Vous aimerez peut-être aussi
- Winter School Immuno Flyer 2020Document2 pagesWinter School Immuno Flyer 2020irdinamarchsyaPas encore d'évaluation
- Permintaan Lab Disertai Ket KlinisDocument1 pagePermintaan Lab Disertai Ket KlinisirdinamarchsyaPas encore d'évaluation
- Lab Result in EnglishDocument3 pagesLab Result in EnglishirdinamarchsyaPas encore d'évaluation
- Pre Training Discussion - BD FACSLyricDocument48 pagesPre Training Discussion - BD FACSLyricirdinamarchsyaPas encore d'évaluation
- 2021 Course Outline Operations Management Tutorial MTM C10Document5 pages2021 Course Outline Operations Management Tutorial MTM C10irdinamarchsyaPas encore d'évaluation
- Competency Are Your Staff Adequately TrainedDocument36 pagesCompetency Are Your Staff Adequately TrainedirdinamarchsyaPas encore d'évaluation
- Academic Program 2020Document2 pagesAcademic Program 2020irdinamarchsyaPas encore d'évaluation
- Audit ToolDocument1 pageAudit ToolirdinamarchsyaPas encore d'évaluation
- AACB Jill Tate ScholarshipDocument3 pagesAACB Jill Tate ScholarshipirdinamarchsyaPas encore d'évaluation
- Thesis Complete Uganda PDFDocument143 pagesThesis Complete Uganda PDFirdinamarchsyaPas encore d'évaluation
- Competency Are Your Staff Adequately TrainedDocument22 pagesCompetency Are Your Staff Adequately TrainedirdinamarchsyaPas encore d'évaluation
- Strengthening Regional Viral Hepatitis Laboratory CapacityDocument23 pagesStrengthening Regional Viral Hepatitis Laboratory CapacityirdinamarchsyaPas encore d'évaluation
- Competency Are Your Staff Adequately TrainedDocument22 pagesCompetency Are Your Staff Adequately TrainedirdinamarchsyaPas encore d'évaluation
- Manufacture of QCDocument19 pagesManufacture of QCirdinamarchsyaPas encore d'évaluation
- Physician health statement for employmentDocument1 pagePhysician health statement for employmentirdinamarchsyaPas encore d'évaluation
- The Challenges and Benefit of Internal Auditing PDFDocument27 pagesThe Challenges and Benefit of Internal Auditing PDFirdinamarchsyaPas encore d'évaluation
- BJSTR - Challenges in Early Infant Diagnosis of Beta ThalassemiaDocument4 pagesBJSTR - Challenges in Early Infant Diagnosis of Beta ThalassemiairdinamarchsyaPas encore d'évaluation
- Use of Genexpert For Clinically Suspected MDR TBDocument6 pagesUse of Genexpert For Clinically Suspected MDR TBirdinamarchsyaPas encore d'évaluation
- Antibiotik Yg Ada D RSKDDocument1 pageAntibiotik Yg Ada D RSKDirdinamarchsyaPas encore d'évaluation
- 01 - Current Draft WHO-CDC Biosafety RecommendationsDocument32 pages01 - Current Draft WHO-CDC Biosafety RecommendationsitsruriPas encore d'évaluation
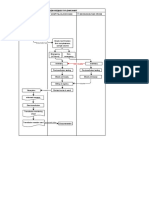
- Blood Request FlowchartDocument1 pageBlood Request FlowchartirdinamarchsyaPas encore d'évaluation
- Antibiotik Yg Ada D RSKD PDFDocument1 pageAntibiotik Yg Ada D RSKD PDFirdinamarchsyaPas encore d'évaluation
- Blood Transfusion: Teoman SOYSAL Prof. MDDocument38 pagesBlood Transfusion: Teoman SOYSAL Prof. MDirdinamarchsyaPas encore d'évaluation
- Uji Validasi Metode Tes Alat Hematologi Sysmex Xnl350Document1 pageUji Validasi Metode Tes Alat Hematologi Sysmex Xnl350irdinamarchsyaPas encore d'évaluation
- Bland and Altman Plots in ExcelDocument7 pagesBland and Altman Plots in ExcelirdinamarchsyaPas encore d'évaluation
- Malignant or Benign Leukocytosis: Tracy I. GeorgeDocument10 pagesMalignant or Benign Leukocytosis: Tracy I. GeorgeirdinamarchsyaPas encore d'évaluation
- TAT For Issuing Blood Products in EmergencyDocument4 pagesTAT For Issuing Blood Products in Emergencyirdinamarchsya100% (1)
- Hem Lect 12 ThalassemiaDocument48 pagesHem Lect 12 ThalassemiaKholisah MardiyahPas encore d'évaluation
- Prinsip Kerja MGITDocument6 pagesPrinsip Kerja MGITirdinamarchsyaPas encore d'évaluation
- Establishment of Reference Ranges For SPE in The Pediatric Population - A. FogliDocument1 pageEstablishment of Reference Ranges For SPE in The Pediatric Population - A. FogliirdinamarchsyaPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- CSEC Notes US in The CaribbeanDocument8 pagesCSEC Notes US in The Caribbeanvernon white100% (2)
- Row 1Document122 pagesRow 1abraha gebruPas encore d'évaluation
- Adjustment DisordersDocument2 pagesAdjustment DisordersIsabel CastilloPas encore d'évaluation
- The Human Element is Critical in Personal SellingDocument18 pagesThe Human Element is Critical in Personal SellingArsalan AhmedPas encore d'évaluation
- Andy Landers - Freeze Zone OffenseDocument6 pagesAndy Landers - Freeze Zone OffenseWinston Brown100% (1)
- Phantom Susan KayDocument379 pagesPhantom Susan Kaytheeyeofthemoon100% (9)
- Supplier Development at Honda, Nissan and ToyotaDocument28 pagesSupplier Development at Honda, Nissan and Toyotapresidonsi100% (1)
- PHILIPPINE INCOME TAX REVIEWERDocument99 pagesPHILIPPINE INCOME TAX REVIEWERquedan_socotPas encore d'évaluation
- OEO105020 LTE ERAN2.2 Connection Management Feature ISSUE 1.00Document52 pagesOEO105020 LTE ERAN2.2 Connection Management Feature ISSUE 1.00Daniel YulistianPas encore d'évaluation
- Speed of Sound and its Relationship with TemperatureDocument2 pagesSpeed of Sound and its Relationship with TemperatureBENNY CALLOPas encore d'évaluation
- Speakout Vocabulary Extra Advanced Unit 03Document3 pagesSpeakout Vocabulary Extra Advanced Unit 03shasha1982100% (2)
- Merry Almost Christmas - A Year With Frog and Toad (Harmonies)Document6 pagesMerry Almost Christmas - A Year With Frog and Toad (Harmonies)gmit92Pas encore d'évaluation
- The Republic of LOMAR Sovereignty and International LawDocument13 pagesThe Republic of LOMAR Sovereignty and International LawRoyalHouseofRA UruguayPas encore d'évaluation
- Cambridge Assessment International Education: Biology 5090/61 October/November 2017Document6 pagesCambridge Assessment International Education: Biology 5090/61 October/November 2017Zarish NoorPas encore d'évaluation
- Role of TaxationDocument5 pagesRole of TaxationCarlo Francis Palma100% (1)
- Di OutlineDocument81 pagesDi OutlineRobert E. BrannPas encore d'évaluation
- Japanese Tea Cups LessonDocument3 pagesJapanese Tea Cups Lessonapi-525048974Pas encore d'évaluation
- Islamic Finance in the UKDocument27 pagesIslamic Finance in the UKAli Can ERTÜRK (alicanerturk)Pas encore d'évaluation
- Unpacking of StandardsDocument41 pagesUnpacking of StandardsJealf Zenia Laborada CastroPas encore d'évaluation
- BCOM 302 BookDocument179 pagesBCOM 302 BookHitanshi AgarwalPas encore d'évaluation
- LumsDocument52 pagesLumsUmar AliPas encore d'évaluation
- Bhaktisiddhanta Appearance DayDocument5 pagesBhaktisiddhanta Appearance DaySanjeev NambalatePas encore d'évaluation
- BUMANGLAG - CLASS D - JEL PlanDocument3 pagesBUMANGLAG - CLASS D - JEL PlanMAUREEN BUMANGLAGPas encore d'évaluation
- H-1 Nationalism in Europe NotesDocument5 pagesH-1 Nationalism in Europe Noteskanishk kumarPas encore d'évaluation
- Bible Study RisksDocument6 pagesBible Study RisksVincentPas encore d'évaluation
- Raman Spectroscopy: 1 Theoretical BasisDocument9 pagesRaman Spectroscopy: 1 Theoretical BasisJèManziPas encore d'évaluation
- Sengoku WakthroughDocument139 pagesSengoku WakthroughferdinanadPas encore d'évaluation
- Jolly Phonics Teaching Reading and WritingDocument6 pagesJolly Phonics Teaching Reading and Writingmarcela33j5086100% (1)
- VDA ChinaDocument72 pagesVDA Chinatuananh1010Pas encore d'évaluation
- United States Court of Appeals, Sixth CircuitDocument5 pagesUnited States Court of Appeals, Sixth CircuitScribd Government DocsPas encore d'évaluation