Vous aimerez peut-être aussi
- Medicine I Block Book FemaleDocument113 pagesMedicine I Block Book Femalecode-24Pas encore d'évaluation
- The Royal Victorian Eye and Ear Hospital AbbreviationsDocument7 pagesThe Royal Victorian Eye and Ear Hospital Abbreviationscode-24Pas encore d'évaluation
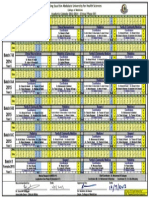
- Academic Calendar Phase III - 2013-2014Document1 pageAcademic Calendar Phase III - 2013-2014code-24Pas encore d'évaluation
- Hart of Dixie Episode Guide - Season 1 Recaps and ReviewsDocument1 pageHart of Dixie Episode Guide - Season 1 Recaps and Reviewscode-24Pas encore d'évaluation
- Antepartum HemorrhageDocument5 pagesAntepartum Hemorrhagecode-24Pas encore d'évaluation
- Skin DiseasesDocument5 pagesSkin Diseasescode-24Pas encore d'évaluation
- 2nd DraftDocument18 pages2nd Draftcode-24Pas encore d'évaluation
- KSAU-HS Female Med Student Participation Assessment FormDocument1 pageKSAU-HS Female Med Student Participation Assessment Formcode-24Pas encore d'évaluation
- Mentoring ProgramDocument1 pageMentoring Programcode-24Pas encore d'évaluation
- Access Medicine - TableDocument2 pagesAccess Medicine - Tablecode-24Pas encore d'évaluation
- Form UCE 10: Clinical Attachment Performance Feedback: DD MM DD MMDocument1 pageForm UCE 10: Clinical Attachment Performance Feedback: DD MM DD MMcode-24Pas encore d'évaluation
- 2-Year Pre-Professional Program Study Plan 2008Document5 pages2-Year Pre-Professional Program Study Plan 2008code-24Pas encore d'évaluation
- Access Medicine - Table (Hypo)Document3 pagesAccess Medicine - Table (Hypo)code-24Pas encore d'évaluation
- 12 Thediciton FINALDocument2 pages12 Thediciton FINALcode-24Pas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- (ATB) Is This Patient Allergic To Penicillin (JAMA)Document8 pages(ATB) Is This Patient Allergic To Penicillin (JAMA)api-3697245100% (1)
- Drug EruptionsDocument11 pagesDrug EruptionsAchmad Hariyanto100% (1)
- PPE-25-Case Report of Aquagenic UrticariaDocument2 pagesPPE-25-Case Report of Aquagenic UrticariaSajin AlexanderPas encore d'évaluation
- Nalco Varidos FSK: Cigweld Pty LTDDocument10 pagesNalco Varidos FSK: Cigweld Pty LTDPouria KazemzadehPas encore d'évaluation
- Drugs Affecting Respiratory SystemDocument19 pagesDrugs Affecting Respiratory SystemRuby Ann DimayugaPas encore d'évaluation
- Drug Class Review Antihistamine (Update 5,2010)Document72 pagesDrug Class Review Antihistamine (Update 5,2010)Supalerk KowinthanaphatPas encore d'évaluation
- Opioid AllergyDocument4 pagesOpioid AllergyJay100% (1)
- Transfusion ReactionsDocument28 pagesTransfusion ReactionsRovefrances ErpeluaPas encore d'évaluation
- New 4Document38 pagesNew 4rishi guptaPas encore d'évaluation
- Cernadas-2013-Pediatric Allergy and ImmunologyDocument7 pagesCernadas-2013-Pediatric Allergy and ImmunologyMoisés PoncePas encore d'évaluation
- Katzung - AutacoidsDocument23 pagesKatzung - AutacoidsKhairul AimanPas encore d'évaluation
- Allergic Skin DiseasesDocument20 pagesAllergic Skin DiseasesRicky ChanPas encore d'évaluation
- The Flushing PatientDocument35 pagesThe Flushing Patientliu_owen17Pas encore d'évaluation
- Chapter 2Document24 pagesChapter 2edward surtidoPas encore d'évaluation
- YÖKDİL/1/İNGİLİZCE/SAĞLIK BİLİMLERİDocument28 pagesYÖKDİL/1/İNGİLİZCE/SAĞLIK BİLİMLERİSüleyman DoğanPas encore d'évaluation
- Metrogyl: New Zealand Consumer Medicine InformationDocument4 pagesMetrogyl: New Zealand Consumer Medicine InformationAnbu KrishnanPas encore d'évaluation
- Urticaria 2Document11 pagesUrticaria 2ijaldo ajahPas encore d'évaluation
- Skinhairnail Ass 1Document43 pagesSkinhairnail Ass 1Airene Aquino BusaniaPas encore d'évaluation
- Doctor Guide to Managing HivesDocument2 pagesDoctor Guide to Managing HivesSunil RathiPas encore d'évaluation
- Healing Begins With Sanctification of The HeartDocument56 pagesHealing Begins With Sanctification of The HeartMwana WaChuma100% (2)
- Food Allergy - Indian ScenarioDocument28 pagesFood Allergy - Indian ScenarioAman BansalPas encore d'évaluation
- Drug Allergy VervloetDocument450 pagesDrug Allergy VervloetGuhaKrishnaswamy100% (1)
- Flutibact Skin OintmentDocument12 pagesFlutibact Skin OintmentSowndarya100% (1)
- UtricariaDocument2 pagesUtricariaaaathavanPas encore d'évaluation
- Alsangedy Bullets For Paces Angioedema 2nd EditionDocument2 pagesAlsangedy Bullets For Paces Angioedema 2nd EditionGhulamMemonPas encore d'évaluation
- Urtikaria & Angioedema: Melinda Rambing Kong 406148015 Pembimbing: Dr. Eko Krisnarto SP - KKDocument19 pagesUrtikaria & Angioedema: Melinda Rambing Kong 406148015 Pembimbing: Dr. Eko Krisnarto SP - KKMelinda KongPas encore d'évaluation
- Paediatric Dermatology (Notes)Document24 pagesPaediatric Dermatology (Notes)Ahmad Syarafi AbdullahPas encore d'évaluation
- Emergency NursingDocument56 pagesEmergency NursingNur SanaaniPas encore d'évaluation
- Chapter 18 Thermal Injuries (Student Copy)Document31 pagesChapter 18 Thermal Injuries (Student Copy)api-287615830Pas encore d'évaluation
- ALLERGIC REACTIONS TO CHEMOTHERAPYDocument23 pagesALLERGIC REACTIONS TO CHEMOTHERAPYAmbl GeronPas encore d'évaluation