Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Enterprise Risk Management Part 1Document37 pagesEnterprise Risk Management Part 1noelsugarPas encore d'évaluation
- Business Law Assignment - Question BDocument7 pagesBusiness Law Assignment - Question BAiman ArifPas encore d'évaluation
- Letter of CreditDocument34 pagesLetter of CreditpweelengPas encore d'évaluation
- Survey On Comparative Analysis of Max Life Online Term Plan Plus and ICICI Prudential IProtect Smart Plan PGDMDocument44 pagesSurvey On Comparative Analysis of Max Life Online Term Plan Plus and ICICI Prudential IProtect Smart Plan PGDMAlok kumarPas encore d'évaluation
- Build Own Operate Transfer (Boot) ProjectsDocument26 pagesBuild Own Operate Transfer (Boot) ProjectsMohammed Faiz100% (1)
- Sun Life Insurance v. CA and Emilio Tan G.R. No. 89741 (1991) FactsDocument1 pageSun Life Insurance v. CA and Emilio Tan G.R. No. 89741 (1991) FactsRod Ralph ZantuaPas encore d'évaluation
- OFR Report December2010Document15 pagesOFR Report December2010Neil GillespiePas encore d'évaluation
- Cal - Dot - Right of Way Manual - ch10Document332 pagesCal - Dot - Right of Way Manual - ch10prowagPas encore d'évaluation
- CV Rajesh GuptaDocument3 pagesCV Rajesh GuptaChandrasen GuptaPas encore d'évaluation
- Property AgreementDocument7 pagesProperty AgreementRocketLawyerPas encore d'évaluation
- Mii Pceia Ceilli ExaminationDocument8 pagesMii Pceia Ceilli Examinationgopalathevar sammuhomPas encore d'évaluation
- The First National Bank and Trust Company of Oklahoma City, Oklahoma v. United States Fidelity and Guaranty Company, A Corporation, and John Fawcett, 347 F.2d 945, 1st Cir. (1965)Document5 pagesThe First National Bank and Trust Company of Oklahoma City, Oklahoma v. United States Fidelity and Guaranty Company, A Corporation, and John Fawcett, 347 F.2d 945, 1st Cir. (1965)Scribd Government DocsPas encore d'évaluation
- Cases&Exercises - Chapter 3 - SolutionsDocument18 pagesCases&Exercises - Chapter 3 - SolutionsBarbara AraujoPas encore d'évaluation
- BIR RULING NO. OT-421-2021: Sun Life of Canada (Philippines), IncDocument6 pagesBIR RULING NO. OT-421-2021: Sun Life of Canada (Philippines), IncCarlota VillaromanPas encore d'évaluation
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument1 pageClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part AAnkitPas encore d'évaluation
- CÂU HỎI LÝ THUYẾT CUỐI KỲ TACN2Document32 pagesCÂU HỎI LÝ THUYẾT CUỐI KỲ TACN2K60 NGUYỄN XUÂN HOAPas encore d'évaluation
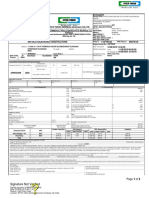
- Iffco-Tokio General Co - LTD: Signature Not VerifiedDocument3 pagesIffco-Tokio General Co - LTD: Signature Not VerifiedDMustNeed mvrPas encore d'évaluation
- Emergency Response Profile: ServproDocument30 pagesEmergency Response Profile: ServproEng Muhammad MarzoukPas encore d'évaluation
- Tax Invoice: KALPANA GAS AGENCY (0000125491)Document2 pagesTax Invoice: KALPANA GAS AGENCY (0000125491)Nithin ChandraPas encore d'évaluation
- IRS Pub 2194 - Disaster Relief Tax AddendumDocument136 pagesIRS Pub 2194 - Disaster Relief Tax AddendumdonlucekPas encore d'évaluation
- The Privatization of Roads and Highways - Walter BlockDocument494 pagesThe Privatization of Roads and Highways - Walter BlockMatt100% (3)
- Chapter 2Document58 pagesChapter 2addweb08Pas encore d'évaluation
- Payment of Indemnity Does Not Mean Owning Right of WayDocument2 pagesPayment of Indemnity Does Not Mean Owning Right of Wayyurets929Pas encore d'évaluation
- Chanakya National Law University: Extent of Insurer's Liability Under Motor Vehicles ActDocument19 pagesChanakya National Law University: Extent of Insurer's Liability Under Motor Vehicles ActSAURABH SUNNYPas encore d'évaluation
- Hull ClausesDocument28 pagesHull ClausesnigelctPas encore d'évaluation
- BIRMDocument2 pagesBIRMboazmashimbaPas encore d'évaluation
- Memorandum of AgreementDocument5 pagesMemorandum of AgreementMaria Lourdes P. GarciaPas encore d'évaluation
- Nara Introduction To Hsa SC Al 1Document11 pagesNara Introduction To Hsa SC Al 1api-293251883Pas encore d'évaluation
- March/April Edition of B2BDocument16 pagesMarch/April Edition of B2BWest Central TribunePas encore d'évaluation
- Preview PDFDocument6 pagesPreview PDFMATHANA SOORIA A/P ADEYAH MoePas encore d'évaluation