Vous aimerez peut-être aussi
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareD'EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CarePas encore d'évaluation
- Respiratory Virus Associated With Surgery in Children PatientsDocument11 pagesRespiratory Virus Associated With Surgery in Children PatientsJainah Rose Ferrer GubacPas encore d'évaluation
- Infants Hospitalized For Bordetella Pertussis Infection Commonly Have Respiratory Viral CoinfectionsDocument6 pagesInfants Hospitalized For Bordetella Pertussis Infection Commonly Have Respiratory Viral CoinfectionsYuscha AnindyaPas encore d'évaluation
- Human Rhinovirus/Enterovirus in Pediatric Acute Respiratory Distress SyndromeDocument6 pagesHuman Rhinovirus/Enterovirus in Pediatric Acute Respiratory Distress SyndromeMaudonlodPas encore d'évaluation
- Imas 11 01 35 PDFDocument4 pagesImas 11 01 35 PDFAkmal RifadliPas encore d'évaluation
- ARDSDocument9 pagesARDSrayalarasatitiPas encore d'évaluation
- An Observational Study of Febrile Seizures: The Importance of Viral Infection and ImmunizationDocument6 pagesAn Observational Study of Febrile Seizures: The Importance of Viral Infection and Immunizationnavali rahmaPas encore d'évaluation
- Hospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionDocument7 pagesHospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionadhitiaPas encore d'évaluation
- Epidemiology of Acute Respiratory Infections in Children in Guangzhou: A Three-Year StudyDocument9 pagesEpidemiology of Acute Respiratory Infections in Children in Guangzhou: A Three-Year Studywina annisaPas encore d'évaluation
- BronchiolitisDocument4 pagesBronchiolitisFlavia RochmanPas encore d'évaluation
- Is Virus Coinfection A Predictor of Severity in Children With Viral Respiratory Infections?Document6 pagesIs Virus Coinfection A Predictor of Severity in Children With Viral Respiratory Infections?castillocavazos09Pas encore d'évaluation
- Art05 PDFDocument7 pagesArt05 PDFPedroCastroAriasPas encore d'évaluation
- Vijay 2018Document6 pagesVijay 2018Rabiatul 'raney' AdawiyahPas encore d'évaluation
- Full TextDocument31 pagesFull TextkanPas encore d'évaluation
- Microbiological Evaluation of Nosocomial Infections by Using National Nosocomial Infection Surveillance (NNIS) SystemDocument13 pagesMicrobiological Evaluation of Nosocomial Infections by Using National Nosocomial Infection Surveillance (NNIS) SystemJanatinAzaPas encore d'évaluation
- Pediatrics 2009Document7 pagesPediatrics 2009sitnuciana_123Pas encore d'évaluation
- 2020 Article 5720Document7 pages2020 Article 5720DIEGO LOURENCO DOS SANTOS SILVAPas encore d'évaluation
- 90532100Document5 pages90532100Devi PuspasariPas encore d'évaluation
- Some Immunological Parameters of Viral Pediatric PneumoniaDocument8 pagesSome Immunological Parameters of Viral Pediatric PneumoniaTJPRC PublicationsPas encore d'évaluation
- Tugas Ipg UlfaDocument8 pagesTugas Ipg UlfaUlfa Mukhlisa Putri UlfaPas encore d'évaluation
- CCRP2016 9458230Document8 pagesCCRP2016 945823028121998Pas encore d'évaluation
- Corticosteroids in PARDSDocument6 pagesCorticosteroids in PARDSzendah123Pas encore d'évaluation
- Invasive Fungal Infections in Pediatric Oncology: MD MD MD MD MD MDDocument6 pagesInvasive Fungal Infections in Pediatric Oncology: MD MD MD MD MD MDerickmattosPas encore d'évaluation
- Evaluation and Significance of C-Reactive Protein in The Clinical Diagnosis of Severe PneumoniaDocument7 pagesEvaluation and Significance of C-Reactive Protein in The Clinical Diagnosis of Severe PneumoniaJhonathan Rueda VidartePas encore d'évaluation
- 2016 Article 645Document10 pages2016 Article 645Betharia TriayuPas encore d'évaluation
- Clinical Features of Respiratory Viral Infections Among Inpatients at A Major US Tertiary Care HospitalDocument9 pagesClinical Features of Respiratory Viral Infections Among Inpatients at A Major US Tertiary Care HospitalPaul JuanilloPas encore d'évaluation
- OutDocument8 pagesOutapi-284695722Pas encore d'évaluation
- MENINGITISVIRALESENADULTOSClinInfectDis 2008ihekwaba7839Document7 pagesMENINGITISVIRALESENADULTOSClinInfectDis 2008ihekwaba7839Michel VenegasPas encore d'évaluation
- Procalcitoninandcap PDFDocument10 pagesProcalcitoninandcap PDFmohd zonPas encore d'évaluation
- Researcharticle Open Access: Alexandra Hagen, Anna Eichinger, Melanie Meyer-Buehn, Tilmann Schober and Johannes HuebnerDocument10 pagesResearcharticle Open Access: Alexandra Hagen, Anna Eichinger, Melanie Meyer-Buehn, Tilmann Schober and Johannes HuebneramaliaPas encore d'évaluation
- Irv 12375Document6 pagesIrv 12375Marella DevinaPas encore d'évaluation
- Research Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal SepsisDocument7 pagesResearch Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal Sepsisflorentina lulutPas encore d'évaluation
- Predictive Value of Proteinuria in Adult Dengue SeverityDocument6 pagesPredictive Value of Proteinuria in Adult Dengue SeverityWindy SuryaPas encore d'évaluation
- 2016 Article 1849 PDFDocument8 pages2016 Article 1849 PDFdydy_7193Pas encore d'évaluation
- Wurzel 2016Document8 pagesWurzel 2016prolanis pkmmulyoharjoPas encore d'évaluation
- Vap NicuDocument8 pagesVap NicuWiwit ClimberPas encore d'évaluation
- Respiratory Tract Virus Infections in The Elderly With PneumoniaDocument11 pagesRespiratory Tract Virus Infections in The Elderly With PneumoniatanyasisPas encore d'évaluation
- Detection of Respiratory Syncytial Virus and Rhinovirus in Healthy InfantsDocument5 pagesDetection of Respiratory Syncytial Virus and Rhinovirus in Healthy Infants8502474Pas encore d'évaluation
- Ventilator AssociatedDocument18 pagesVentilator AssociatedAndry Wahyudi AgusPas encore d'évaluation
- Chest X-Ray Appearances in Pneumonia and BronchiolitisDocument7 pagesChest X-Ray Appearances in Pneumonia and BronchiolitisMariani AniPas encore d'évaluation
- Clinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaDocument6 pagesClinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaBobanBisercicPas encore d'évaluation
- Gittle R 2017Document4 pagesGittle R 2017Hari 'hardyboy' PurwantoPas encore d'évaluation
- Ne W Engl and Journal MedicineDocument8 pagesNe W Engl and Journal MedicineferPas encore d'évaluation
- BMJ c4978 FullDocument6 pagesBMJ c4978 Fulljesusm_115Pas encore d'évaluation
- PneumocystisDocument10 pagesPneumocystisJESSICA QUISPE HUASCOPas encore d'évaluation
- Journal PNTD 0001244Document10 pagesJournal PNTD 0001244Zulia Ahmad BurhaniPas encore d'évaluation
- Sépsis em Pacientes Neurovascular Focus On Infection and Sepsis in Intensive Care PatientsDocument3 pagesSépsis em Pacientes Neurovascular Focus On Infection and Sepsis in Intensive Care PatientsEdson MarquesPas encore d'évaluation
- Jurnal 6Document6 pagesJurnal 6Anonymous Us5v7C6QhPas encore d'évaluation
- The Burden of Respiratory Syncytial Virus Infection in Young ChildrenDocument11 pagesThe Burden of Respiratory Syncytial Virus Infection in Young ChildrenanggiPas encore d'évaluation
- Etiology of Acute Otitis Media in Children Less Than 5 Years of AgeDocument9 pagesEtiology of Acute Otitis Media in Children Less Than 5 Years of AgeadyPas encore d'évaluation
- A Clinical Scoring System For Pediatric Hand - Foot-Mouth DiseaseDocument8 pagesA Clinical Scoring System For Pediatric Hand - Foot-Mouth DiseaseclaudyPas encore d'évaluation
- Dengue Hemorrhagic Fever in Infants: A Study of Clinical and Cytokine ProfilesDocument12 pagesDengue Hemorrhagic Fever in Infants: A Study of Clinical and Cytokine ProfilesYono FabiandiPas encore d'évaluation
- IJP Volume 6 Issue 11 Pages 8507-8516Document10 pagesIJP Volume 6 Issue 11 Pages 8507-8516Marda LinaPas encore d'évaluation
- Articulo MicroDocument8 pagesArticulo Microliliana ospinaPas encore d'évaluation
- tmp7F77 TMPDocument9 pagestmp7F77 TMPFrontiersPas encore d'évaluation
- Revista MedicaDocument6 pagesRevista MedicaWilson LeccaPas encore d'évaluation
- 270 948 1 PBDocument8 pages270 948 1 PBindah96Pas encore d'évaluation
- 2015 Article 427Document6 pages2015 Article 427Chloe BujuoirPas encore d'évaluation
- Jurnal YuliaDocument8 pagesJurnal YuliaRayantiPas encore d'évaluation
- Childhood Community Acquired Pneumonia A Review of Etiology and Antimicrobial Treatment Studies.Document10 pagesChildhood Community Acquired Pneumonia A Review of Etiology and Antimicrobial Treatment Studies.Andry Wahyudi AgusPas encore d'évaluation
- Post-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasesDocument6 pagesPost-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasesSoniJfreePas encore d'évaluation
- Anesthetizing The Obese.1Document3 pagesAnesthetizing The Obese.1SoniJfreePas encore d'évaluation
- Airway Evaluation: Thin Sliced and Packaged: Randolph H. Hastings, MD, PHDDocument2 pagesAirway Evaluation: Thin Sliced and Packaged: Randolph H. Hastings, MD, PHDSoniJfreePas encore d'évaluation
- Problem AnalysisDocument2 pagesProblem AnalysisSoniJfreePas encore d'évaluation
- The Etiologies of non-CF Bronchiectasis in Childhood: A Systematic Review of 989 SubjectsDocument8 pagesThe Etiologies of non-CF Bronchiectasis in Childhood: A Systematic Review of 989 SubjectsSoniJfreePas encore d'évaluation
- Colistin For Lung Infection: An Update: Review Open AccessDocument12 pagesColistin For Lung Infection: An Update: Review Open AccessSoniJfreePas encore d'évaluation
- Pertussis Vaccination in Child Care Workers: Room For Improvement in Coverage, Policy and PracticeDocument5 pagesPertussis Vaccination in Child Care Workers: Room For Improvement in Coverage, Policy and PracticeSoniJfreePas encore d'évaluation
- Pertussis: Espid R RDocument2 pagesPertussis: Espid R RSoniJfreePas encore d'évaluation
- Social Justice, Climate Change, and Dengue: Aileen Y. Chang, Douglas O. Fuller, Olveen Carrasquillo, John C. BeierDocument12 pagesSocial Justice, Climate Change, and Dengue: Aileen Y. Chang, Douglas O. Fuller, Olveen Carrasquillo, John C. BeierSoniJfreePas encore d'évaluation
- ,swojwoDocument8 pages,swojwoSoniJfreePas encore d'évaluation
- Strategy Tester Report: EA Siluman Mirza AimanDocument7 pagesStrategy Tester Report: EA Siluman Mirza AimanSoniJfreePas encore d'évaluation
- KmshwirwjoewDocument7 pagesKmshwirwjoewSoniJfreePas encore d'évaluation
- GftydsrfjDocument11 pagesGftydsrfjSoniJfreePas encore d'évaluation
- BBBBBDocument11 pagesBBBBBAlfredo ErguetaPas encore d'évaluation
- Advanced MultisimDocument146 pagesAdvanced MultisimHec Itou75% (4)
- Flight Inspection of GAST D Approach and Taxi Guidance Systems - v1Document10 pagesFlight Inspection of GAST D Approach and Taxi Guidance Systems - v1Olivier LaylyPas encore d'évaluation
- Fuse Link KDocument6 pagesFuse Link KABam BambumPas encore d'évaluation
- KTM Tokamak Project. Present and Future Activity: January 2008Document9 pagesKTM Tokamak Project. Present and Future Activity: January 2008AB XEROXPas encore d'évaluation
- User AgentDocument2 pagesUser AgenthuongPas encore d'évaluation
- Fairwell TestDocument16 pagesFairwell TestSsekyanzi CalvinPas encore d'évaluation
- Engine Overhaul : Group 11BDocument80 pagesEngine Overhaul : Group 11BДмитрий100% (1)
- HW7 A SolutionsDocument6 pagesHW7 A Solutionsmmsingh91100% (1)
- Supertester 680 RDocument39 pagesSupertester 680 Rdomingos.sanchezPas encore d'évaluation
- Brochure Cementindustrie PfeifferDocument24 pagesBrochure Cementindustrie Pfeifferdoxa maria0% (1)
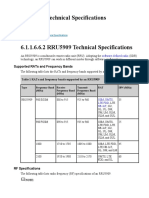
- RRU5909 Technical SpecificationsDocument7 pagesRRU5909 Technical SpecificationsDmitry059100% (1)
- Pedestrian Volume Studies: A Case Study in The City of GothenburgDocument80 pagesPedestrian Volume Studies: A Case Study in The City of GothenburgPaula A. FigueroaPas encore d'évaluation
- Onion Ring Magic SquareDocument8 pagesOnion Ring Magic SquareMJ Foust100% (2)
- Clinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFDocument12 pagesClinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFLuis Mochas HClPas encore d'évaluation
- Sequential Reliability TestsDocument2 pagesSequential Reliability Teststanpreet_makkadPas encore d'évaluation
- SMAC Actuators User ManualDocument52 pagesSMAC Actuators User ManualGabo DuarPas encore d'évaluation
- Latex ProjectDocument3 pagesLatex ProjectPrincess MiroPas encore d'évaluation
- NCERT Solutions For Class 12 Physics Chapter 12 AtomsDocument14 pagesNCERT Solutions For Class 12 Physics Chapter 12 AtomsKritika MishraPas encore d'évaluation
- KW Kwh/YrDocument3 pagesKW Kwh/YrHaris BaigPas encore d'évaluation
- QP NTSE Stage 1 2016 17 AndhraPradeshDocument27 pagesQP NTSE Stage 1 2016 17 AndhraPradeshsudhir_narang_3Pas encore d'évaluation
- Escape Velocity PDFDocument5 pagesEscape Velocity PDFRatriPas encore d'évaluation
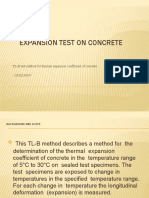
- Expansion Test of ConcreteDocument18 pagesExpansion Test of ConcreteAshokPas encore d'évaluation
- sbd0105 33 71 1BBE0 000011Document1 pagesbd0105 33 71 1BBE0 000011NetflixPas encore d'évaluation
- Crop Productivity Aroma Profile and Antioxidant Activity in Pelargonium Graveolens L-H-R Under inDocument7 pagesCrop Productivity Aroma Profile and Antioxidant Activity in Pelargonium Graveolens L-H-R Under inNo VivoPas encore d'évaluation
- Oracle Ebs InstallationDocument22 pagesOracle Ebs InstallationMr. JalilPas encore d'évaluation
- CEH PRACTICAL NOTES - Pratik KaranDocument23 pagesCEH PRACTICAL NOTES - Pratik Karanproton infosecPas encore d'évaluation
- Appendix 59.docx Inventory Custodian SlipDocument2 pagesAppendix 59.docx Inventory Custodian SlipJimmy CootPas encore d'évaluation
- Student Management SystemDocument5 pagesStudent Management SystemRamesh Kumar60% (5)
- Flatpack2 IntegratedDocument2 pagesFlatpack2 IntegratedNeil BailliePas encore d'évaluation