IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 4 Ver. VII (Apr. 2015), PP 01-05
www.iosrjournals.org
A 5 Year Histopathological Study of Skin Adnexal Tumors at a
Tertiary Care Hospital
Dr.Vani.D1, Dr.Ashwini.N.S2, Dr.Sandhya.M3, Dr.T.R.Dayananda4,
Dr.Bharathi.M5
1,2,3,5,
Department of Pathology, Mysore Medical College & Research Institute, Mysore, India
4,
Department of Dermatology, BGS Apollo Hospital, Mysore, India
Abstract:
Introduction: Skin adnexal neoplasms are uncommon and are daunting diagnostic problems in view of the
wide spectrum of lesions and their variants. Benign adnexal neoplasms are more common than malignant
lesions.
Aim: To study histopathology of skin adnexal neoplasms and to correlate with the clinical profile.
Methodology: 51cases with a diagnosis of skin adnexal neoplasm over a 5 year period reported in the
Department of Pathology, Mysore Medical College & Research Institute were included in the study.
Histopathological examination was done on Haematoxylin& Eosin stained slides and corroborated with special
stains wherever required.
Results: Skin adnexal tumors were most common in the age group of 40 to 49 years (21.56%, 11/51). Male to
female ratio was 1:1.68. The head and neck region was the most common site affected (64.70%, 33/51) with
39.21% (20/51) caseslocated on the face. 74.50% (38/51) cases were benign and 25.49% (13/51) cases were
malignant. The sweat gland tumors formed the largest group involving 43.13% (22/51) cases followed by the
hair follicle tumors 37.25% (19/51) followed by sebaceous gland tumors 19.60% (10/51). Nodular hidradenoma
was the most common benigntumor .Trichoblastic carcinoma and sebaceous carcinoma were the most frequent
malignant adnexal tumors in our study.
Conclusion: Histopathological examination is indispensable in the diagnosis of skin adnexal lesions owing to
their wide spectrum and frequency of differentiation along two different lines in the same lesion.
Keywords:Adnexal neoplasm, Histopathology, Skin
I.
Introduction
Skin adnexal tumours(SAT) are a large and diverse group of benign and malignant neoplasms which
exhibit morphological differentiation towards one of the different types of adnexal epithelium present in normal
skin:pilosebaeceousunit,eccrine and apocrine [1]. SAT are uncommon and pose major diagnostic problems to
both surgeons and pathologists [2]. SAT may display more than one line of differentiation (hybrid/composite
tumours), rendering precise classification of these neoplasms difficult [1].These tumours are derived from
multipotential undifferentiated cells present within the epidermis or its appendgeal structures and the histologic
features of a tumour are related to the activation of molecular pathways responsible for forming the mature
adnexal structures[3]. Most SAT are benign, but a malignant counterpart of every SAT has been described [1].
Malignant skin adnexal tumours are rare, locally aggressive and have the potential for nodal involvementand
distant metastasis with a poor clinical outcome. Therefore establishing a diagnosis of malignancy in SAT is
important for therapeutic and prognostic purposes [1].
II.
Materials And Methods
A blinded retrospective review of all skin adnexal neoplasms reported in the Department of Pathology
during the period 2010 to 2014 MMC&RI, Mysore, was done.51 cases were there in total.
Thehistopathologicalexamination was done on formalin fixed tissues and paraffin embedded blocks were made.
Haematoxylin &Eosin stained sections were examined and few special stains like PAS &reticulin were
performed wherever required.
III.
Results
In the present study, SAT were observed in all age groups ranging from 10 to 82 years. However, the
highest incidence was observed in the age group of 40 to 49 years (21.56%, 11/51) followed by age groups 5059 (17.64%, 9/51) and 70-79 years (17.64%, 9/51). The male:female ratio was 1:1.68. The head and neck region
was the most common site affected (64.70%, 33/51) followed by lower limb (15.68%, 8/51) and upper limb
(13.72%, 7/51). In head and neck region, 39.21% (20/51) were located on the face followed by 21.56% (11/51)
DOI: 10.9790/0853-14470105
www.iosrjournals.org
1 | Page
A 5 Year Histopathological Study Of Skin Adnexal Tumors At A Tertiary Care Hospital
over the scalp. The neck region was least affected accounting to 3.92% (2/51). Benign adnexal tumors
constituted 74.50% (38/51) cases and malignant adnexal tumors constituted 25.49% (13/51) cases. The sweat
gland tumors formed the largest group involving 43.13% (22/51) cases followed by the hair follicle tumors
37.25% (19/51) followed by sebaceous gland tumors 19.60% (10/51). The sweat gland tumors are composed of
nodular hidradenoma,
eccrineporoma, syringoscystadenomapapilliferum, apocrine hidrocystoma,
eccrinespiradenoma and cylindroma. Pilomatrixoma, trichoepithelioma, trichofilliculoma, porocarcinoma and
proliferating trichilemmal cyst with malignant transformation constituted the hair follicle tumors. Sebaceous
gland tumors are composed of sebaceous hyperplasia, sebaceousepithelioma and sebaceous
carcinoma.Syringocystadenomapapilliferum of eyelid, proliferating trichilemmal cyst with malignant
transformation, apocrine hidrocystoma and eccrinespiradenoma (Fig 1) were some of the rare tumors
encountered in our study. Amongst the benign tumors, nodular hidradenoma was the most common tumor
representing 15.78%, 6/38 cases. Trichoblastic carcinoma (30.76%, 4/13) and sebaceous carcinoma (30.76%,
4/13) were the most frequent malignant adnexal tumors in our study. Benign tumors were observed in age
ranging from 10-78 years and most of the malignant tumors were noted above 40 years of age.
IV.
Discussion
Adnexal tumors of the skin, though rare have been recognised from the later part of 19th century [4].
Skin adnexal neoplasms are an assorted group of tumours that show differentiation towards pilosebaceous,
eccrine or apocrine structures. Often they show evidence of more than one lineage within a single tumour.The
histogenesis of SAT are from either primary epithelial germ cells or pluripotential cells or cells of pre-existing
structure [5].Skin adnexal tumors have a wide range of age distribution. Ankit et al observed that commonest
age of presentation was 51-60 years whereas Radhika et al found third decade to be the most common age of
occurrence [3, 5]. However, in the present study, commonest age group was 41-50 years (21.56%) followed
closely by 51-60 years (17.64%).
Male: Female ratio was reported to be 1.07:1 by Ankit et al. In our study the male:female ratio was found to be
1:1.68 which was in concordance with Radhika et al, Nair et al and Saha et al.Ankit et al and Radhika et al
observed that head and neck region was the most common site of occurrence, which was also noted in our study
(62.24%) [3,5,6,7]
Incidence of benign tumours is moreas compared to malignant cases [3]. Benign tumours showed
smooth borders, absence of ulcers, presence of adnexae and absence of necrosis. Malignant tumours showed
ulcers, clefts between tumour cells and stroma and necrosis [2].The occurrence of benign tumors in our study
was 74.50% and 25.49% were malignant which was in tandem with studies of Radhika et al, Ankit et al, and
Samaila who reported 77.14%, 80.36%, and 88.5% benign and 29.63%, 19.64% and 11.5% malignant lesions
respectively [5, 3, 8].
Ankit et al and Nair et al observed that tumors of sweat gland differentiation were most common
followed by hair follicle tumors and then sebaceous glands tumors [3, 6]. The present study showed similar
results with sweat gland tumors constituting the largest group (43.13%), followed by hair follicle tumors(
37.25%) and sebaceous gland tumours (19.6%).
Nodular hidradenoma (Fig 2) was the most frequently encountered benign sweat gland tumor in the
present study. Similar observations were reported by Radhika et al and Ankit et al [5, 3].Histopathologically
most of these tumors are circumscribed and solid with few showing cystic change. Tumor is composed of
varying sizes of tubules and papillary projections lined by inner cuboidal and outer myeoepithelial cell layer.
Solid portions of the tumor showed nodules comprised of clear and polygonal cells [9].
Cylindroma was found to be the least common benign sweat gland tumor in our study. The tumor is
composed of irregularly shaped islands that are surrounded by hyaline sheath. Islands consist of two types of
epithelial cells: undifferentiated cells with small dark nuclei and cells with large pale nuclei representing certain
degree of differentiation towards ductal cells.
In the present study we reported four cases each of trichoblastic carcinoma and sebaceous carcinoma.
Histopathologicallytrichoblastic carcinoma (Fig 3) was comprised of islands of basaloid cells. These islands
demonstrated peripheral palisading surrounded by fibrocellularstroma. Basaloid cells exhibited cytological
atypia and brisk mitotic activity. Infiltration of underlying muscles was noted. Microscopically, sebaceous
carcinoma (Fig 4) revealed irregular epithelial lobules with an infiltrative growth pattern in the dermis. Lesional
cells demonstrated marked cytologicatypia, mitotic activity and focal sebaceous differentiation.
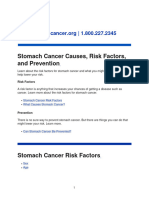
Syringocystadenomapapilleiferum (Fig 5) is a rare adnexal neoplasm, with eyelid being an even more
uncommon site. On microscopic examination, papillary projections with squamous epithelial lining and ductal
invaginations were obsereved. These ductal structures were lined by inner columnar and outer cuboidal cells [9].
There are only few studies from India and abroad describing in detail about the appendagealtumors of
the skin. We observed that adnexal tumors of skin appear to be relatively uncommon. Histopathological
DOI: 10.9790/0853-14470105
www.iosrjournals.org
2 | Page
A 5 Year Histopathological Study Of Skin Adnexal Tumors At A Tertiary Care Hospital
examination is the cornerstone in establishing the diagnosis of adnexal neoplasms in spite of expanding arsenal
of stem cell markers.
V.
Conclusion
Histopathological examination is indispensable in the diagnosis of skin adnexal neoplasms owing to
their wide spectrum and frequency of differentiation along two different lines in the same lesion. In spite of
being armed with volumes of literature, it is an intimidating task for the surgical pathologist to categorise them
correctly; especially so since they are uncommonly met with.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
K O Alsaad, N AObaidat, D Ghazarain, Skin adnexal neoplasms-part 1: An approach to tumours of pilosebaceous unit, J ClinPathol
2007; 60: 129:44
RTirumale, M O Roopa, Benign vs. Malignant Skin Adnexal Neoplasms: How Useful are Silhouettes? Indian Journal of
Dermatology, 58 (1), 2013
A Sharma, D G Paricharak, J S Nigam, S Rewri, P B Soni, A Omhare et al, Histopathological Study of Skin Adnexal TumoursInstitutional Study in South India, Journal of Skin Cancer 2014(2014)
M K Reddy, A J Veliath, S Nagarajan, A L Aurora, A clinicopathological study of adnexal tumours of skin, Indian J Med Res 75,
1982, 882-9
K Radhika, B V Phaneendra, N Rukmangadha, M K Reddy A biopsy confirmed skin adnexal tumours: experience at a tertiary care
teaching hospital, Journal of Scientific Research, 2, 2013, 132-138
P S Nair, A clinic-histopathological study of skin appendagealtumors, Indian Journal of Dermatology,Venerology and Leprology,
74 (550), 2008
A Saha, N K Das, R C Gharami, S N Chowdhury, P K Datta, A Clinico-histopathological study of appendageal skin tumors
affecting head and neck region in patients attending the dermatology opd of a tertiary care centre in eastern India, Indian J ournal of
Dermatology, 56, 2011, 33-36
M O A Samaila, Adnexal skin tumors in Zaria, Nigeria, Annals of African Medicine, 7(1), 2008, 6-10
W Klein, E Chan, J T Seykora, Tumors of epidermal appendages,DE Elder (Ed) Levers Histopathology of the Skin9thedn.
Philadelphia, PA: Lippincott Williams & Wilkins, 2005, 867-926.
Figure 1:Eccrinespiradenoma showing epithelial cells with large pale nuclei around small lumina and another
type of cells with small dark nuclei.
Figure 2 of Nodular hidradenoma showing bsaloidtumor cells with clear cytoplasm arranged in nodules
DOI: 10.9790/0853-14470105
www.iosrjournals.org
3 | Page
A 5 Year Histopathological Study Of Skin Adnexal Tumors At A Tertiary Care Hospital
Figure 3:Trichoblastic carcinoma composed of islands of basaloid cells showing cytologicatypia.
Figure 4: Sebaceous carcinoma showing small undifferentiated eosinophilic cells
Figure 5:Syringocystadenomapapilliferum showing epidermis with papillary projections and extending into
lumina of the cystic invaginations.
Table 1: Adnexal Tumors According To The Line Of Differentiation.
Sl No
1
2
3
Line of differentiation
Sweat gland tumors
Hair follicle tumors
Sebaceous gland tumors
Total
DOI: 10.9790/0853-14470105
No. Of cases
22
19
10
51
www.iosrjournals.org
Percentage incidence (%)
43.13
37.25
19.60
4 | Page
A 5 Year Histopathological Study Of Skin Adnexal Tumors At A Tertiary Care Hospital
Table 2: The Site And Sex Distribution Of Observed Adnexal Tumors
Sl No
1
2
3
4
Site of tumor
Head & Neck
Scalp
Face
Neck
Trunk
Upper limb
Lower limb
Total
Male
Female
Total
Percentage incidence (%)
6
7
1
1
2
2
19
5
13
1
2
5
6
32
11
20
2
3
7
8
51
21.56
39.21
3.92
5.88
13.72
15.68
100.00
Pie chart showing proportion of benign and malignant cases.
Table 3:Benign Adnexal Lesions In The Present Study
Sweat gland tumors
Nodular hidradenoma
Eccrineporoma
EccrineSpiradenoma
Acrospiroma
Cylindroma
SyringocystadenomaPappilliferum
Apocrine hidrocystoma
Total
No. of
cases
6
4
2
2
1
4
2
21
Hair follicle tumors
Pilomatrixoma
Trichoepithelioma
Trichoblastoma
Trichofolliculoma
No. of
cases
5
5
1
1
Sebaceous gland tumors
Sebaceous hyperplasia
Sebaceous epithelioma
Sebaceoma
12
No. of
cases
3
1
1
Table 4: Malignant Adnexal Tumors In The Present Study
Malignant adnexal tumors
Trichoblastic carcinoma
Porocarcinoma
Proliferating trichilemmal cyst with malignant transformation
Sebaceous carcinoma
Nodular hidradenoma with atypia
Malignant adnexal neoplasm (eccrine/apocrine)
No. Of cases
4
2
1
4
1
1
Bar diagram showing age distribution of cases of adnexal neoplasms.
DOI: 10.9790/0853-14470105
www.iosrjournals.org
5 | Page
Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Histopathology Specimens - Clinical, Pathological and Laboratory Aspects (PDFDrive)Document560 pagesHistopathology Specimens - Clinical, Pathological and Laboratory Aspects (PDFDrive)Xyrelle Navarro100% (2)
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDocument5 pages"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDocument7 pagesSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocument5 pagesAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Document15 pagesA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDocument6 pagesThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Assessment of The Implementation of Federal Character in Nigeria.Document5 pagesAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDocument7 pagesA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDocument7 pagesComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDocument4 pagesInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Impact of Technologies On Society: A ReviewDocument5 pagesThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDocument5 pagesEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDocument14 pagesAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDocument5 pagesDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalPas encore d'évaluation
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDocument7 pagesTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDocument5 pagesRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Importance of Mass Media in Communicating Health Messages: An AnalysisDocument6 pagesImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Role of Madarsa Education in Empowerment of Muslims in IndiaDocument6 pagesRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- SolidtumorsinchildrenDocument24 pagesSolidtumorsinchildrenPriyaPas encore d'évaluation
- Week 13 Cancer in Children Ncma219 Lec Midterm ReviewerDocument10 pagesWeek 13 Cancer in Children Ncma219 Lec Midterm ReviewerWynahPas encore d'évaluation
- Odontogenic Keratocyst: Submitted By: Digcha Shree Rai Roll No: 22Document31 pagesOdontogenic Keratocyst: Submitted By: Digcha Shree Rai Roll No: 22Rajat NangiaPas encore d'évaluation
- Choriocarcinoma 11Document23 pagesChoriocarcinoma 11Fakhir HasanPas encore d'évaluation
- FCM3-3.02 Philippine Cancer Control ProgramDocument11 pagesFCM3-3.02 Philippine Cancer Control ProgramJoher MendezPas encore d'évaluation
- Fibroids PowerpointDocument27 pagesFibroids Powerpointteritohaha100% (3)
- What Are PolypsDocument3 pagesWhat Are PolypsMicah PingawanPas encore d'évaluation
- SP ACCURE InjectablesDocument8 pagesSP ACCURE Injectablessanjay_gawaliPas encore d'évaluation
- 39 All Cancers Fact SheetDocument2 pages39 All Cancers Fact SheetSrinivas PingaliPas encore d'évaluation
- SOP CYTO UpdatedDocument39 pagesSOP CYTO UpdatedDEEPAK SINGH SANGWANPas encore d'évaluation
- ONCO 21 Desember 2020 Undiferentiated Pleomorfic Sarcoma Rev 1Document46 pagesONCO 21 Desember 2020 Undiferentiated Pleomorfic Sarcoma Rev 1ciptakarwanaPas encore d'évaluation
- The 2021 WHO Classification of TumorsDocument21 pagesThe 2021 WHO Classification of TumorsVamsi Krishna0% (1)
- Jadwal Pir MalangDocument4 pagesJadwal Pir MalangAbraham BayuPas encore d'évaluation
- Breast Cancer WHODocument104 pagesBreast Cancer WHOGoh Dody100% (2)
- NIH Public Access: Management of Endometrial PrecancersDocument22 pagesNIH Public Access: Management of Endometrial PrecancersmariePas encore d'évaluation
- A Rare Bladder Cancer - Small Cell Carcinoma: Review and UpdateDocument11 pagesA Rare Bladder Cancer - Small Cell Carcinoma: Review and UpdateIvan HoPas encore d'évaluation
- Mouth Cancer Information LeafletDocument2 pagesMouth Cancer Information LeafletmukeshrinkPas encore d'évaluation
- Bladder PDFDocument117 pagesBladder PDFimranqazi11Pas encore d'évaluation
- WCLC2017 Abstract Book WebDocument700 pagesWCLC2017 Abstract Book Webdavid.yb.wangPas encore d'évaluation
- Cancer Country Profile Indonesia-2020Document2 pagesCancer Country Profile Indonesia-2020Dwi AndayaniPas encore d'évaluation
- CDC Cervical Cancer Screening GuidelinesDocument2 pagesCDC Cervical Cancer Screening GuidelinesHumberto Camacho GonzalezPas encore d'évaluation
- TataDocument2 pagesTatavamsi NathPas encore d'évaluation
- Referat CA PancreasDocument25 pagesReferat CA PancreasPamela VasikhaPas encore d'évaluation
- Characterization of Adrenal Metastatic Cancer Using FDG PET CTDocument8 pagesCharacterization of Adrenal Metastatic Cancer Using FDG PET CTEngky ChristianPas encore d'évaluation
- Bone Tumors - Clues and CuesDocument97 pagesBone Tumors - Clues and CuesRhyRhye Sawitri AriantiPas encore d'évaluation
- Tracheobronchial LN EnlargementDocument6 pagesTracheobronchial LN EnlargementKarla FeliuPas encore d'évaluation
- Meigs Syndrome: Background: Meigs Syndrome Is Defined As The Triad of Benign OvarianDocument8 pagesMeigs Syndrome: Background: Meigs Syndrome Is Defined As The Triad of Benign OvarianRizki Amaliah100% (1)
- EAU EANM ESTRO ESUR ISUP SIOG Pocket On Prostate Cancer 2024Document40 pagesEAU EANM ESTRO ESUR ISUP SIOG Pocket On Prostate Cancer 2024nadaelhaousPas encore d'évaluation
- Stomach Cancer Causes, Risk Factors, and PreventionDocument15 pagesStomach Cancer Causes, Risk Factors, and PreventionJibba kamaraPas encore d'évaluation