced AnesthesiaDocument7 pagesGeneral Anesthetics: General Anesthesia - Characteristics Balanced AnesthesiarisanataliasiburianPas encore d'évaluation
- Medication Administration PolicyDocument188 pagesMedication Administration Policyليراث ليPas encore d'évaluation
- Neonatal AnaesthesiaDocument30 pagesNeonatal Anaesthesiavenkatesh chowdaryPas encore d'évaluation
- Monitored Anesthesia Care in Adults: Considerations During Covid-19 PandemicDocument29 pagesMonitored Anesthesia Care in Adults: Considerations During Covid-19 PandemicGanda Impola TBAPas encore d'évaluation
- Preanesthetic Medication JasminaDocument44 pagesPreanesthetic Medication Jasminaanjali sPas encore d'évaluation
- Anaesthesia For Thyroid Surgery....Document46 pagesAnaesthesia For Thyroid Surgery....Parvathy R NairPas encore d'évaluation
- Regional AnesthesiaDocument209 pagesRegional AnesthesiaNatnael ZelalemPas encore d'évaluation
- Rapid Seq InductionDocument6 pagesRapid Seq InductionandikszuhriPas encore d'évaluation
- Elia Jennifer Perioperative Fluid Management andDocument19 pagesElia Jennifer Perioperative Fluid Management andSiddhartha PalaciosPas encore d'évaluation
- Anesthesia Considerations For Neuromuscular DiseaseDocument42 pagesAnesthesia Considerations For Neuromuscular Diseasesamrox54Pas encore d'évaluation
- Management of Intraoperative Bronchospasm: Dr. ImranDocument49 pagesManagement of Intraoperative Bronchospasm: Dr. ImranhellodrvigneshwarPas encore d'évaluation
- Patient Monitoring1370Document53 pagesPatient Monitoring1370Ridha Surya NugrahaPas encore d'évaluation
- Enhanced Recovery After Surgery: Nutrition Issues in Gastroenterology, Series #151Document15 pagesEnhanced Recovery After Surgery: Nutrition Issues in Gastroenterology, Series #151Hendry DimasPas encore d'évaluation
- Anaesthesia For Neuroradiological Procedures Premalatha SDocument48 pagesAnaesthesia For Neuroradiological Procedures Premalatha SPrema LathaPas encore d'évaluation
- Anasthesia in Obese PatientDocument4 pagesAnasthesia in Obese PatientWaNda GrPas encore d'évaluation
- AntidotesDocument36 pagesAntidotesMohamed Haggag100% (1)
- Spinal Anaesthesia A Practical GuideDocument14 pagesSpinal Anaesthesia A Practical GuideNovita WulandariPas encore d'évaluation
- Anesthesia For Genitourinary SurgeryDocument76 pagesAnesthesia For Genitourinary SurgeryWenny Eka FildayantiPas encore d'évaluation
- IV Induction Agents UMAIDDocument63 pagesIV Induction Agents UMAIDUmaid Mirza100% (1)
- Bronchial AsthmaDocument25 pagesBronchial AsthmaKamil HannaPas encore d'évaluation
- TIVA - Copy (2) - Copy-1Document34 pagesTIVA - Copy (2) - Copy-1Keerthikumar Parvatha100% (2)
- Muscle RelaxantsDocument8 pagesMuscle RelaxantsFemi AustinPas encore d'évaluation
- OpioidsDocument16 pagesOpioidsCutie PiePas encore d'évaluation
- Pharmacokinetics of Inhalation AnestheticsDocument24 pagesPharmacokinetics of Inhalation AnestheticsKinanta DewiPas encore d'évaluation
- Anesthesia MachineDocument37 pagesAnesthesia MachineDakshPas encore d'évaluation
- Low Flow Anesthesia-FInalDocument45 pagesLow Flow Anesthesia-FInalYohanes Widjaja100% (1)
- Anaesthesia in Laproscopy SurgeriesDocument39 pagesAnaesthesia in Laproscopy SurgeriesRaguPas encore d'évaluation
- Eras Bps Final Nov2017 2Document24 pagesEras Bps Final Nov2017 2Wardah Fauziah El SofwanPas encore d'évaluation
- TivaDocument38 pagesTivasunny kumar100% (1)
- IV Anesthetic AgentsDocument72 pagesIV Anesthetic AgentsRaghavendra PrasadPas encore d'évaluation
- PreoperativeDocument34 pagesPreoperativeTasha NurfitrianiPas encore d'évaluation
- Airway Pharmacology: Anesthesia KeyDocument19 pagesAirway Pharmacology: Anesthesia KeyChrispin FaithPas encore d'évaluation
- Pediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderD'EverandPediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderPas encore d'évaluation
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingD'EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováPas encore d'évaluation
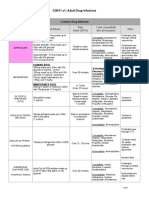
- CG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtherDocument8 pagesCG011.v1: Adult Drug Infusions: Drug Dose and Diluent Rate (Note UNITS) Y Site Compatibility (Not All-Inclusive) OtheriqbalPas encore d'évaluation
- Skor CHIPPSDocument11 pagesSkor CHIPPSSuryanti SultanPas encore d'évaluation
- ATI Flash Cards 05, Medications Affecting The Nervous SystemDocument110 pagesATI Flash Cards 05, Medications Affecting The Nervous SystemGiovanni MictilPas encore d'évaluation
- Acta Anaesthesiol Scand - 2021 - Dokken - Iatrogenic Withdrawal Syndrome Frequently Occurs in Paediatric Intensive CareDocument8 pagesActa Anaesthesiol Scand - 2021 - Dokken - Iatrogenic Withdrawal Syndrome Frequently Occurs in Paediatric Intensive Carefuka priesleyPas encore d'évaluation
- Comparison of Propofol CRI and Isoflurane Speke Gazelle 2017Document11 pagesComparison of Propofol CRI and Isoflurane Speke Gazelle 2017Tareas GalileoPas encore d'évaluation
- Acta Anaesthesiol Scand 2015 PasinDocument8 pagesActa Anaesthesiol Scand 2015 PasinLuis CordovaPas encore d'évaluation
- Tiva en NiñosDocument22 pagesTiva en NiñosAndre EstupiñanPas encore d'évaluation
- HELDMANN 1999 The Association of Propofol Usage With Posoperatve Wound Infection Rate in Clean Wounds PDFDocument4 pagesHELDMANN 1999 The Association of Propofol Usage With Posoperatve Wound Infection Rate in Clean Wounds PDFAntonio PG´sPas encore d'évaluation
- Sedatives in Neurocritical Care 2019 Curr Opin Crit CareDocument8 pagesSedatives in Neurocritical Care 2019 Curr Opin Crit CareCAMILO ERNESTO DAZA PERDOMOPas encore d'évaluation
- PIIS2058534920300202Document7 pagesPIIS2058534920300202Dwi WahyudiPas encore d'évaluation
- General Anesthesia: Outline of LectureDocument37 pagesGeneral Anesthesia: Outline of LectureScribDPas encore d'évaluation
- Drug Study (Anesthesia)Document4 pagesDrug Study (Anesthesia)Jane Arian Berzabal100% (4)
- Critical Care CasesDocument7 pagesCritical Care CasesJude Micko Bunyi AlipitPas encore d'évaluation
- Ebp - Best Practice For Sedation Protocol in Icu PatientsDocument32 pagesEbp - Best Practice For Sedation Protocol in Icu Patientsapi-435628975Pas encore d'évaluation
- Anaesthesia in Dogs and Cats With Cardiac DiseaseDocument19 pagesAnaesthesia in Dogs and Cats With Cardiac DiseaseALEJANDRA MADRIGALPas encore d'évaluation
- Status AsthmaticusDocument22 pagesStatus AsthmaticusGali Kesuma100% (1)
- GADocument51 pagesGAWasi KhanPas encore d'évaluation
- Anesthetic Management and Deep Sedation After Emergence From General Anesthesia - A Retrospective Cohort StudyDocument10 pagesAnesthetic Management and Deep Sedation After Emergence From General Anesthesia - A Retrospective Cohort Studygwhqvmqks5Pas encore d'évaluation
- Status Epilepticus: by Aaron M. Cook, Pharm.D., BCPS, BCCCPDocument20 pagesStatus Epilepticus: by Aaron M. Cook, Pharm.D., BCPS, BCCCPpuaanPas encore d'évaluation
- Jurnal AnestesiDocument8 pagesJurnal AnestesiFaidh HusnanPas encore d'évaluation
- Rguhs Thesis Topics in AnesthesiaDocument5 pagesRguhs Thesis Topics in AnesthesiaDltkCustomWritingPaperMurfreesboro100% (2)
- Neuromonitoring in Surgery and Anesthesia - UpToDateDocument47 pagesNeuromonitoring in Surgery and Anesthesia - UpToDateAna Belén Artero CastañoPas encore d'évaluation
- Oral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Document13 pagesOral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Max FaxPas encore d'évaluation
- General AnaesthesiaDocument11 pagesGeneral AnaesthesiaFaria Islam JuhiPas encore d'évaluation
- FinalprintedversionDocument9 pagesFinalprintedversionشادي العمرPas encore d'évaluation
- Drug Study (Burn Injury) ManuscriptDocument4 pagesDrug Study (Burn Injury) ManuscriptEricka VillanuevaPas encore d'évaluation
- Case 4 BurnDocument4 pagesCase 4 BurnZahraa farajPas encore d'évaluation
- Anaesthesia For Neurosurgery-PIIS1472029919302656Document6 pagesAnaesthesia For Neurosurgery-PIIS1472029919302656james Wilson09Pas encore d'évaluation
- Propofol Vs Midazolam For ICU SedationDocument9 pagesPropofol Vs Midazolam For ICU SedationLiszt AlcantaraPas encore d'évaluation
- Preanaesthetic Medication Anaesthetic Agents PDFDocument35 pagesPreanaesthetic Medication Anaesthetic Agents PDFSubhash BeraPas encore d'évaluation