Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Bone Turnover Markers in Epileptic PatientsDocument3 pagesBone Turnover Markers in Epileptic PatientskemalmiaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Management Dislipidemia PDFDocument5 pagesManagement Dislipidemia PDFkemalmiaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Guidance For Vitamin D Deficiency in ChildrenDocument3 pagesGuidance For Vitamin D Deficiency in ChildrenkemalmiaPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Vitamin D ImmunomodulatorDocument13 pagesVitamin D ImmunomodulatorkemalmiaPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Longitudinal Change of Vitamin D Status in ChildrenDocument7 pagesLongitudinal Change of Vitamin D Status in ChildrenkemalmiaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Long Term OAE Vitamin D Sri LankaDocument1 pageLong Term OAE Vitamin D Sri LankakemalmiaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Impact of Anti-Epileptic Drugs On Growth and PDFDocument22 pagesThe Impact of Anti-Epileptic Drugs On Growth and PDFkemalmiaPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Correction of Vitamin D Defi Ciency Improves Seizure Control in Epilepsy A Pilot StudyDocument3 pagesCorrection of Vitamin D Defi Ciency Improves Seizure Control in Epilepsy A Pilot StudykemalmiaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Influence of Drugs On Vitamin D and Calcium MetaboDocument10 pagesInfluence of Drugs On Vitamin D and Calcium MetabokemalmiaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Vitamin D: An Evidence-Based ReviewDocument9 pagesVitamin D: An Evidence-Based ReviewWill TohallinoPas encore d'évaluation
- Bone and Calcium Metabolism and Antiepileptic DrugsDocument10 pagesBone and Calcium Metabolism and Antiepileptic DrugskemalmiaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Adverse Metabolic Effects ofDocument13 pagesAdverse Metabolic Effects ofkemalmiaPas encore d'évaluation
- Altered Calcium Metabolism in Epileptic Children On AnticDocument3 pagesAltered Calcium Metabolism in Epileptic Children On AntickemalmiaPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Vitamin D: An Evidence-Based ReviewDocument9 pagesVitamin D: An Evidence-Based ReviewWill TohallinoPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Role of Various Vitamins in The Patients With EpilepsyDocument9 pagesRole of Various Vitamins in The Patients With EpilepsykemalmiaPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Stay Tuned To PXR An Orphan Actor ThatDocument3 pagesStay Tuned To PXR An Orphan Actor ThatkemalmiaPas encore d'évaluation
- Jci0421867 PDFDocument10 pagesJci0421867 PDFkemalmiaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Possible Involvement of Pregnane XDocument10 pagesPossible Involvement of Pregnane XkemalmiaPas encore d'évaluation
- Efficacy of Levamisole in Children With Frequently Relapsing andDocument3 pagesEfficacy of Levamisole in Children With Frequently Relapsing andkemalmiaPas encore d'évaluation
- Enzyme Induction With Antiepileptic DrugsDocument17 pagesEnzyme Induction With Antiepileptic DrugskemalmiaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- A Systematic Review of Pediatric ClinicalDocument21 pagesA Systematic Review of Pediatric ClinicalkemalmiaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Vitamin D Levels in Children and AdolescentsDocument5 pagesVitamin D Levels in Children and AdolescentskemalmiaPas encore d'évaluation
- Pharmacogenetics and PhenoDocument6 pagesPharmacogenetics and PhenokemalmiaPas encore d'évaluation
- Anti Epileptic Drugs and Osteoporosis December 2015 PDFDocument3 pagesAnti Epileptic Drugs and Osteoporosis December 2015 PDFkemalmiaPas encore d'évaluation
- Penyebab Glomerulonefritis AkutDocument11 pagesPenyebab Glomerulonefritis AkutkemalmiaPas encore d'évaluation
- Infeksi GnapsDocument9 pagesInfeksi GnapskemalmiaPas encore d'évaluation
- Jurnal Sindroma NefrotikDocument7 pagesJurnal Sindroma NefrotikkemalmiaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Sindroma NefrotikDocument5 pagesSindroma NefrotikkemalmiaPas encore d'évaluation
- PSGNDocument26 pagesPSGNMichael StevenPas encore d'évaluation
- Gnaps ThroatDocument7 pagesGnaps ThroatkemalmiaPas encore d'évaluation
- TMD List - RichardDocument30 pagesTMD List - Richardsheena PerezPas encore d'évaluation
- AbbreviationDocument84 pagesAbbreviationbettyquensiePas encore d'évaluation
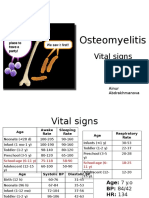
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaPas encore d'évaluation
- Pediatrics Review: Create Your Own E-LibraryDocument56 pagesPediatrics Review: Create Your Own E-LibraryL TPas encore d'évaluation
- Problems of The Neonate Low Birth Weight BabiesDocument25 pagesProblems of The Neonate Low Birth Weight BabiesmelbourneichrcPas encore d'évaluation
- Journey of The First 1000 Days 25 - 04 - 2018 For Web (Low Res) PDFDocument177 pagesJourney of The First 1000 Days 25 - 04 - 2018 For Web (Low Res) PDFchandraprakash_shuklPas encore d'évaluation
- Curriculum Vitae For Locum and JobDocument7 pagesCurriculum Vitae For Locum and JobrihihaPas encore d'évaluation
- InfertilitasDocument6 pagesInfertilitasmasdipoPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The VygonDocument2 pagesThe VygonDarpan Bhatt0% (1)
- Fields of Medicine: Clinical PracticeDocument9 pagesFields of Medicine: Clinical PracticeNorjetalexis Maningo CabreraPas encore d'évaluation
- Evaluacion de La Clase 8-1Document2 pagesEvaluacion de La Clase 8-1Carlitos J CosmePas encore d'évaluation
- 2010 Clinical Establishments (Registration and Regulation) Act, 2010Document15 pages2010 Clinical Establishments (Registration and Regulation) Act, 2010KakuPas encore d'évaluation
- Ophthalmia NeonatorumDocument5 pagesOphthalmia NeonatorumTeresa MontesPas encore d'évaluation
- 35-1404729796 JurnalDocument3 pages35-1404729796 JurnalNancy ZhangPas encore d'évaluation
- Circumcision PrsentationDocument34 pagesCircumcision PrsentationNitin KulkarniPas encore d'évaluation
- S2 Application FM-CSVlrd-01NEW 29july2016Document2 pagesS2 Application FM-CSVlrd-01NEW 29july2016Sherwin Anoba Cabutija100% (1)
- Hospital Design - AUHDocument108 pagesHospital Design - AUHDion LakonawaPas encore d'évaluation
- 2nd Year SyllabusDocument24 pages2nd Year Syllabuspraveen MPas encore d'évaluation
- Radiology in PeriodonticsDocument0 pageRadiology in PeriodonticsMohamed Abd El-Fattah GalalPas encore d'évaluation
- Hemodynamic Case Studies: Edward G. Hamaty JR., D.O. FACCP, FACOIDocument101 pagesHemodynamic Case Studies: Edward G. Hamaty JR., D.O. FACCP, FACOIrichard100% (1)
- Orthognathic SurgeryDocument72 pagesOrthognathic Surgeryrurinawangsari0% (1)
- Assessment of Growth and DevelopmentDocument29 pagesAssessment of Growth and DevelopmentKrupa JyothirmaiPas encore d'évaluation
- Allied HospitalDocument6 pagesAllied HospitalMalik Mubeen 007Pas encore d'évaluation
- Illegalization of Abortion in The PhilippinesDocument3 pagesIllegalization of Abortion in The PhilippinesLeo Jr MagbanuaPas encore d'évaluation
- Ixium Naha15 enDocument2 pagesIxium Naha15 enavabishay avapetrosPas encore d'évaluation
- CME Examination DermatologyDocument25 pagesCME Examination DermatologylimeddyPas encore d'évaluation
- ACOG Obesity in Pregnancy COREDocument15 pagesACOG Obesity in Pregnancy CORESaranya BalamuruganPas encore d'évaluation
- Anesthesiologists Manual of Surgical ProceduresDocument3 pagesAnesthesiologists Manual of Surgical ProceduresSheinGervacioErnacio0% (1)
- Pedia Platinum (1st Edition)Document546 pagesPedia Platinum (1st Edition)Mao Dela Cruz100% (4)
- Wards and Department in HospitalDocument11 pagesWards and Department in HospitalTias AstikaPas encore d'évaluation
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (26)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)