Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Ophthalmology QuizDocument45 pagesOphthalmology QuizLana LocoPas encore d'évaluation
- Muscles of The EyeDocument3 pagesMuscles of The EyeAnna GarbiPas encore d'évaluation
- Correspondence: The Fishmouth Phenomenon in Retinal DetachmentDocument1 pageCorrespondence: The Fishmouth Phenomenon in Retinal DetachmentSushi HtetPas encore d'évaluation
- Ptosis: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanDocument13 pagesPtosis: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanAnonymous LnWIBo1GPas encore d'évaluation
- Refleksi Kasus BKMM-Benda Asing Di KonjungtivaDocument11 pagesRefleksi Kasus BKMM-Benda Asing Di KonjungtivaAnnisa Westania DanialPas encore d'évaluation
- Optic Nerve Disease, Papillaedema Optic Atropy, Visual FieldDocument31 pagesOptic Nerve Disease, Papillaedema Optic Atropy, Visual FieldsamxtraPas encore d'évaluation
- Use of Dyes in OphthalmologyDocument4 pagesUse of Dyes in OphthalmologyMaulana MalikPas encore d'évaluation
- InggrisDocument32 pagesInggrisRani Dwi HapsariPas encore d'évaluation
- Slitlampexaminationlecture 140828092025 Phpapp02Document100 pagesSlitlampexaminationlecture 140828092025 Phpapp02Anupama JanardhananPas encore d'évaluation
- Community Ophthalmology Int - L ClassDocument30 pagesCommunity Ophthalmology Int - L ClassaaPas encore d'évaluation
- 1.1 Statement of The Problem: Eye Care+ 1Document8 pages1.1 Statement of The Problem: Eye Care+ 1Walid Gee AbdulrahimPas encore d'évaluation
- Automated Direct Selective Laser Trabeculoplasty - First Prospective Clinical TrialDocument11 pagesAutomated Direct Selective Laser Trabeculoplasty - First Prospective Clinical TrialMasha DiBPas encore d'évaluation
- Clinical and Histological Presentation After Plexr Application, Needle Shaping (Vibrance) and O.F.FDocument9 pagesClinical and Histological Presentation After Plexr Application, Needle Shaping (Vibrance) and O.F.Falejandro GonzàlezPas encore d'évaluation
- Organic Chemistry Klein 2nd Edition Test BankDocument36 pagesOrganic Chemistry Klein 2nd Edition Test Bankattabaldigitulejp7tlPas encore d'évaluation
- Diagnosis and Management of Pseudoexfoliation Glaucoma - American Academy of Ophthalmology PDFDocument7 pagesDiagnosis and Management of Pseudoexfoliation Glaucoma - American Academy of Ophthalmology PDFnoviaPas encore d'évaluation
- Visual Field TestingDocument16 pagesVisual Field TestingHendry HuangPas encore d'évaluation
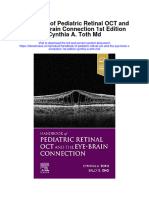
- Handbook of Pediatric Retinal Oct and The Eye Brain Connection 1St Edition Cynthia A Toth MD Full ChapterDocument67 pagesHandbook of Pediatric Retinal Oct and The Eye Brain Connection 1St Edition Cynthia A Toth MD Full Chapterpaul.grissom854100% (4)
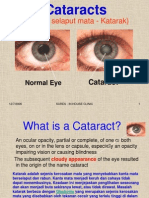
- Cataract and Eye Care DCaDocument26 pagesCataract and Eye Care DCaSamuil SumpalPas encore d'évaluation
- Infographic of Eye AnatomyDocument2 pagesInfographic of Eye AnatomyAshi RossPas encore d'évaluation
- Chalazion and Hordeolum (Stye) - Eye Disorders - Merck Manuals Professional EditionDocument3 pagesChalazion and Hordeolum (Stye) - Eye Disorders - Merck Manuals Professional EditionAlfina MeidinaPas encore d'évaluation
- Choice of Artificial Tear Formulation For Patients With Dry Eye: Where Do We Start?Document5 pagesChoice of Artificial Tear Formulation For Patients With Dry Eye: Where Do We Start?Priscila Verduzco100% (1)
- Comparison of Goldmann Applanation Tonometer, Tono-PenDocument19 pagesComparison of Goldmann Applanation Tonometer, Tono-PenLidiasilambaPas encore d'évaluation
- Ocular EmergencyDocument86 pagesOcular EmergencyMohammadPas encore d'évaluation
- MPSC Exams of Ophthalmology 3Document7 pagesMPSC Exams of Ophthalmology 3Hussein AliPas encore d'évaluation
- Life Sciences Grade 12 Term 3 Week 2 - 2020Document7 pagesLife Sciences Grade 12 Term 3 Week 2 - 2020paballorandomaccPas encore d'évaluation
- NCP GlaucomaDocument15 pagesNCP GlaucomaW'ton BorbePas encore d'évaluation
- 01.06.2017-Congenital Cataract Case Presentation-Dr - LikithaDocument32 pages01.06.2017-Congenital Cataract Case Presentation-Dr - Likithamuhammed fouadPas encore d'évaluation
- List of Thesis Topics in OphthalmologyDocument8 pagesList of Thesis Topics in Ophthalmologyalyssahaseanchorage100% (1)
- Ophthalmology UpdateDocument2 pagesOphthalmology UpdateskPas encore d'évaluation
- Oftalmologia - Apostila de Oftalmologia USP PDFDocument312 pagesOftalmologia - Apostila de Oftalmologia USP PDFRodrigo Mendes100% (1)