Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Revised Guidelines For Confirmed COVID-19 Cases 24012022Document4 pagesRevised Guidelines For Confirmed COVID-19 Cases 24012022Cezara ZahariaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Instructionsforself-Isolatingathome ClosecontactsDocument7 pagesInstructionsforself-Isolatingathome ClosecontactsCezara ZahariaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Phase-Answers To Citizens Enquiries - enDocument6 pagesPhase-Answers To Citizens Enquiries - enCezara ZahariaPas encore d'évaluation
- Metal Ceramic Dowel Crown RestorationsDocument4 pagesMetal Ceramic Dowel Crown RestorationsCezara ZahariaPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Family Welfare ProgrammeDocument19 pagesFamily Welfare ProgrammeMahesh Sahu100% (2)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Test 5 Answer KeyDocument4 pagesTest 5 Answer KeyEliPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- (Medical Specialty Board Review) George Williams, Navneet Grewal, Marc Popovich - Anesthesiology Critical Care Board Review (2019, Oxford University Press) PDFDocument217 pages(Medical Specialty Board Review) George Williams, Navneet Grewal, Marc Popovich - Anesthesiology Critical Care Board Review (2019, Oxford University Press) PDFLuís Irajá Nogueira De Sá NetoPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- OxytocinDocument1 pageOxytocinliam0831Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- ÔN TẬP TIẾNG ANH 1 CUỐI HPDocument14 pagesÔN TẬP TIẾNG ANH 1 CUỐI HPdty2357203010065Pas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Ancient Egyptian Temples Ancient Greece AsclepiusDocument5 pagesAncient Egyptian Temples Ancient Greece AsclepiusRana EhtishamPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
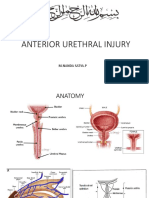
- Rupture Urethra Anterior DR Sule FixDocument36 pagesRupture Urethra Anterior DR Sule FixkadinfathiaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Project Report HospitalDocument90 pagesProject Report HospitalSaket ModiPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- FaicoDocument3 pagesFaicoknbabuPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- QA03005 Critical Testand Critical Result ReportingDocument7 pagesQA03005 Critical Testand Critical Result Reportingdebbie o. azcunaPas encore d'évaluation
- Concepts in NC II TESDA Certification ExaminationDocument5 pagesConcepts in NC II TESDA Certification ExaminationCon BernardinoPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- YASASII - Nursing ManualDocument20 pagesYASASII - Nursing ManualSalma Alsheikh AbdullahPas encore d'évaluation
- Lumbar PunctureDocument23 pagesLumbar Puncturemamoon100% (2)
- Maxillary Injection TechniquesDocument2 pagesMaxillary Injection Techniqueszuperzilch1676100% (4)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Masters in Medical Science - MMSCDocument12 pagesMasters in Medical Science - MMSCtexilaamericanPas encore d'évaluation
- Amnio InfusionDocument26 pagesAmnio InfusionMuhammad Harmen Reza SiregarPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- MCQ Sick NewbornDocument21 pagesMCQ Sick NewbornprabhatPas encore d'évaluation
- Stages of Labor and DeliveryDocument9 pagesStages of Labor and Deliverykhrysty1506Pas encore d'évaluation
- Correcting Forward HeadDocument64 pagesCorrecting Forward HeadPaul DoneyPas encore d'évaluation
- Ectopic Pregnancy - MedscapeDocument31 pagesEctopic Pregnancy - Medscapeantonio91uPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- المصادر المعتمدة في فرع تمريض الام والوليدDocument6 pagesالمصادر المعتمدة في فرع تمريض الام والوليدمنتظر عبدالعظيم عبدالله حميدPas encore d'évaluation
- Aural Haematoma and Its Surgical Management in Non Discript CatDocument3 pagesAural Haematoma and Its Surgical Management in Non Discript CatAnonymous 0PLXMqGcJ2Pas encore d'évaluation
- Principles of Endodontic SurgeryDocument29 pagesPrinciples of Endodontic SurgeryCristina Ene100% (3)
- Amra Rad 8Document3 pagesAmra Rad 8nikola-avramov-8934Pas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Medical Surgical Nursing Assignment - 2Document147 pagesMedical Surgical Nursing Assignment - 2Sonali Sengar0% (1)
- VAC Diversified FlowDocument1 pageVAC Diversified FlowWinnie AtienoPas encore d'évaluation
- Filed Under: Multifocal Atrial TachycardiaDocument3 pagesFiled Under: Multifocal Atrial TachycardiaBogdan TeoPas encore d'évaluation
- Perceptions and Beliefs Regarding Caesarean Section Among Pregnant Women Receiving Antenatal Care at Ishaka Adventist HospitalDocument12 pagesPerceptions and Beliefs Regarding Caesarean Section Among Pregnant Women Receiving Antenatal Care at Ishaka Adventist HospitalKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Kamus ICD 10 ICD 9Document59 pagesKamus ICD 10 ICD 9kiyoeugraPas encore d'évaluation
- 85 161 1 SMDocument3 pages85 161 1 SMvinay0717Pas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)