Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Piping FormulaeDocument9 pagesPiping FormulaeVashish RamrechaPas encore d'évaluation
- ISA SymbolsDocument1 pageISA SymbolsmustafasandikciPas encore d'évaluation
- Max Allowable Pressure of Pipes and Pipellines CER 04022013 1 (V. S. Kumar Unprotected)Document106 pagesMax Allowable Pressure of Pipes and Pipellines CER 04022013 1 (V. S. Kumar Unprotected)Vashish Ramrecha100% (1)
- Steel Beam BS 5950Document17 pagesSteel Beam BS 5950Vashish RamrechaPas encore d'évaluation
- In-Text: (Nickerson and Buist, 2008) Bibliography: Nickerson, D. and Buist, M. (2008) - Practical Application of Cellml 1.1: The IntegrationDocument1 pageIn-Text: (Nickerson and Buist, 2008) Bibliography: Nickerson, D. and Buist, M. (2008) - Practical Application of Cellml 1.1: The IntegrationVashish RamrechaPas encore d'évaluation
- Steel Cals SimpleDocument53 pagesSteel Cals SimpleVashish RamrechaPas encore d'évaluation
- Gantt ChartDocument6 pagesGantt ChartVashish RamrechaPas encore d'évaluation
- Development of A SemiDocument4 pagesDevelopment of A SemiVashish RamrechaPas encore d'évaluation
- Roll 2015Document26 pagesRoll 2015Vashish RamrechaPas encore d'évaluation
- Legacy ECSA ProfEng Appform TESDocument1 pageLegacy ECSA ProfEng Appform TESVashish RamrechaPas encore d'évaluation
- CH-4 Shells Under External PressureDocument64 pagesCH-4 Shells Under External PressureVashish RamrechaPas encore d'évaluation
- The Gurney Flap: A Case Study: 1.1 Issues in Wing DesignDocument9 pagesThe Gurney Flap: A Case Study: 1.1 Issues in Wing DesignVashish RamrechaPas encore d'évaluation
- E C S A: DeclarationDocument1 pageE C S A: DeclarationVashish RamrechaPas encore d'évaluation
- 4.2d - 4.6bDocument21 pages4.2d - 4.6bVashish RamrechaPas encore d'évaluation
- Nations Cup TimetableDocument60 pagesNations Cup TimetableVashish RamrechaPas encore d'évaluation
- Formula Sheet 2007Document3 pagesFormula Sheet 2007Vashish RamrechaPas encore d'évaluation
- Pressure-Volume Loops: Feasible For The Evaluation of Right Ventricular Function in An Experimental Model of Acute Pulmonary Regurgitation?Document6 pagesPressure-Volume Loops: Feasible For The Evaluation of Right Ventricular Function in An Experimental Model of Acute Pulmonary Regurgitation?Vashish RamrechaPas encore d'évaluation
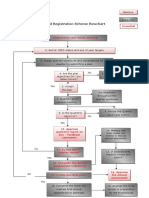
- SRS Flowchart of ProcessDocument1 pageSRS Flowchart of ProcessVashish RamrechaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- TroponinDocument39 pagesTroponinBayu AgastiaPas encore d'évaluation
- Fetal Circulation...Document2 pagesFetal Circulation...Ezra Dizon Manzano100% (1)
- Stroke Volume and Cardiac OutputDocument2 pagesStroke Volume and Cardiac OutputDennifer MadayagPas encore d'évaluation
- Cardiac TamponadeDocument6 pagesCardiac TamponadeVicky XiePas encore d'évaluation
- Circulation: Ms. Jonalyn P. SantosDocument18 pagesCirculation: Ms. Jonalyn P. SantosHoward John M. RamiterrePas encore d'évaluation
- Cardiovascular DrugsDocument6 pagesCardiovascular DrugsSilvio PerezPas encore d'évaluation
- SKILLS LAB 3 - CardiovascularDocument2 pagesSKILLS LAB 3 - CardiovascularJordiMarianoPas encore d'évaluation
- Hasil Tesis AdelaideDocument93 pagesHasil Tesis AdelaideAndi Alfian Zainuddin100% (1)
- Ayurveda in CADDocument3 pagesAyurveda in CADrajeevsonaliPas encore d'évaluation
- Heart SoundsDocument17 pagesHeart SoundsAlfrin Antony100% (3)
- What's The New of CPR?: Dr. Faisal Muchtar SP - An KIC SMF Anestesi Dan Intensive Care RS Wahidin Sudirohusodo MakassarDocument41 pagesWhat's The New of CPR?: Dr. Faisal Muchtar SP - An KIC SMF Anestesi Dan Intensive Care RS Wahidin Sudirohusodo MakassarfikranPas encore d'évaluation
- Histology of The Cardiac System: Dr. Nabil Khoury Anatomy DepartmentDocument51 pagesHistology of The Cardiac System: Dr. Nabil Khoury Anatomy DepartmentCzarina Aeri RollorataPas encore d'évaluation
- Cardiac Physiology MCQsDocument13 pagesCardiac Physiology MCQsالعراقي الصامد100% (2)
- AssignmentDocument4 pagesAssignmentDáńí KħâŋPas encore d'évaluation
- Heart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Document22 pagesHeart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Kenneth Jay EdnacoPas encore d'évaluation
- NEWS2 Chart 3 - NEWS Observation Chart - 0 PDFDocument1 pageNEWS2 Chart 3 - NEWS Observation Chart - 0 PDFKartini MedikalPas encore d'évaluation
- Peripheral Arterial DiseaseDocument32 pagesPeripheral Arterial DiseaseNiko YuandikaPas encore d'évaluation
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenPas encore d'évaluation
- Car&Ane&Pra&ASP&Sar&Gva&1 STDocument334 pagesCar&Ane&Pra&ASP&Sar&Gva&1 STAna Belén Artero CastañoPas encore d'évaluation
- Pulmonary EmbolismDocument93 pagesPulmonary EmbolismRakesh PanchalPas encore d'évaluation
- Congenital Heart Disease and Adolescence (2016, Springer International Publishing)Document235 pagesCongenital Heart Disease and Adolescence (2016, Springer International Publishing)paul00040Pas encore d'évaluation
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
- Criteria For The Diagnosis of Acute Myocardial InfarctionDocument20 pagesCriteria For The Diagnosis of Acute Myocardial InfarctionalexandraossesPas encore d'évaluation
- Pathophysiology of StrokeDocument22 pagesPathophysiology of StrokeKingman844100% (3)
- Differential Diagnosis of StrokeDocument2 pagesDifferential Diagnosis of Strokeamna_badar1Pas encore d'évaluation
- Effect of Early Physiotherapy in Coronary Artery Bypass Graft Surgery: A CaseDocument4 pagesEffect of Early Physiotherapy in Coronary Artery Bypass Graft Surgery: A CaseFitratun NajizahPas encore d'évaluation
- Rhythm Description Schematic Diagram Egc Characteristics Sample TraceDocument6 pagesRhythm Description Schematic Diagram Egc Characteristics Sample TraceJhenne Kyle Ko Dee100% (1)
- Pericardial Diseases: Dr. Abazie, Ugochi CDocument63 pagesPericardial Diseases: Dr. Abazie, Ugochi CUgochi AbaziePas encore d'évaluation
- Pharmacology For Nurses: The Islamic UniversityDocument118 pagesPharmacology For Nurses: The Islamic UniversityRojina AdhikariPas encore d'évaluation
- Guidelines For ICU Admission Discharge and TriageDocument18 pagesGuidelines For ICU Admission Discharge and TriageTika SartikaPas encore d'évaluation