Vous aimerez peut-être aussi
- Bell Single-Sleeve Shrug Crochet PatternDocument2 pagesBell Single-Sleeve Shrug Crochet PatternsicksoxPas encore d'évaluation
- Clinical Obstetrics/Gynecology Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2D'EverandClinical Obstetrics/Gynecology Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Évaluation : 4 sur 5 étoiles4/5 (1)
- Preparation For MCAT Verbal ReasoningDocument88 pagesPreparation For MCAT Verbal ReasoningAishwarya Balasubramaniyan100% (3)
- CA-idms Ads Alive User Guide 15.0Document142 pagesCA-idms Ads Alive User Guide 15.0svdonthaPas encore d'évaluation
- AAFP QuestionsDocument509 pagesAAFP QuestionsAnchalia Chandrakumaran100% (3)
- Physiologycal Changes in PregnancyDocument66 pagesPhysiologycal Changes in PregnancyYulia RestyPas encore d'évaluation
- Combat Storm - Shipping ContainerDocument6 pagesCombat Storm - Shipping ContainermoiPas encore d'évaluation
- 1 - Maternal Physiological Changes During PregnancyDocument45 pages1 - Maternal Physiological Changes During PregnancyKholoud KholoudPas encore d'évaluation
- Physiological Changes During Pregnancy 2010Document42 pagesPhysiological Changes During Pregnancy 2010Asyhok Renault100% (1)
- Management of Pregnant Patient in DentistryDocument10 pagesManagement of Pregnant Patient in DentistryVíctor Orduña LópezPas encore d'évaluation
- Paso de Blas Lying in Clinic For NewDocument5 pagesPaso de Blas Lying in Clinic For NewNaheed Dean MustafaPas encore d'évaluation
- Practice Quiz Reflection Project Initiation and Key ComponentsDocument3 pagesPractice Quiz Reflection Project Initiation and Key ComponentsFalastin Tanani67% (3)
- Neonatal PolycythemiaDocument13 pagesNeonatal PolycythemiaMariel HuamancayoPas encore d'évaluation
- Physiology, Maternal Changes - StatPearls - NCBI Bookshelf PDFDocument5 pagesPhysiology, Maternal Changes - StatPearls - NCBI Bookshelf PDFAlejandro DiezPas encore d'évaluation
- Cambios Fisiologicos EmbarazoDocument23 pagesCambios Fisiologicos EmbarazoajanethPas encore d'évaluation
- Alterations in Physiology and Anatomy During Pregnancy PDFDocument12 pagesAlterations in Physiology and Anatomy During Pregnancy PDFAsh AmePas encore d'évaluation
- Maternal Adaptations To Pregnancy - Hematologic Changes - UpToDate PDFDocument27 pagesMaternal Adaptations To Pregnancy - Hematologic Changes - UpToDate PDFDiego Andres VasquezPas encore d'évaluation
- Shock and PregnancyDocument11 pagesShock and Pregnancy101 Andi Dwi Fahria.RPas encore d'évaluation
- Hematologic Changes in PregnancyDocument27 pagesHematologic Changes in PregnancySafinaz Inaz100% (1)
- Physiological Changes in Pregnancy - PMCDocument16 pagesPhysiological Changes in Pregnancy - PMCWidad SalsabilaPas encore d'évaluation
- Changes in PregnancyDocument9 pagesChanges in PregnancyFrankRodríguezLuisPas encore d'évaluation
- Physiology 212 Harrison AssignmentDocument3 pagesPhysiology 212 Harrison AssignmentHarrison RumePas encore d'évaluation
- Maternal Adaptations To PregnancyDocument12 pagesMaternal Adaptations To PregnancyTessa AcostaPas encore d'évaluation
- Definition:: Maternal Physiology During PregnancyDocument139 pagesDefinition:: Maternal Physiology During PregnancygibreilPas encore d'évaluation
- Maternal Adaptations To Pregnancy - Renal and Urinary Tract Physiology - UpToDateDocument9 pagesMaternal Adaptations To Pregnancy - Renal and Urinary Tract Physiology - UpToDateGrace TupiaPas encore d'évaluation
- Hematologic Changes in PregnancyDocument9 pagesHematologic Changes in PregnancyAlberto VelazquezPas encore d'évaluation
- Physiological Changes in Pregnancy: Candice K Silversides, Jack M ColmanDocument12 pagesPhysiological Changes in Pregnancy: Candice K Silversides, Jack M ColmanrinimeimeiPas encore d'évaluation
- OB I For 2nd YearDocument122 pagesOB I For 2nd YeardiribaPas encore d'évaluation
- Hematological Changes in Pregnancy The PreparatiDocument6 pagesHematological Changes in Pregnancy The Preparatiمحمد رحيم حسن محمودPas encore d'évaluation
- 1 s2.0 S2666668521001324 MainDocument5 pages1 s2.0 S2666668521001324 Mainmchojnacki81Pas encore d'évaluation
- CARDIOVASCULARDocument7 pagesCARDIOVASCULARyoungjbPas encore d'évaluation
- Obstetric AnesthesiaDocument31 pagesObstetric AnesthesiaChosenPas encore d'évaluation
- Reanimacion en La Paciente EmbarazadaDocument13 pagesReanimacion en La Paciente EmbarazadaJerry PowersPas encore d'évaluation
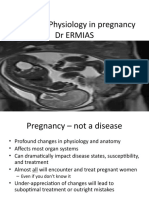
- Maternal Physiology in Pregnancy by ERMIDocument56 pagesMaternal Physiology in Pregnancy by ERMIHenok Y KebedePas encore d'évaluation
- Hematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, EthiopiaDocument7 pagesHematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, Ethiopiaade lydia br.siregarPas encore d'évaluation
- Maternal Physiology During PregnancyDocument60 pagesMaternal Physiology During PregnancySerge TresorPas encore d'évaluation
- Physiologic Changes of Pregnacy ADODocument55 pagesPhysiologic Changes of Pregnacy ADOTadesse MuhammedPas encore d'évaluation
- Resume Luar Negeri Dita FebriyantiDocument9 pagesResume Luar Negeri Dita FebriyantiDita FebriyantiPas encore d'évaluation
- Acute Abdomen in PregnancyDocument14 pagesAcute Abdomen in PregnancyNaila WardhanaPas encore d'évaluation
- Maternalphysiologylecture 091206194125 Phpapp01Document69 pagesMaternalphysiologylecture 091206194125 Phpapp01Ian Kirby Formeloza SolpicoPas encore d'évaluation
- Physiological Changes in Hematological Parameters During PregnancyDocument4 pagesPhysiological Changes in Hematological Parameters During PregnancyEva SihalohoPas encore d'évaluation
- Heart Disease and PregnancyDocument17 pagesHeart Disease and PregnancyDuy Nguyen CongPas encore d'évaluation
- Maternal Physiology and Complications of Multiple PregnancyDocument11 pagesMaternal Physiology and Complications of Multiple PregnancyFafaPas encore d'évaluation
- Normal PregnancyDocument150 pagesNormal Pregnancydevag0973Pas encore d'évaluation
- Thrombocytopenia in The Parturient: ReviewarticleDocument10 pagesThrombocytopenia in The Parturient: ReviewarticlesteffiesolinPas encore d'évaluation
- Presentor:-Sameeksha Sidhpuria Moderator: - Mrs. ANUPAMADocument69 pagesPresentor:-Sameeksha Sidhpuria Moderator: - Mrs. ANUPAMALakshmi PrasannaPas encore d'évaluation
- Preeclampsia: Clinical Features and DiagnosisDocument20 pagesPreeclampsia: Clinical Features and DiagnosisEdward VertizPas encore d'évaluation
- Physiologic Changes During Pregnancy and DeliveryDocument13 pagesPhysiologic Changes During Pregnancy and DeliveryBudi Khang100% (1)
- Physiological Changes in PregnancyDocument4 pagesPhysiological Changes in PregnancyMichimichi 78Pas encore d'évaluation
- Post Partum HemorrhageDocument10 pagesPost Partum HemorrhagedenekePas encore d'évaluation
- Pregnancy and Renal Function: Educational SupplementDocument3 pagesPregnancy and Renal Function: Educational SupplementIskandar HasanPas encore d'évaluation
- Critical Illness in Pregnancy Part I: An Approach To A Pregnant Patient in The ICU and Common Obstetric DisordersDocument12 pagesCritical Illness in Pregnancy Part I: An Approach To A Pregnant Patient in The ICU and Common Obstetric Disordersgustavo1rodriguesPas encore d'évaluation
- Physiological Changes in PregnancyDocument7 pagesPhysiological Changes in PregnancyFarid DjafarPas encore d'évaluation
- Hematological Changes Blood Volume: Figure 4-6Document12 pagesHematological Changes Blood Volume: Figure 4-6'aac' JujuuPas encore d'évaluation
- Physiologic Changes of PregnancyDocument8 pagesPhysiologic Changes of PregnancyAsteway MesfinPas encore d'évaluation
- Hematological Changes Blood Volume: Figure 4-6Document12 pagesHematological Changes Blood Volume: Figure 4-6'aac' JujuuPas encore d'évaluation
- Anesthesia in Pregnant Patients For Nonobstetric SurgeryDocument7 pagesAnesthesia in Pregnant Patients For Nonobstetric SurgeryBig TexPas encore d'évaluation
- Physiologic Changes During Normal Pregnancy and DeliveryDocument13 pagesPhysiologic Changes During Normal Pregnancy and DeliveryAlejandra RequesensPas encore d'évaluation
- Trauma Dalam KehamilanDocument6 pagesTrauma Dalam Kehamilaniin FzahroPas encore d'évaluation
- Fisiología en El Embarazo - Crit Care 2006Document7 pagesFisiología en El Embarazo - Crit Care 2006Fabiola Buelna GaxiolaPas encore d'évaluation
- Riñon y EmbarazoDocument20 pagesRiñon y EmbarazoMTZGEJPas encore d'évaluation
- 10.1007@s11906 020 01058 WDocument11 pages10.1007@s11906 020 01058 WMauricio Lopez MejiaPas encore d'évaluation
- Jcbfm2012210a PDFDocument14 pagesJcbfm2012210a PDFVenerandaPas encore d'évaluation
- Classification and Treatment of Ovarian Hyperstimulation SyndromeDocument7 pagesClassification and Treatment of Ovarian Hyperstimulation SyndromeGabo Bravo RodríguezPas encore d'évaluation
- Beers 2020 ACKD Kidney Physiology in PregnancyDocument6 pagesBeers 2020 ACKD Kidney Physiology in PregnancyBCR ABLPas encore d'évaluation
- Endoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokDocument37 pagesEndoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokMalavan MohammedPas encore d'évaluation
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionD'EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionPas encore d'évaluation
- Weill Cornell Medical College in Qatar: Week 18Document1 pageWeill Cornell Medical College in Qatar: Week 18Anchalia ChandrakumaranPas encore d'évaluation
- 2014Document10 pages2014Anchalia ChandrakumaranPas encore d'évaluation
- Autonomic DRUGSDocument25 pagesAutonomic DRUGSAnchalia ChandrakumaranPas encore d'évaluation
- Weill Cornell Medical College in Qatar: Week 1: AnesthesiaDocument1 pageWeill Cornell Medical College in Qatar: Week 1: AnesthesiaAnchalia ChandrakumaranPas encore d'évaluation
- LG 4Document2 pagesLG 4Anchalia ChandrakumaranPas encore d'évaluation
- Nri 3349Document13 pagesNri 3349Anchalia ChandrakumaranPas encore d'évaluation
- BOD Week 3 ScheduleDocument1 pageBOD Week 3 ScheduleAnchalia ChandrakumaranPas encore d'évaluation
- Weill Cornell Medical College in Qatar: Week 17: RheumatologyDocument1 pageWeill Cornell Medical College in Qatar: Week 17: RheumatologyAnchalia ChandrakumaranPas encore d'évaluation
- 2014Document10 pages2014Anchalia ChandrakumaranPas encore d'évaluation
- Kjim 29 281Document10 pagesKjim 29 281Anchalia ChandrakumaranPas encore d'évaluation
- Tissue Factor and Cancer Metastasis - The Role of Intracellular and Extracellular Signaling PathwaysDocument6 pagesTissue Factor and Cancer Metastasis - The Role of Intracellular and Extracellular Signaling PathwaysAnchalia ChandrakumaranPas encore d'évaluation
- MSK Path LabDocument1 pageMSK Path LabAnchalia ChandrakumaranPas encore d'évaluation
- E2559 FullDocument8 pagesE2559 FullAnchalia ChandrakumaranPas encore d'évaluation
- New CompDocument5 pagesNew CompAnchalia ChandrakumaranPas encore d'évaluation
- Amphiregulin Induces Tyrosine Phosphorylation of The Epidermal Growth Factor Receptor and p185Document8 pagesAmphiregulin Induces Tyrosine Phosphorylation of The Epidermal Growth Factor Receptor and p185Anchalia ChandrakumaranPas encore d'évaluation
- NK CellDocument11 pagesNK CellAnchalia ChandrakumaranPas encore d'évaluation
- DiagramDocument1 pageDiagramAnchalia ChandrakumaranPas encore d'évaluation
- Access Public File Serve 1Document10 pagesAccess Public File Serve 1Anchalia ChandrakumaranPas encore d'évaluation
- May 2013 SchedulesDocument72 pagesMay 2013 SchedulesAnchalia ChandrakumaranPas encore d'évaluation
- The Transcription Factor Fra-2 Promotes Mammary Tumour Progression by Changing The Adhesive Properties of Breast Cancer CellsDocument11 pagesThe Transcription Factor Fra-2 Promotes Mammary Tumour Progression by Changing The Adhesive Properties of Breast Cancer CellsAnchalia ChandrakumaranPas encore d'évaluation
- Raw TrackDocument8 pagesRaw TrackAnchalia ChandrakumaranPas encore d'évaluation
- 749 FTPDocument11 pages749 FTPAnchalia ChandrakumaranPas encore d'évaluation
- Gangliosides Expressed On Breast Cancer Cells Are E-Selectin LigandsDocument7 pagesGangliosides Expressed On Breast Cancer Cells Are E-Selectin LigandsAnchalia ChandrakumaranPas encore d'évaluation
- 8660406Document14 pages8660406Anchalia ChandrakumaranPas encore d'évaluation
- Cancer Res 2011 Julien 7683 93Document12 pagesCancer Res 2011 Julien 7683 93Anchalia ChandrakumaranPas encore d'évaluation
- The Transcription Factor Fra-2 Promotes Mammary Tumour Progression by Changing The Adhesive Properties of Breast Cancer CellsDocument11 pagesThe Transcription Factor Fra-2 Promotes Mammary Tumour Progression by Changing The Adhesive Properties of Breast Cancer CellsAnchalia ChandrakumaranPas encore d'évaluation
- 8660406Document14 pages8660406Anchalia ChandrakumaranPas encore d'évaluation
- Paper Format IJRDTDocument3 pagesPaper Format IJRDTrock starPas encore d'évaluation
- Trend in Agricultural ProductivityDocument1 pageTrend in Agricultural ProductivityGiaPas encore d'évaluation
- Panel Hospital List IGIDocument6 pagesPanel Hospital List IGIAbdul RahmanPas encore d'évaluation
- MT4 EA Installation Guide Digital - EnglishDocument7 pagesMT4 EA Installation Guide Digital - EnglishThe Trading PitPas encore d'évaluation
- Spike Magazine Cup PackDocument5 pagesSpike Magazine Cup PackBungle MarleyPas encore d'évaluation
- Gel Electrophoresis Worksheet Teacher AnswersDocument3 pagesGel Electrophoresis Worksheet Teacher AnswersChris FalokunPas encore d'évaluation
- No ApprovedDocument154 pagesNo ApprovedAnnaPas encore d'évaluation
- Hotel Voucher: Itinerary ID Hotel Santika Taman Mini Indonesia IndahDocument2 pagesHotel Voucher: Itinerary ID Hotel Santika Taman Mini Indonesia IndahSyukron PribadiPas encore d'évaluation
- English Assignment - October 6, 2020 - Group AssignmentDocument3 pagesEnglish Assignment - October 6, 2020 - Group AssignmentDaffa RaihanPas encore d'évaluation
- COSO DefinEDDocument21 pagesCOSO DefinEDRefdy AnugrahPas encore d'évaluation
- VDRL - Press. GaugesDocument9 pagesVDRL - Press. GaugesSourav RayPas encore d'évaluation
- Exam C - HANATEC142: SAP Certified Technology Associate - SAP HANA (Edition 2014)Document10 pagesExam C - HANATEC142: SAP Certified Technology Associate - SAP HANA (Edition 2014)SadishPas encore d'évaluation
- Tip Sheet March 2017Document2 pagesTip Sheet March 2017hoangvubui4632Pas encore d'évaluation
- Asme Bladder Accumulator DatasheetDocument3 pagesAsme Bladder Accumulator DatasheetSamad A BakarPas encore d'évaluation
- Engineering Mathematics Questions and AnswersDocument9 pagesEngineering Mathematics Questions and AnswersZaky Muzaffar100% (1)
- No Experience ResumeDocument2 pagesNo Experience ResumeNatalia PantojaPas encore d'évaluation
- Police Cranston School Committee Member Stole PTO FundsDocument1 pagePolice Cranston School Committee Member Stole PTO FundsashaydelinePas encore d'évaluation
- Epidemiological Triad of HIV/AIDS: AgentDocument8 pagesEpidemiological Triad of HIV/AIDS: AgentRakib HossainPas encore d'évaluation
- DD 3600 3500 3000 Parts CatalogDocument46 pagesDD 3600 3500 3000 Parts CatalogAndres Fdo Mora D100% (2)
- KirbyDocument3 pagesKirbyNorhassanah UtosabuayanPas encore d'évaluation
- Introduction To Object Oriented Database: Unit-IDocument67 pagesIntroduction To Object Oriented Database: Unit-Ipreetham rPas encore d'évaluation
- 7 ApportionmentDocument46 pages7 Apportionmentsass sofPas encore d'évaluation
- Job Sheet 1Document5 pagesJob Sheet 1Sue AzizPas encore d'évaluation
- SET UP Computer ServerDocument3 pagesSET UP Computer ServerRicHArdPas encore d'évaluation
- Bank OD Account in Tally 1Document3 pagesBank OD Account in Tally 1yashusahu180Pas encore d'évaluation