Vous aimerez peut-être aussi
- Hypertension Protocol JeannineDocument53 pagesHypertension Protocol JeannineAleile DRPas encore d'évaluation
- Mod 4 Revision Guide 1 Reaction Kinetics AQA A2 ChemistryDocument5 pagesMod 4 Revision Guide 1 Reaction Kinetics AQA A2 Chemistryviyas07Pas encore d'évaluation
- Physician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseDocument9 pagesPhysician Factors Associated With Polypharmacy and Potentially Inappropriate Medication UseratnatriaaPas encore d'évaluation
- Research Paper On PolypharmacyDocument5 pagesResearch Paper On Polypharmacyefj02jba100% (1)
- International Research Journal of PharmacyDocument5 pagesInternational Research Journal of PharmacyKoko DandashPas encore d'évaluation
- Interventions in Nursing HomesDocument18 pagesInterventions in Nursing Homesvictory818Pas encore d'évaluation
- Salud PublicaDocument21 pagesSalud PublicaJorge DiazPas encore d'évaluation
- Potential For Alcohol and Prescription Drug Interactions in Older PeopleDocument7 pagesPotential For Alcohol and Prescription Drug Interactions in Older PeopleEstephane CoelhoPas encore d'évaluation
- Self Medication Study in PunjabDocument4 pagesSelf Medication Study in PunjabAnkeet PatkarPas encore d'évaluation
- Farmacología en AncianosDocument13 pagesFarmacología en AncianosGisselle RodriguezPas encore d'évaluation
- Prevalence of Self-Medication Practices and Its Associated Factors in Rural Bengaluru, Karnataka, IndiaDocument6 pagesPrevalence of Self-Medication Practices and Its Associated Factors in Rural Bengaluru, Karnataka, IndiaVijaya RaniPas encore d'évaluation
- Corresponding AuthorDocument25 pagesCorresponding AuthorSundas EjazPas encore d'évaluation
- Dietary Supplement Users Vary in Attitudes and Sources of Dietary Supplement Information in East and West Geographic Regions: A Cross-Sectional StudyDocument10 pagesDietary Supplement Users Vary in Attitudes and Sources of Dietary Supplement Information in East and West Geographic Regions: A Cross-Sectional StudyfsfPas encore d'évaluation
- 18 Trastorno BipolarDocument9 pages18 Trastorno BipolarDiana Carolina Vasquez CardenasPas encore d'évaluation
- Patients' Perceptions of Drug Therapy Counseling in Israel: Original ArticlesDocument4 pagesPatients' Perceptions of Drug Therapy Counseling in Israel: Original ArticlesMartha OktaviaPas encore d'évaluation
- Añonuevo Matorres Moreno Copernicus Final-Paper-Pr2Document43 pagesAñonuevo Matorres Moreno Copernicus Final-Paper-Pr211SA AÑONUEVO MARJORIE NICOLEPas encore d'évaluation
- The Unsung Role of The Pharmacist in Patient Health: Credit Rich Pedroncelli/Associated PressDocument3 pagesThe Unsung Role of The Pharmacist in Patient Health: Credit Rich Pedroncelli/Associated PressJohnny PaulPas encore d'évaluation
- Literature Review PolypharmacyDocument12 pagesLiterature Review Polypharmacyea8p6td0100% (1)
- 18 Gouri Et AlDocument6 pages18 Gouri Et AleditorijmrhsPas encore d'évaluation
- 2018 Value-in-HeDocument7 pages2018 Value-in-HeArchie CabachetePas encore d'évaluation
- DownloadDocument6 pagesDownloadMr AggarwalPas encore d'évaluation
- Medication Appropriateness IndexDocument12 pagesMedication Appropriateness IndexMarc FosterPas encore d'évaluation
- Relationships Between Beliefs About Medications AnDocument7 pagesRelationships Between Beliefs About Medications Annoor cahayaPas encore d'évaluation
- Potentially Inappropriate Medications Defined by STOPP Criteria and The Risk of Adverse Drug Events in Older Hospitalized Patients FREEDocument14 pagesPotentially Inappropriate Medications Defined by STOPP Criteria and The Risk of Adverse Drug Events in Older Hospitalized Patients FREENurul FitryaniPas encore d'évaluation
- Philippine College of Health Science IncDocument23 pagesPhilippine College of Health Science Incpeter brucePas encore d'évaluation
- Geriatrics: Roger E. ThomasDocument44 pagesGeriatrics: Roger E. ThomasSubhash SharmaPas encore d'évaluation
- 0rder 343 NRS-493-ASSIGNMENT 3 Literature ReviewDocument6 pages0rder 343 NRS-493-ASSIGNMENT 3 Literature Reviewjoshua chegePas encore d'évaluation
- Co-Prescription Trends in A Large Cohort of Subjects Predict Substantial Drug-Drug InteractionsDocument19 pagesCo-Prescription Trends in A Large Cohort of Subjects Predict Substantial Drug-Drug Interactionsadern-07huepfendPas encore d'évaluation
- Potentially Inappropriate Prescribing and Cost Outcomes For Older People: A National Population StudyDocument10 pagesPotentially Inappropriate Prescribing and Cost Outcomes For Older People: A National Population Studybiotech_vidhyaPas encore d'évaluation
- Exploring The Knowledge and Attitude of Medical and Pharmacy Students About Generic Medicine in Lahore, PakistanDocument7 pagesExploring The Knowledge and Attitude of Medical and Pharmacy Students About Generic Medicine in Lahore, PakistanMathilda UllyPas encore d'évaluation
- Jurnal ReadinhDocument7 pagesJurnal ReadinhwindysiPas encore d'évaluation
- Literature Review On PolypharmacyDocument5 pagesLiterature Review On Polypharmacyfuhukuheseg2100% (1)
- GROUP 2 - Written Report - Journal Critique Using PICOTS ToolDocument3 pagesGROUP 2 - Written Report - Journal Critique Using PICOTS ToolMissy NaguitPas encore d'évaluation
- Chakelba 2013Document9 pagesChakelba 2013Nawang WulanPas encore d'évaluation
- Ni Hms 94884Document13 pagesNi Hms 94884Cahya Daris TriwibowoPas encore d'évaluation
- Barnes 2004 Complementary UseDocument18 pagesBarnes 2004 Complementary UseAntonio MoreiraPas encore d'évaluation
- 7 Sadiqua EtalDocument6 pages7 Sadiqua EtaleditorijmrhsPas encore d'évaluation
- British Journal of Clinical PharmacologyDocument6 pagesBritish Journal of Clinical PharmacologyJunerey Hume Torres RodriguezPas encore d'évaluation
- Pharmpract 14 740Document7 pagesPharmpract 14 740Hamza DibPas encore d'évaluation
- NIH Public Access: Clinical Consequences of Polypharmacy in ElderlyDocument11 pagesNIH Public Access: Clinical Consequences of Polypharmacy in ElderlyGabo Bravo RodríguezPas encore d'évaluation
- PJMS 34 959Document5 pagesPJMS 34 959Husni FaridPas encore d'évaluation
- Review of Relat WPS OfficeDocument3 pagesReview of Relat WPS OfficeArdiene Shallouvette GamosoPas encore d'évaluation
- Antipsychotic Long Acting InjectionsDocument7 pagesAntipsychotic Long Acting InjectionsVoNda AprilianiPas encore d'évaluation
- Jazul Lang MalakasDocument5 pagesJazul Lang MalakasDarl VelardePas encore d'évaluation
- KetorolacDocument16 pagesKetorolacniken retnoPas encore d'évaluation
- Prescribing Patterns of Drugs in Outpatient Department of Paediatrics in Tertiary Care HospitalDocument12 pagesPrescribing Patterns of Drugs in Outpatient Department of Paediatrics in Tertiary Care HospitalAleena Maria KurisinkalPas encore d'évaluation
- Running Head: Healthcare Policy Concern 1Document8 pagesRunning Head: Healthcare Policy Concern 1Nasir HussainPas encore d'évaluation
- Terms Used in Patient Safety Related To Medication A Literature ReviewDocument5 pagesTerms Used in Patient Safety Related To Medication A Literature ReviewckkuzaxgfPas encore d'évaluation
- Staff Perceptions of Substance Use Among Acute Psychiatry In-PatientsDocument6 pagesStaff Perceptions of Substance Use Among Acute Psychiatry In-PatientsPaula StroianPas encore d'évaluation
- 673 FullDocument7 pages673 FullAq IfahPas encore d'évaluation
- The KIDs ListDocument17 pagesThe KIDs ListSantiago MerloPas encore d'évaluation
- Improving Primary Care in Rural Alabama With A Pharmacy InitiativeDocument7 pagesImproving Primary Care in Rural Alabama With A Pharmacy InitiativeBasilharbi HammadPas encore d'évaluation
- How Much Do Elders With Chronic Conditions Know About Their Medications?Document7 pagesHow Much Do Elders With Chronic Conditions Know About Their Medications?Sundas EjazPas encore d'évaluation
- Bpac Polypharmacy Poem 2006 PFDocument20 pagesBpac Polypharmacy Poem 2006 PFJacob Alexander MarpaungPas encore d'évaluation
- Medicacion InapropiadaDocument22 pagesMedicacion Inapropiadaagu oliveroPas encore d'évaluation
- 1268 PDFDocument5 pages1268 PDFCMargs ConceptsPas encore d'évaluation
- Alalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Document4 pagesAlalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Basema HashhashPas encore d'évaluation
- Med ExpertsDocument39 pagesMed ExpertsPH Ph GnsoPas encore d'évaluation
- Chapter - 2 Rational Drug Use: Health Administrator Vol: XIX Number 1: 5-7Document3 pagesChapter - 2 Rational Drug Use: Health Administrator Vol: XIX Number 1: 5-7mayapuspitasariunsriPas encore d'évaluation
- Cannabis For Symptom Management in Older Adults - 2020Document19 pagesCannabis For Symptom Management in Older Adults - 2020Carlos Ferrete JuniorPas encore d'évaluation
- Analytical Chemistry for Assessing Medication AdherenceD'EverandAnalytical Chemistry for Assessing Medication AdherencePas encore d'évaluation
- Allen Cognitive Level Testreport 1Document27 pagesAllen Cognitive Level Testreport 1Kimmy ChuPas encore d'évaluation
- Chronometry of Mentally Versus Physically Practiced Tasks in People With StrokeDocument6 pagesChronometry of Mentally Versus Physically Practiced Tasks in People With StrokeKimmy ChuPas encore d'évaluation
- Description of Dementia Caregiver Uplifts and Implications For Occupational TherapyDocument6 pagesDescription of Dementia Caregiver Uplifts and Implications For Occupational TherapyKimmy ChuPas encore d'évaluation
- Drivers With Dementia and Outcomes of Becoming Lost While DrivingDocument8 pagesDrivers With Dementia and Outcomes of Becoming Lost While DrivingKimmy ChuPas encore d'évaluation
- Effectiveness of Therapy Ball Chairs On Classroom Participation in Children With Autism Spectrum DisordersDocument9 pagesEffectiveness of Therapy Ball Chairs On Classroom Participation in Children With Autism Spectrum DisordersKimmy ChuPas encore d'évaluation
- Functional Performance Characteristics Associated With Postponing Elementary School Entry Among Children With Down SyndromeDocument7 pagesFunctional Performance Characteristics Associated With Postponing Elementary School Entry Among Children With Down SyndromeKimmy ChuPas encore d'évaluation
- Neurocognitive Habilitation Therapy For Children With Fetal Alcohol Spectrum Disorders: An Adaptation of The Alert ProgramDocument11 pagesNeurocognitive Habilitation Therapy For Children With Fetal Alcohol Spectrum Disorders: An Adaptation of The Alert ProgramKimmy ChuPas encore d'évaluation
- Optical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andDocument19 pagesOptical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andCarl SoriaPas encore d'évaluation
- Real Time Operating SystemsDocument15 pagesReal Time Operating SystemsSaro VrsPas encore d'évaluation
- Task 4 Finite Element MethodDocument7 pagesTask 4 Finite Element MethodMohd Azizee Bin SukorPas encore d'évaluation
- Full U-Band Rectangular Waveguide-to-Microstrip Transition Using E-Plane ProbeDocument4 pagesFull U-Band Rectangular Waveguide-to-Microstrip Transition Using E-Plane ProbeSanjib MandalPas encore d'évaluation
- CATIA COMPOSER SYNC2 FLYER 2014 Draft2Document2 pagesCATIA COMPOSER SYNC2 FLYER 2014 Draft2타키비Pas encore d'évaluation
- OVA37066E: Product Data SheetDocument2 pagesOVA37066E: Product Data SheetFred BionPas encore d'évaluation
- PC - Section 1.3 - Worksheet PDFDocument2 pagesPC - Section 1.3 - Worksheet PDFAnabbPas encore d'évaluation
- Biomechanics of The KneeDocument8 pagesBiomechanics of The KneeJorge LopezPas encore d'évaluation
- Bobrick 2021 Class. Quantum Grav. 38 105009Document23 pagesBobrick 2021 Class. Quantum Grav. 38 105009MaxPas encore d'évaluation
- Psychometric Development and Validation of GaslightingDocument15 pagesPsychometric Development and Validation of GaslightingYang ZhangPas encore d'évaluation
- Strain STREMADocument6 pagesStrain STREMAChavin StormPas encore d'évaluation
- UMTS Optimization GuidelineDocument84 pagesUMTS Optimization GuidelineEvelio Sotolongo100% (3)
- Lecture 5Document35 pagesLecture 5MAHAMA SADIKPas encore d'évaluation
- DS1103 Datasheet PDFDocument6 pagesDS1103 Datasheet PDFRosario RiveraPas encore d'évaluation
- Hydrocarbon RecoveryDocument29 pagesHydrocarbon RecoveryAlekhya BandaruPas encore d'évaluation
- Computer Dictionary PDFDocument95 pagesComputer Dictionary PDFMarjenneilPas encore d'évaluation
- OODBMSDocument19 pagesOODBMSashimsarkar2006Pas encore d'évaluation
- Semi Conductors: The Start of Information AgeDocument15 pagesSemi Conductors: The Start of Information AgeMarvin LabajoPas encore d'évaluation
- Hot and Cold ApplicDocument33 pagesHot and Cold Appliccamille_12_15100% (1)
- An FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure CommunicationsDocument5 pagesAn FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure Communicationslaz_chikhi1574Pas encore d'évaluation
- Photo Luminescence of Surfaces and InterfacesDocument25 pagesPhoto Luminescence of Surfaces and InterfacesNick KellerPas encore d'évaluation
- Circuit Protective Devices: Learner Work BookDocument41 pagesCircuit Protective Devices: Learner Work BookChanel Maglinao80% (5)
- XG5000 Manual (2009.10.26) (Eng)Document645 pagesXG5000 Manual (2009.10.26) (Eng)wanderly_40100% (1)
- JPSP - 2022 - 698Document10 pagesJPSP - 2022 - 698hifeztobgglPas encore d'évaluation
- Ruby On Rails 3 Cheat SheetDocument7 pagesRuby On Rails 3 Cheat SheetJarosław MedwidPas encore d'évaluation
- ImmunologyDocument8 pagesImmunologyማላያላም ማላያላም89% (9)
- Dbms-Lab Assignment - 1: Name - VIKAS SINGH Roll No - 4257Document3 pagesDbms-Lab Assignment - 1: Name - VIKAS SINGH Roll No - 4257Vikas SinghPas encore d'évaluation
- Code of Practice For Selection, Laying of Moist Fuel Gas Lines IPSS:1-06-014-17Document11 pagesCode of Practice For Selection, Laying of Moist Fuel Gas Lines IPSS:1-06-014-17Sarbendu PaulPas encore d'évaluation
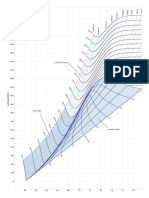
- Mollier Enthalpy Entropy Chart For Steam - US UnitsDocument1 pageMollier Enthalpy Entropy Chart For Steam - US Unitslin tongPas encore d'évaluation