Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Complaint Against Waples Mobile Home ParkDocument32 pagesComplaint Against Waples Mobile Home Parkwamu885100% (2)
- HRM Individual Assignment-1Document3 pagesHRM Individual Assignment-1David LimPas encore d'évaluation
- Human Resource Planning: Job AnalysisDocument34 pagesHuman Resource Planning: Job AnalysisaidushPas encore d'évaluation
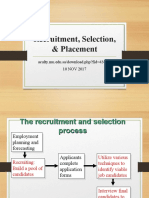
- Recruitment, Selection, & Placement: Aculty - Mu.edu - Sa/download - Php?fid 43097 10 NOV 2017Document33 pagesRecruitment, Selection, & Placement: Aculty - Mu.edu - Sa/download - Php?fid 43097 10 NOV 2017Anggi ArdhiastiPas encore d'évaluation
- Social Security in India - 2Document24 pagesSocial Security in India - 2Amitav TalukdarPas encore d'évaluation
- Corporate Training - The Education CoalitionDocument56 pagesCorporate Training - The Education CoalitionDayaPas encore d'évaluation
- SLR611S - Sports Law and Regulations - 1ST Opp - June 2022Document14 pagesSLR611S - Sports Law and Regulations - 1ST Opp - June 2022IsaiPas encore d'évaluation
- Rack Safety Inspection GuideDocument26 pagesRack Safety Inspection GuideFfttPas encore d'évaluation
- Nexus PMG 2022 WhitepaperDocument29 pagesNexus PMG 2022 Whitepapern.hartonoPas encore d'évaluation
- Business Communication: Raymond V. LesikarDocument23 pagesBusiness Communication: Raymond V. LesikarMahomuda AkterPas encore d'évaluation
- Job Evaluation MethodsDocument3 pagesJob Evaluation MethodsSasirekhaPas encore d'évaluation
- Nebosh Risk Assessment Sample Durka Nahendran Muthu Krishnan - 00510131Document11 pagesNebosh Risk Assessment Sample Durka Nahendran Muthu Krishnan - 00510131Mashael82% (11)
- Main Project CNGDocument14 pagesMain Project CNGmukaddimPas encore d'évaluation
- Performance ManagementDocument13 pagesPerformance ManagementHR AssigmnetsPas encore d'évaluation
- Experiences: 1. Introduce YourselfDocument2 pagesExperiences: 1. Introduce Yourselfmuhdfairuzzz muhammadfairuzzPas encore d'évaluation
- English B Paper 1 Guidelines and PracticeDocument87 pagesEnglish B Paper 1 Guidelines and Practicesarahworkspace111Pas encore d'évaluation
- Employee Handbook: Mission StatementDocument56 pagesEmployee Handbook: Mission StatementLedilyn MangaoangPas encore d'évaluation
- 2013 S2 Econ1016Document22 pages2013 S2 Econ1016Tom AfaPas encore d'évaluation
- Essay On WomenDocument5 pagesEssay On WomenkunalPas encore d'évaluation
- Teja G SDocument9 pagesTeja G Sinspire techPas encore d'évaluation
- Mini Case On Organizational BehaviorDocument3 pagesMini Case On Organizational BehaviorMd. Asif ZamanPas encore d'évaluation
- What Is International Human Trafficking?: Definitions and StatisticsDocument25 pagesWhat Is International Human Trafficking?: Definitions and StatisticsSuvedhya ReddyPas encore d'évaluation
- TN MIN WAGES REVISION EFFECTIVE 100719Document3 pagesTN MIN WAGES REVISION EFFECTIVE 100719GHANNESHPas encore d'évaluation
- Issue: Tiglao vs. Manila Railroad 98 Phil 181 Art. 1180, Setting of PeriodDocument4 pagesIssue: Tiglao vs. Manila Railroad 98 Phil 181 Art. 1180, Setting of PeriodLou StellarPas encore d'évaluation
- Introduction MidhunDocument86 pagesIntroduction MidhunVignesh VijayanPas encore d'évaluation
- Lease Telecom MDBAL0072 MervoDocument27 pagesLease Telecom MDBAL0072 MervoParents' Coalition of Montgomery County, MarylandPas encore d'évaluation
- United States Court of Appeals, Eleventh CircuitDocument12 pagesUnited States Court of Appeals, Eleventh CircuitScribd Government DocsPas encore d'évaluation
- Gloria M Goytia - VP MarketingDocument2 pagesGloria M Goytia - VP MarketinggmgoytiaPas encore d'évaluation
- I4 CT Students2019 PDFDocument127 pagesI4 CT Students2019 PDFEnrique ReynaPas encore d'évaluation
- Groups & Teams in OrganizationsDocument28 pagesGroups & Teams in OrganizationsVIBHOR JUNEJA EPGDIB On Campus 2022-23Pas encore d'évaluation