Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- NCP 106Document8 pagesNCP 106yer tagalajPas encore d'évaluation
- Community Acquired Pneumonia, A Case StudyDocument26 pagesCommunity Acquired Pneumonia, A Case StudyMenggay SanDiego57% (7)
- Hesi Study GuideDocument16 pagesHesi Study Guideangie10231100% (3)
- Cameron 2016Document11 pagesCameron 2016CarmePonsPas encore d'évaluation
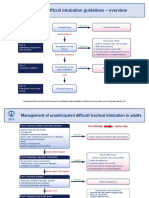
- Difficult Intubation Guidelines OverviewDocument3 pagesDifficult Intubation Guidelines OverviewMaufer AlPas encore d'évaluation
- q1 Social CRMDocument17 pagesq1 Social CRMcésar_campos_45Pas encore d'évaluation
- Poku2016 Q1Document4 pagesPoku2016 Q1césar_campos_45Pas encore d'évaluation
- Gru Now 2013Document18 pagesGru Now 2013césar_campos_45Pas encore d'évaluation
- Aga en Uci 2015Document5 pagesAga en Uci 2015césar_campos_45Pas encore d'évaluation
- VM Prolongada JCC 2015Document7 pagesVM Prolongada JCC 2015césar_campos_45Pas encore d'évaluation
- Insulinoterapia JCC 2015Document6 pagesInsulinoterapia JCC 2015césar_campos_45Pas encore d'évaluation
- VM Seleccionando El Peep Correcto Cocc 2015Document8 pagesVM Seleccionando El Peep Correcto Cocc 2015césar_campos_45Pas encore d'évaluation
- Prognosis GuidelinesDocument103 pagesPrognosis GuidelinesPaola MedinaPas encore d'évaluation
- Hipercapnia, Relevancia Clinica y Mecanismos Cocc 2015Document6 pagesHipercapnia, Relevancia Clinica y Mecanismos Cocc 2015césar_campos_45Pas encore d'évaluation
- Aki Inducida Por Sepsis Cocc 2014Document8 pagesAki Inducida Por Sepsis Cocc 2014césar_campos_45Pas encore d'évaluation
- Vili Cocc 2015Document6 pagesVili Cocc 2015césar_campos_45Pas encore d'évaluation
- Dar o No Dar Fluidos 2012Document8 pagesDar o No Dar Fluidos 2012césar_campos_45Pas encore d'évaluation
- ViliDocument7 pagesVilicésar_campos_45Pas encore d'évaluation
- (Inglés) Guía Infusión Insulina para Manejo Hiperglicemia Pctes Críticos (2012)Document26 pages(Inglés) Guía Infusión Insulina para Manejo Hiperglicemia Pctes Críticos (2012)césar_campos_45Pas encore d'évaluation
- ARDS New Definition - Berlin ConsensusDocument8 pagesARDS New Definition - Berlin ConsensusAndreas IoannouPas encore d'évaluation
- Problems of The Neonate Low Birth Weight BabiesDocument25 pagesProblems of The Neonate Low Birth Weight BabiesmelbourneichrcPas encore d'évaluation
- Case Study of PneumoniaDocument8 pagesCase Study of PneumoniaAnne SedanzaPas encore d'évaluation
- MODULE L3A1 - Sample Weekly Home Learning Plans - MANDIA - TEAM DENNISDocument31 pagesMODULE L3A1 - Sample Weekly Home Learning Plans - MANDIA - TEAM DENNISBernardo Jose MandiaPas encore d'évaluation
- Mojoli 2023 Tidal Lung Hysteresis To Interpret PEEP-induced Changes in Compliance in ARDS PatientsDocument10 pagesMojoli 2023 Tidal Lung Hysteresis To Interpret PEEP-induced Changes in Compliance in ARDS PatientsKhanh Ha NguyenPas encore d'évaluation
- Respiration - Behavior of GasesDocument25 pagesRespiration - Behavior of GasesSodeinde SimeonPas encore d'évaluation
- Mechanical Ventilator Management ProtocolDocument3 pagesMechanical Ventilator Management ProtocolRick Frea100% (2)
- Foreign BodyDocument11 pagesForeign BodyVania Dwi AndhaniPas encore d'évaluation
- Mechanical Ventilation:: 2. Positive Pressure VentilatorDocument3 pagesMechanical Ventilation:: 2. Positive Pressure VentilatorMurad KhairoPas encore d'évaluation
- Acute Respiratory Distress SyndromeDocument2 pagesAcute Respiratory Distress SyndromemaraPas encore d'évaluation
- Practical 4 AssignmentDocument21 pagesPractical 4 AssignmentJamalulhaslina Binti FuadPas encore d'évaluation
- Acute Respiratory InfectionsDocument34 pagesAcute Respiratory InfectionssafiebuttPas encore d'évaluation
- Form 3 Chapter 1 QuestionsDocument11 pagesForm 3 Chapter 1 QuestionsCheah Foo Kit50% (2)
- Lightening Organs of FishDocument22 pagesLightening Organs of FishHeer SheikhPas encore d'évaluation
- Respiratory Anatomy Comparison Green Leatherback Sea TurtlesDocument1 pageRespiratory Anatomy Comparison Green Leatherback Sea TurtlesAldinaPas encore d'évaluation
- Chest Tubes and ThoracentesisDocument18 pagesChest Tubes and ThoracentesisecleptosPas encore d'évaluation
- Neonatal 2Document37 pagesNeonatal 2Mateen Shukri100% (1)
- How animals survive and adapt to their environmentsDocument25 pagesHow animals survive and adapt to their environmentsLean Cristian LlobreraPas encore d'évaluation
- 3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsDocument35 pages3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsCharisma Tiara RessyaPas encore d'évaluation
- Jamb Biology Past Questions UnibenpagesDocument51 pagesJamb Biology Past Questions UnibenpagesEhigie promisePas encore d'évaluation
- Breathing Techniques For ExerciseDocument5 pagesBreathing Techniques For ExerciseHamilton DurantPas encore d'évaluation
- Nurse sees post-op appendectomy client first after endorsementDocument9 pagesNurse sees post-op appendectomy client first after endorsementMishia Renee EchonPas encore d'évaluation
- Disease ProjectDocument18 pagesDisease Projectapi-293515530Pas encore d'évaluation
- Respiratory Gas ExchangeDocument8 pagesRespiratory Gas ExchangeJohn SorianoPas encore d'évaluation
- Acute Respiratory Failure Pa Tho PhysiologyDocument4 pagesAcute Respiratory Failure Pa Tho Physiologyroseanne18100% (4)
- Respiratory System Insects 2Document4 pagesRespiratory System Insects 2KIPNGETICH FREDRICKPas encore d'évaluation
- ER RT ConsultDocument3 pagesER RT ConsultRobert BeatyPas encore d'évaluation
- Teaching Plan CopdDocument11 pagesTeaching Plan CopdMary Grace AgataPas encore d'évaluation