IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 5 Ver. III (May. 2015), PP 53-57
www.iosrjournals.org
Biochemical Changes in HIV Related Malnutrition in Children
Dr. G.Rajeswari 1*, Dr. P.Satya Gopal 1, Dr. E.Suresh2,
Dr. G.B.V.V.S.V.Prasad2
1*
Professor &HOD, Department of Biochemistry, Rangaraya Medical College, Kakinada.
1 Assistant Professor, Department of Pharmacology, Rangaraya Medical College, Kakinada.
2 Post Graduate, Departmentof Biochemistry, Rangaraya Medical College, Kakinada.
Abstract:
Background: Acquired Immune Deficiency Syndrome (AIDS) has become the most devastating disease
humankind has ever faced. An estimated 2.5 million children around the world are living with HIV/AIDs. As
HIV has many major complications in children, but main and important is malnutrition as children living
with HIV/AIDS face increased challenges in maintaining proper nutrition and also are anemic.
Aim: The aim of this study was to investigate serum Iron and TIBC changes and total proteins and cholesterol
in HIV malnourished children.
Materials and Methods: 100 HIV/AIDS children cases were compared with age and sex matched 50 normal
control groups for estimation of serum Iron, TIBC along with Total protein, Cholesterol,and data obtained was
statistically analyzed .
Results: Serum Iron was observed to be statistically decreased(p<0.0001)and TIBC is statistically
increased,and serum proteins and cholesterol also decreased significantly
Conclusion: Evaluation of Serum Iron and TIBC ,cholesterol and serum proteins in hiv children revealing of
intestinal malabsorption and also increased susceptibility of infection.
Key words: AIDS, TIBC, malnutrition, malabsorption
I.
Introduction
Acquired Immune Deficiency Syndrome (AIDS) has become the most devastating disease humankind
has ever faced. An estimated 2.5 million children around the world are living with HIV/AIDs, according to the
Joint United Nations Program on HIV/AIDS (JNAIDS) "2010 Report on the Global AIDS Epidemic."
Human immunodeficiency virus (HIV) is a lentivirus (a member of the retrovirus family) that causes acquired
immunodeficiency syndrome (AIDS),[1][2] a condition in humans in which progressive failure of the immune
system allows life-threatening opportunistic infections and cancers to thrive. HIV infection leads to low levels
of CD4+ T cells through three main mechanisms:
First, direct viral killing of infected cells; second, increased rates of apoptosis in infected cells; and
third, killing of infected CD4+ T cells by CD8 cytotoxic lymphocytes that recognize infected cells. When
CD4+ T cell numbers decline below a critical level, cell-mediated immunity is lost, and the body becomes
progressively more susceptible to opportunistic infections.
The World Health Organization (WHO) defines malnutrition as the cellular imbalance between the
supply of nutrients and energy and the bodys demand for them to ensuregrowth, maintenance, and specific
functions.Malnutrition is a medical condition caused by an improper or insufficient diet. [3] Malnutrition is
technically a category of diseases that includes: under nutrition, obesity and overweight, and micronutrient
deficiency among others.[4] However it is frequently used to mean just under nutrition from either
inadequate calories or inadequate specific dietary components for whatever reason. [3] The term "severe
malnutrition" is often used to refer specifically to protein-energy malnutrition.[5] Protein-energy malnutrition
(PEM) is often associated with micronutrient deficiency. [5] Two forms of protein-energy malnutrition are
kwashiorkor and marasmus, and they commonly coexist. [3]Kwashiorkor (displaced child) is mainly caused by
inadequate protein intake resulting in a low concentration of amino acids. [3] The main symptoms are edema,
wasting, liver enlargement, hypoalbuminaemia, steatosis, and possibly depigmentation of skin and
hair.[3] Kwashiorkor is identified by swelling of the extremities and belly, which is deceiving of actual
nutritional status.[6]
Marasmus (to waste away) is caused by an inadequate intake of both protein and energy. The main
symptoms are severe wasting, leaving little or no edema, minimal subcutaneous fat, severe muscle wasting, and
non-normal serum albumin.
People living with HIV/AIDS face increased challenges in maintaining proper nutrition. Despite
developments in medical treatment, nutrition remains a key component in managing this condition.
DOI: 10.9790/0853-14535357
www.iosrjournals.org
53 | Page
Biochemical Changes in HIV Related Malnutrition in Children
As well, the nutritional needs of people with HIV/AIDS are greater due to their immune system fighting
off opportunistic infections that do not normally cause disease in people with healthy immune
systems. Medication along with proper nutrition is a major component of maintaining good health and quality of
life for people living with HIV/AIDS.
Relationship between Nutrition and HIV/AIDS
o HIV infection impairs nutrient intake and absorption while increasing nutrient needs;
o The risks of opportunistic infections are increased with poor nutrition thus accelerating progression of HIV
into AIDS;
o The development of opportunistic infections reduce food intake leading to malnutrition in HIV;
o HIV/AIDS and malnutrition create a vicious cycle that eventually weakens the immune system.
HIV infected individuals have higher nutritional requirements than uninfected individuals, particularly
with regard to protein and energy. If they suffer from opportunistic infections, they are prone to loss of appetite,
even anorexia, thus reducing their dietary intake at the very time when requirements are higher. In addition, the
infection sometimes interferes with the body's ability to absorb food.Several factors constitute the component of
nutrition assessment. Nutrition assessment does not only mean physical measurements but also an understanding
of the clinical and lifestyle behaviours of the patient. They include the following:
Anthropometric measurements of body size or proportions (weight/, height, BMI, lean body mass, body
cell mass, skin-fold thickness, body circumference)
Biochemical assessment ( albumin, Haemoglobin, CD4, CD8 counts, micronutrients, serum proteins blood
sugar, lipids)
Clinical assessment (diarrhoea, nausea, vomiting, oral sores, dysphagia, odynophagia, fever, muscle
wasting, tuberculosis, anorexia, fatigue, lethargy, skin rashes)
Diet history/food availability (food access, utilization and handling, food supplementation, appetite, eating
patterns, medication,
Lifestyle: smoking, alcohol, physical activity, caffeine
Psychosocial factors: mood, social support systems
Biochemical Assessment
This assessment evaluates what nutrients are in a persons blood and whether the nutrients are within the normal
range or not. The commonly affected nutrients include,
Iron: measured as haemoglobin, which provides a total measure of the red blood cells. Depletion of iron is
associated with nutritional anaemia. Iron status is usually affected by infections such as malaria and
intestinal infections.
Serum albumin which is the bodys protector of blood volume and fluid electrolyte balance, any depletion
of albumin is associated with visceral protein impairment; this test can be used as a basic screen for
malnutrition. This nutrient is also affected by infection, where it will be lowered
Pre albumin: it also provides sensitive measure of visceral body protein
Other biochemical tests include: total fat, cholesterol, blood sugar and vitamins such as vitamin A, C, B
complex group.
II.
Aims And Objectives
Malnutrition is one of the major complications of HIV infection and a significant factor in advanced
disease.HIV infected individuals have higher nutritional requirements than uninfected individuals, particularly
with regard to protein and energy. If they suffer from opportunistic infections, they are prone to loss of
appetite, even anorexia, thus reducing their dietary intake at the very time when requirements are higher. In
addition, the infection sometimes interferes with the body's ability to absorb food. Except for a low protein or
low quality protein intake and chronic blood loss, patients canalso develop severe anaemia if there is a dietary
deficiency of iron, Children with malnutrition have decreased blood glucose, serum proteins and total
cholesterol levels.
Keeping this in view the Biochemical parameters were studied with the following objectives.
1. To study glucose, urea and creatinine concentrations in HIV malnourished children
2. To study Serum total proteins,albumin,globulins and A/G ratio in HIV malnourished children
3. To study Total cholesterol levels in HIV malnourished children
4. To study serum iron changes in HIV malnourished children
5. To study Total iron binding capacity ( TIBC) in HIV malnourished children
6. To compare the above parameters in HIV related malnutrition children with that of normal healthy children.
DOI: 10.9790/0853-14535357
www.iosrjournals.org
54 | Page
Biochemical Changes in HIV Related Malnutrition in Children
III.
Materials And Methods
The present study was conducted in the Department of Biochemistry, Rangaraya Medical College,
Kakinada, Andhra Pradesh, India. Study was undertaken to determine biochemical changes in HIV related
malnourished patients, in venous blood consisting of 100 patients. These values are compared with 50 normal
healthy children. All of these subjects were taken from ART centre OP. After taking consent, Blood samples
were obtained from Ante Cubital Vein of upper limbs of each patient. Control group were tested for HIV before
conducting tests and were found negative. Plasma was separated and analysed by using standard methods. All
data were expressed as mean + standard deviation. Studentt test paired two sample for means was used to
compare the values. Differences with a p value of less than 0.05 were considered to be statistically significant.
Biochemical analysis:
Blood samples were obtained from the subjects immediately after enrolment. Blood samples were
centrifuged at 2000 g for 10 min The samples were analyzed for Glucose, Urea, Creatinine, Total Cholesterol,
Total Proteins, Albumin, A/G ratio, Iron and TIBC are God-Pod , Urease , Alkaline picrate, Cod-Pod, Biuret ,
Bcg Dye, Ferrozine methods respectively.
IV.
Observation And Results
In the present study 100 HIV malnourished children and 50 normal healthy children below 13 years were
enrolled in case and control study.
Table-1: Levels of different Biochemical parameters in venous blood of malnourished children(< 13 years )
and control group. Mean SD
PARAMETER
GLUCOSE in mg/dl
UREA in mg/dl
CREATININE in mg/dl
TOTAL PROTEINS in g/dl
ALBUMIN in g/dl
CHOLESTEROL in mg/dl
IRON in g/dl
TIBC in g/dl
GLOBULINS in g/dl
A/G ratio
CONTROLS
(n=50)
100.12 17.27
16.32 4.14
0.778 0.243
6.322 0.259
3.196 0.219
153.50 16.38
95.12 18.17
304.22 39.88
3.129 0.263
0.990 0.140
CASES
(n=100)
61.67 19.24
17.88 5.07
0.822 0.246
5.169 0.863
2.642 0.607
90.18 15.91
41.67 12.11
450.53 103.05
2.527 0.70
1.116 0.533
p value
<0.0001*
NS
NS
<0.0001*
<0.0001*
<0.0001*
<0.0001*
<0.0001*
<0.0001*
NS
Figure 1: Bar diagram shows the values of serum toal protein and Albumin in controls and cases
DOI: 10.9790/0853-14535357
www.iosrjournals.org
55 | Page
Biochemical Changes in HIV Related Malnutrition in Children
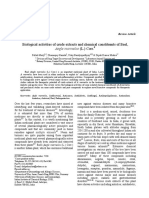
Figure 2: Bar diagram shows the values of serum Iron,TIBC, Cholesterol in controls and cases
V.
Discussion
The present study deals with the basic facts on the biochemical changes in HIV malnutrition in children.
Nutrition and HIV are strongly related to each other:
Any immune impairment as a result of HIV/AIDS leads to malnutrition, and malnutrition leads to
immune impairment, worsens the effect of HIV and contributes to more rapid progression to AIDS.
In the present study,the blood glucose levels are significantly decreased (p<0.0001)because of
decreased glucose absorption, hepatic glucose production, or increased glucose clearance.A fine balance
between EGP(Endogenous glucose production) and glucose clearance maintains blood glucose concentrations
[9]
. Decreased glucose production could be related to an impaired glucagon response, but it is not caused by
increased insulin secretion
Lower EGP could be caused by a decrease in glycogenolysis or
gluconeogenesis.Similar result had been given by Robert H J Bandsmaetal.[9]
Total proteins,albumin are significantly decreased(p<0.0001)decreased due to malabsorption
(insufficient intake and/or digestion of proteins) . This supports the notion that hypoalbuminemia indicates a
severe derangement in the child's metabolic system, reflecting a disturbance in protein metabolism, potentially
cytokine-mediated inhibition of albumin synthesis or alternatively cytokine-mediated capillary leak and
redistribution of albumin to the extravascular space and with increased oxidative stress. Whole-body protein
synthesis and breakdown are higher in malnourished children associated with HIV. Similar study had been done
by M J Manary, R L Broadheadetal[10,11]
Albumin was choosen as a marker of deterioration in the metabolic prole. The serum total protein,
albumin and serum A/G ratio were significantly lower in HIV malnutrition in children than control.When
comparison were done within the different grades of PEM associated with HIV, it was found that their A/G ratio
were changed but not significantly.Similar results were given by Rahman MZ, Begum BA.[11]
In my present study,total cholesterol is significantly reduced (p<0.0001)when compared with the
controls. The depression in the amount of total cholesterol was more marked in the severe forms of
undernutrition.Decreases in total cholesterol have been reported in the early stages of HIV-infection,being more
evident with decreasing CD4+lymphocytecountsa marker of disease progression showing a negative correlation
with TNF, TNF receptors, and IFN and disturbances in cholesterol metabolismThis is important for HIVinfection pathogenesis as HDL provides cholesterol for peripheral cells involved in the immune response and
tissue repair.[8]A similar result had been shown byLaura Maria D. da Silva etal.[8]
Common examples of secondary hypocholesterolemia include hyperthyroidism, various liver diseases,
HIV or AIDS and malnutrition.Decreased serum levels of albumin and cholesterol significantly correlated with
higher viral loads, lower CD4%, lower CD4:CD8, as well as stunting.
The important nutritional marker in HIV related malnutrition in children is Iron.
Serum iron levels are significantly decreased when compared to controls (p<0.0001) and it is related
to intestinal malabsorption .A similar study was conducted by Castaldoetal [11]
DOI: 10.9790/0853-14535357
www.iosrjournals.org
56 | Page
Biochemical Changes in HIV Related Malnutrition in Children
TIBC (total iron binding capacity)is significantly increased when compared to controls(p<0.0001).
Similar observations were made by Michael H. N. Goldenetal, Ulrich E. Schaibl, Stefan H. E. Kaufmann. When
infection is present and fever is observed, plasma concentrations of iron falls, causing hypoferraemia.[7]
Hypoferraemia causes changes in plasma concentrations of iron-binding proteins.
The iron-binding proteins help with the uptake of iron through the reticuloendothelial system or
through the removal and reutilization of hemoglobin from erythrocytes.
Children with human immunodeficiency virus (HIV) infection have a higher prevalence of intestinal
malabsorption. Anaemia is also a common feature in these children especially iron deficiency. Iron deficiency is
related to intestinal malabsorption.
VI.
Conclusion
This study was conducted in biochemical parameters in HIV malnourished children and normal
healthy children to know the differences if any, in the levels of plasma glucose, total proteins, albumin, A/G,
Total cholesterol, serum iron and TIBC in venous blood of HIV malnourished children as compared to control
group. The important nutritional marker in HIV related malnutrition in children is iron. The findings of present
study are as follows;
1. Plasma glucose concentrations, Serum total proteins , albumin and globulin levels, and total Cholesterol
levels are significantly decreased in HIV malnourished children when compared with the controls.
2. Serum Iron levels are significantly and statistically decreased in HIV malnourished children when
compared with the controls
3. TIBC levels are significantly and statistically increased in HIV malnourished children when compared with
the controls
4. Serum creatinine and urea showed no significance in HIV malnourished children when compared with the
controls.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
AIDS in the Twenty-First Century: Disease andGlobalization" by Tony Barnett and Alan Whiteside
Amadi B et al. Intestinal and systemic infection, HIV, and mortality in Zambian children with persistent diarrhea and
malnutrition. Journal of Pediatric Gastroenterology and Nutrition, 2001, 32(5):
Collins S, et al. Management of severe acute malnutrition in children. The Lancet, 2006, 368(9551):19922000.
Collins S, et al. Key issues in the success of community-based management of severe malnutrition. Food and Nutrition
Bulletin, 2006, 27(Suppl. 3):S4982.
Egger M, May M, Chene G et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative
analysis of prospective studies. Lancet 2002; 360: 119129.
Fawzi WW, Msamanga GI, Spiegelman D et al. A randomized trial of multivitamin supplements and HIV disease progression and
mortality. N Engl J Med 2004; 351: 2332.
Iron Deficiency and Intestinal Malabsorption in HIV Disease Castaldo, Annunziata; Tarallo, Luigi; Palomba, Elvia*; Albano, Fabio;
Russo, Stefania; Zuin, Giovanna; Buffardi, Floriana; Guarino, Alfredo
Lipid and Acute-Phase Protein Alterations in HIV-1 Infected Patients in the Early Stages of Infection: Correlation with CD4
ArcioTreitinger, CelsoSpada, Laura Maria D. da Silva, Clinical Analysis Department
Mechanisms Behind Decreased Endogenous Glucose Production in Malnourished ChildrenRobert H J Bandsma, Marijke Mendel,
Martijn N Spoelstra, Dirk-Jan Reijngoud
Serum and plasma markers of nutritional status in children infected with the human immunodeficiency virus.
Serum total protein, albumin and A/G ratio in different grades of protein energy malnutrition.Rahman MZ, Begum BA
DOI: 10.9790/0853-14535357
www.iosrjournals.org
57 | Page
Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDocument7 pagesSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDocument5 pages"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Assessment of The Implementation of Federal Character in Nigeria.Document5 pagesAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDocument14 pagesAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Document15 pagesA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDocument5 pagesRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDocument7 pagesA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocument5 pagesAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDocument6 pagesThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Impact of Technologies On Society: A ReviewDocument5 pagesThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDocument7 pagesComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDocument4 pagesInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Importance of Mass Media in Communicating Health Messages: An AnalysisDocument6 pagesImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDocument5 pagesEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Human Rights and Dalits: Different Strands in The DiscourseDocument5 pagesHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Lute Against Doping in SportDocument5 pagesThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationDocument3 pagesBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDocument7 pagesTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Role of Madarsa Education in Empowerment of Muslims in IndiaDocument6 pagesRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahDocument9 pagesClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsDocument6 pagesAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweDocument9 pagesTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationDocument6 pagesKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Women Empowerment Through Open and Distance Learning in ZimbabweDocument8 pagesWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweDocument8 pagesMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextDocument6 pagesDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaDocument11 pagesSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDocument5 pagesDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalPas encore d'évaluation
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaDocument3 pagesMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Study On The Television Programmes Popularity Among Chennai Urban WomenDocument7 pagesA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Diabetes Leader 2019 PDFDocument12 pagesDiabetes Leader 2019 PDFArjun Kumar AdhikariPas encore d'évaluation
- Blood Glucose Measurement by Sweat Using Arduino: K. Nivetha, N. Ramya, R. Thendral & A. GopikrishnanDocument8 pagesBlood Glucose Measurement by Sweat Using Arduino: K. Nivetha, N. Ramya, R. Thendral & A. GopikrishnanWael Abdelgadir AbdelazizPas encore d'évaluation
- Best Ayurvedic Medicine For Diabetes - Comparison & ReviewsDocument13 pagesBest Ayurvedic Medicine For Diabetes - Comparison & ReviewsSomanshu BanerjeePas encore d'évaluation
- The Ketogenic Diet & Managing Insulin ResistanceDocument2 pagesThe Ketogenic Diet & Managing Insulin ResistanceSaurabh Pandey0% (1)
- Gestational Diabetes Case Study With Questions For The Undergraduate NurseDocument46 pagesGestational Diabetes Case Study With Questions For The Undergraduate NurseAndrea Donmyer100% (1)
- Care Plan 3Document3 pagesCare Plan 3nyctotem50% (2)
- Vijaya Diagnostic Lab Test ResultsDocument10 pagesVijaya Diagnostic Lab Test ResultsRamaniPas encore d'évaluation
- Approach To Hypoglycemia in Infants and Children - UpToDateDocument20 pagesApproach To Hypoglycemia in Infants and Children - UpToDateDenny IntanPas encore d'évaluation
- IMO - Question Paper & Answer KeyDocument15 pagesIMO - Question Paper & Answer KeyDrAsish ParidaPas encore d'évaluation
- CHAPTER 10 SPECIAL PHLEBOTOMY AutosavedDocument104 pagesCHAPTER 10 SPECIAL PHLEBOTOMY AutosavedNorlyn Mae BihayPas encore d'évaluation
- Thornton 2015Document8 pagesThornton 2015Juan Antonio Herrera LealPas encore d'évaluation
- A Systematic Review On The Pre-Clinical Study of Cephalandra Indica and Gymnema Sylvestre in Diabetes Mellitus Type 2Document7 pagesA Systematic Review On The Pre-Clinical Study of Cephalandra Indica and Gymnema Sylvestre in Diabetes Mellitus Type 2International Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Gestational Diabetes MellitusDocument31 pagesGestational Diabetes MellitusJasmine PraveenPas encore d'évaluation
- Effects of Ingesting Highly Branched Cyclic DextrinDocument4 pagesEffects of Ingesting Highly Branched Cyclic DextrinLuis Castro XtrmPas encore d'évaluation
- Laboratory and DiagnosisDocument4 pagesLaboratory and DiagnosisHannah ChiuPas encore d'évaluation
- POC Testing in Lab Quality: Efficient Operation Combined With Convenient UseDocument2 pagesPOC Testing in Lab Quality: Efficient Operation Combined With Convenient UseMario RuizPas encore d'évaluation
- Biological Activities of Crude Extracts and Chemical Constituents of Aegle MarmelosDocument13 pagesBiological Activities of Crude Extracts and Chemical Constituents of Aegle MarmeloskavalapparaPas encore d'évaluation
- Nursing Care PlanDocument1 pageNursing Care PlanBtob meloPas encore d'évaluation
- Teaching Diabetes ManagementDocument5 pagesTeaching Diabetes ManagementWebster Claveria100% (5)
- Maternity Healthcare For Patients With Gestational DiabetesDocument59 pagesMaternity Healthcare For Patients With Gestational DiabetesManish MahajanPas encore d'évaluation
- 2016 Girraween High School HSC Biology Trial ExamDocument79 pages2016 Girraween High School HSC Biology Trial ExamArtemisPas encore d'évaluation
- Exercises To Lower Blood Sugar - LSDocument3 pagesExercises To Lower Blood Sugar - LSjferrell4380Pas encore d'évaluation
- Andrade, Ban, Salleva - Liver Cirrhosis - Objectives, Manifestations, Drug StudyDocument9 pagesAndrade, Ban, Salleva - Liver Cirrhosis - Objectives, Manifestations, Drug StudyWindi Dawn SallevaPas encore d'évaluation
- Case Analysis Format Final DraftDocument53 pagesCase Analysis Format Final DraftHannah Angelu CabadingPas encore d'évaluation
- Lab Report NewDocument8 pagesLab Report Newumeshsinghrajput1996Pas encore d'évaluation
- Journal of Ethnopharmacology: Trilobata (L.) Pruski Flower in RatsDocument7 pagesJournal of Ethnopharmacology: Trilobata (L.) Pruski Flower in RatsHeriansyah S1 FarmasiPas encore d'évaluation
- Hereditary Fructose IntoleranceDocument7 pagesHereditary Fructose Intolerancelucia galesPas encore d'évaluation
- Quiz 7. NCM 116 For StudentsDocument4 pagesQuiz 7. NCM 116 For StudentsZayne Lucas Gabrielle TadiamonPas encore d'évaluation
- Nursing Care Plan Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: Goat Was MetDocument4 pagesNursing Care Plan Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: Goat Was Metjeannezelle anne mariz gazaPas encore d'évaluation
- Diabetes PPT FinalDocument86 pagesDiabetes PPT FinalMohammed IbraheemPas encore d'évaluation